Provider and Staff Responses to Non-Facility Specific Patient Experience Feedback with Post-Acute Care Transitions
While a large portion of efforts related to improving patient experience, reducing medical errors, and improving clinical outcomes have focused on acute care settings, improvements in the quality of post-acute care and patient experience with transitions from general acute care settings to post-acute levels of care are key to accomplishing population health goals. While patient experience surveys are utilized nationwide, there is evidence of a need for deliberate efforts to create and implement recommendations derived from analyzing patient experience data with healthcare staff and providers. In 2019, 14 focus group sessions were conducted with providers and staff, including nursing, pharmacy, therapy, and case management from skilled nursing facilities, long-term acute care hospitals, and inpatient rehabilitation facilities. To minimize bias while studying reactions to patient comments regarding care transitions, participants from different facilities were placed into groups together and provided de-identified patient comments to review and discuss key themes and potential solutions. Attribution, discourse, and summative content analyses were performed to identify the key themes. A framework was developed to understand provider and staff reactions to non-facility-specific patient experience feedback as well as recommendations for improving post-acute care transitions.
Introduction
While a large portion of the funding and attention of healthcare industry professionals and regulatory agencies related to improving patient experience, reducing medical errors, and improving overall outcomes has focused on the inpatient setting, the quality of post-acute care and the patient experience with transitions from the general acute care setting to post-acute levels of care and eventually home are key for accomplishing population health goals such as readmission reduction. With the recent introduction of the novel coronavirus (COVID-19) impacting older individuals at a higher rate, the quality of post-acute care and the transitions from acute care facilities are especially crucial issues to consider. Healthcare administrators are challenged with the tasks of building interdisciplinary teams that can work collaboratively across settings and develop improved tools and strategies for improving patient-centered care.
Although patient experience surveys are used nationwide, there is evidence of a strong need for more deliberate efforts to create and implement recommendations derived from analyzing patient experience data with healthcare staff and providers [1]. Studies have also shown that while patients may vocally criticize their care in interviews and interactions, they may be reluctant to do so when completing written questionnaires, limiting the potential application of those written responses [1]. Providers and staff have been shown to suffer from data fatigue and frequently use an optimistic explanatory style when interpreting and responding to survey comments or documented patient concerns specific to their facilities and roles. One study reported that only 7% of providers receiving patient experience feedback considered the feedback in routinely adjusting and making improvements to their patient care and bedside manner [2].
Background
While several studies have involved focus groups of patients discussing general and specific patient experience feedback and concerns [3, 4], very few studies have coordinated large groups of providers and staff to discuss specific processes related to patient transitions in general, nonetheless those to post-acute care environments. This presents a gap in the existing research and an opportunity for health services researchers and students to broaden their understanding of patient, provider, and staff perspectives.
Recent studies have utilized other approaches to demonstrate mixed results related to the impact of programs designed to improve patient experience scores through the use of patient satisfaction data and targeted provider education programs. One study demonstrated the use of patient experience survey data and feedback by administrators conducting performance improvement “may promote, under certain circumstances, job dissatisfaction, attrition, and inappropriate clinical care among some physicians” [5]. According to Seiler, et al. simulation-based physician training on appropriate communication practices and techniques was not significantly associated with improvement in physician communication patient experience scores. Rather than attempting to alter perspectives or behaviors, this study endeavored to understand provider and staff perspectives reactions to patient comments within the framework of discourse analysis and gather information for the creation of post-acute care transition checklists.
Methods
Purpose of Study
In 2019, 14 focus group sessions were conducted with 87 providers and staff, including nursing, pharmacy, therapy, and case management from skilled nursing facilities, long- term acute care hospitals, and inpatient rehabilitation facilities (IRFs). The focus groups were designed to gather and document general reactions to shared type written patient experience comments and provide healthcare professionals with the opportunity to critically assess the concerns in the comments and propose solutions or tactics to address any problems or issues noted in the comments. While some studies have suggested that providers may at times be dismissive of patient complaints or constructive feedback when the feedback is directed toward their or their individual organization’s performance [2], this study endeavored to capture provider and staff reactions when provided with outside patient comments and feedback not specific to their own performance.
Research Questions
The study endeavored to answer the exploratory research question, “By providing de-identified non-provider specific patient experience feedback, will facilitators be able to engage providers in a proactive discussion regarding patient needs during post-acute care transitions and potential solutions to problems discussed and concerns voiced in the narrative comments?”. Additionally, the research team endeavored to detect and analyze patterns in provider and staff responses to patient experience comments in order to develop an improved understanding of how healthcare professionals respond to critical feedback and offer solutions. Once these aims were established, a focus group facilitation guide was created de novo and informed by the Strategic Framework for Improving Patient Experience in Hospitals [6] and recent research and literature on post-acute care transitions. The focus group tool was revised based on input from physicians, nurses, population health professionals, and qualitative research experts. The facilitation guide was pilot tested with a group of six providers and staff, edited, and appraised for face validity by qualitative methods experts in two California research organizations.
Focus Group Procedures
A total of 38 post-acute care facilities located in California participated in an initial cross-sectional study that collected survey data from patients, including self-reported experience scores with different aspects of post-acute care transitions, patient care, and care coordination. The survey also collected narrative comments from the patient and patient designee respondents that were then made available for review during the focus group sessions. A total of 5,349 confidential comments were collected from the combined 1264 surveys administered in 38 post-acute care facilities. Each of the 14 focus groups was conducted in 2019 and was composed of a different mixture of healthcare professionals from different facilities, including physician providers, advanced practice professionals (PA/NP), general nursing, pharmacy, therapy, and case management. However, in order to ensure the opportunity to thoroughly discuss patient care- related comments, every focus group included a minimum of one physician and one nursing staff member. Focus groups were held in a private meeting room at four different hospital sites. All participants provided written informed consent and agreed to be audio recorded in advance. Focus groups were conducted for 90 minutes and were facilitated by two facilitators, who were primary members of the research team.
To study provider and staff reactions to patient comments regarding post-acute care transitions while reducing the likelihood of bias, participants from different facilities were placed into groups together and provided de-identified (no patient or facility identifiers) written patient comments from three random facilities per group to review and discuss key themes and potential solutions. The focus groups were each provided with a smaller portion of four substantive positive comments related to post-acute care transitions to begin their discussion. Comments such as “Thank you!” were not included in the comments provided and any staff names provided in specific comments was removed. As an icebreaker for the sessions, the focus group participants were asked to review and react to the positive comments followed by a question for the group regarding when in their careers as healthcare professionals did they feel most appreciated: “Before we get started, reviewing the additional patient comments, let us consider and discuss when in your careers you felt most appreciated by patients and families similar to what we see reflected in these comments”.
Following the initial discussion regarding positive feedback, participant groups were each provided 12 specific comments regarding patient care or care coordination during post-acute care transitions that reflected some criticism or were labeled as not completely positive. These comments were collected as part of the post-acute care transition patient experience survey in response to seven items designed to collect narrative feedback. Figure 1 provides the specific questions used to solicit a wide range of comments from the 5,349 patient comments from which the sample of comments used for this study was drawn. The comments were sampled at random from a scrubbed dataset of 2,100 comments that contained constructive feedback across six different areas of patient concern.
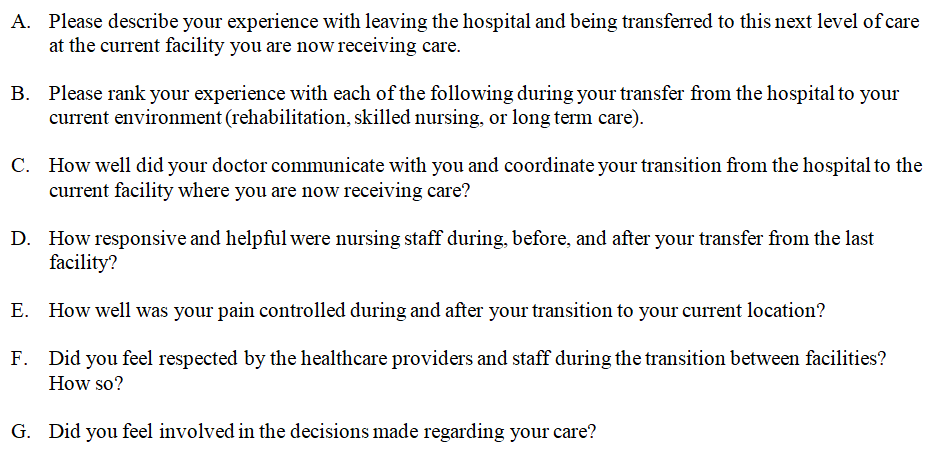
The comments utilized included different substantive patient concerns, primarily focused on one or some of the following issues: (1) patient and family involvement in care decisions, (2) timing and management of transfer processes, (3) pain management or medication consistency during/after transition, (4) nursing care, responsiveness, or hygiene concerns, (5) physician communication issues, and (6) frustrations related to inconsistencies in information sharing or duplication of forms/processes. To provide a balanced assortment of comments for discussion and avoid overloading any sensitive issues that might cause additional bias or discomfort for participants, two comments from each of the six subcategories were provided to each group. Not all comments were covered in every focus group session with some participants choosing to spend additional time discussing specific comments, similar examples from their own experiences working with patients, and potential strategies for mitigating or preventing specific patient concerns. Participants were asked to react openly to comments and share their initial thoughts when reading each comment. Participants were also asked to share where they felt most and least confident in their respective approaches and models of care, and where they believed the elements of their approaches could be considered best practice.
Coding
Initially, the researchers participated in focus group sessions and listened to recordings in order to understand the mood, context, and timing of comments with greater context. The two primary researchers then independently reviewed focus group transcripts and coded the focus group transcripts using manual methods in order to capture accurate results and reduce the likelihood of researcher bias impacting the coded data as a whole. The researchers identified common themes in responses across focus groups using inductive content analysis. The data were then reviewed to determine the agreement on the main themes. Four additional reviewers examined a sampling of 20 quotes each by providers and staff and matched each of the quotes with the corresponding theme identified by the team with a 100% accuracy rate.
Analysis
Attribution analysis and discourse analysis were performed to understand the participant reactions within the context of their roles as well as a summative content analysis to identify key themes around patient-centered care and interdisciplinary collaboration. Specifically, discourse analysis was utilized to explore three fundamental assumptions as they apply to patient experience with post- acute care transitions: (1) antirealism (provider, staff, and patients descriptions, including patient experience comments, cannot be deemed true or false portrayals of reality), (2) constructionism (how providers’ and staff’s constructs and boundaries are created and reinforced), and (3) reflexivity, including critical examinations of their roles and the impact of their viewpoint on their ability to express empathy toward patients and make meaningful improvements [7]. Discourse analysis provided the opportunity to understand provider and staff responses to patient experience comments regarding post-acute care transitions from the lens of their tendency to “situate each other with respect to social narratives and roles” [8]. Attribution analysis through the lens of semantical content analysis was used to identify primary themes in the focus group transcripts related, but not limited to, the posturing of responses, and the readiness to address patient concerns.
Results
While a variety of reactions were documented and problem solving and performance improvement-oriented discussions occurred during the focus group sessions, a total of nine general themes were identified using attribution analysis. The themes that emerged during the group discussions can be separated into two broad categories of provider reactions to post-acute care transitioned patient experience comments, including: (1) defensive factors and (2) problem solving and creative factors. Figure 2 illustrates the primary themes and explanatory styles identified in each category and illustrates the presence of defensive factors as a barrier to positive creative discussion around improving patient experience.
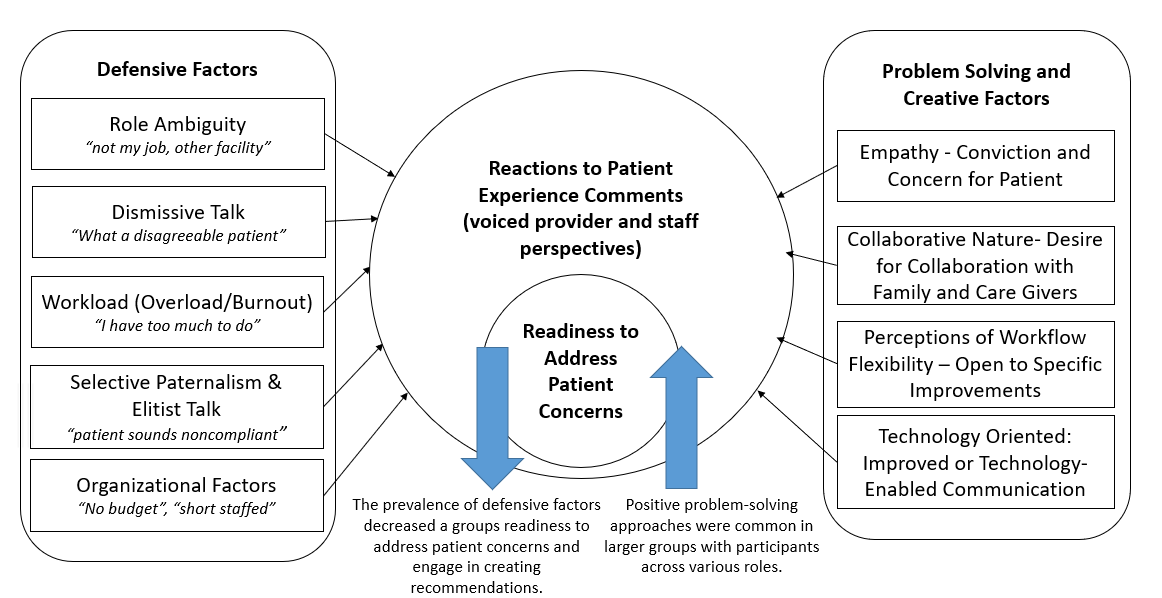
The design of this study included the use of comments from three random facilities in order to mitigate the potential for providers and staff to feel uncomfortable or personally accused as discussed in prior studies [5]. However, even though the comments were not directed towards the participants, the presence of defensive factors and the tendency of participants to work to excuse the behavior noted in individual negative comments was common in 11 of the 14 groups. The intention was to capture feedback from a range of roles and perspectives while embracing a “just culture” perspective and reducing discomfort by asking providers to respond to feedback from patients they likely never met or treated. These 11 groups spent a portion of their time empathizing with the perspective of the healthcare professionals involved, while often challenging the nature and validity of patient concerns. While providers and staff are valued members of the care team regardless of the use of defensive approaches, those who chose to rely on fewer defensive factors to rationalize, justify, or explain patient behavior were able to have more productive conversations that were more likely to end in specific recommendations regarding care improvements or strategies to prevent or mitigate the patient concerns discussed in the comments provided.
The five defensive factors observed included (1) reference to ambiguity in the roles and facility responsibilities during patient transfer, (2) dismissive talk and phrasing in which problems are minimized or avoided, (3) reference to workload limitations, tacit memory, and burnout, (4) selective paternalism and elitism based on shared assumptions that “the patient is not the expert and does not know what they need,” and (5) organizational factors such as a lack of financial and human resources. Creative factors included (1) empathy or concern for patients, (2) evidence of a collaborative nature, (3) openness to change and workflow revisions, and (4) positive perspectives on the use and integration of technology-based solutions in healthcare.
Limitations
There were several limitations in this study due to the nature of conducting focus groups with providers and staff in a facility environment. Given healthcare providers often work long hours and may not have an abundance of time to contribute to participate in a 90 minute focus group, volunteer bias based on the inclusion of individuals who readily made themselves available and were interested in the topic certainly could exist in the study [9]. While open dialogue and discussion was encouraged during the focus groups, this study also had a high risk of being impacted by acquiescence bias as well as social desirability bias as defined as “a tendency to present reality to align with what is perceived to be socially acceptable” [10]. Furthermore, it was observed that potential perceptions of the traditional hierarchy of healthcare professional roles may have impacted discussion with many of the perspectives being voiced on recordings coming from or being in agreement with the statements of physician participants. This could be evidence of hierarchical bias or a feature of the researchers’ choice to include multiple medical care-related concerns in the patient experience comments shared as prompts.
Another limitation was the inclusion of post-acute care staff members only, while participating physicians serving as attendees or physical medicine rehabilitation physicians in the post-acute environment have experience with multiple settings and possibly an understanding of transfer processes in both the acute and post-acute settings. Researchers may wish to consider incorporating nursing and case management staff from inpatient acute medical centers to join future conversations and contribute added perspectives. The researchers who had in-depth knowledge of the patient comments and feedback from the prior survey participated as facilitators and could have introduced a sympathetic bias into the conversation, thus creating a more collaborative and receptive environment than might exist otherwise. In retrospect, the study could have been strengthened through additional quantitative data collection. Specifically, an opportunity was missed to expand data collection and distribute a survey based tool to capture provider and staff self-reported receptivity to feedback by asking questions such as “On a scale of 1-5, how open are you to receiving feedback and constructive criticism.” or “Do you frequently incorporate patient and family feedback into your approach to delivering patient care.”
Discussion
A variety of themes were identified during the summative content analysis of the focus group transcripts, including ambiguity regarding facility and staff roles in the transition process, perceptions of lower resource availability in post-acute care settings, and hierarchical communication tendencies. However, additional attribution analysis revealed more prominent findings and led to the development of a model for understanding provider and staff reactions and perceptions based on (1) defensive factors and (2) problem- solving and creative factors. While these two groups of factors appear to be interrelated and a natural inverse of one another, the discussions revealed that both factors may be present in discussions allowing participants to initially react to the patient comments defensively and then complete a positive re-appraisal of the situation and discuss contributing factors to patient concerns and potential actions to mitigate those concerns.
Conclusion
The use of discourse analysis helped shape the interpretation of comments made by providers and staff regarding personal and organization-related defensive factors. When interpreted within the lens of organizational roles of provider, nursing, pharmacy, and care management, the volume of defensive and dismissive language increased when responding to comments related to the specific role or related processes. However, the potential for problem solving, solution generation, and positive framing also increased when a group comprised two or more individuals within the same role. For example, groups with two or more nursing staff members may have initially responded with defensive language when discussing a nursing- related patient comment; however, these groups also more frequently re-framed the discussion after a few moments and generated specific recommendations to address and/or prevent specific patient concerns.
Additionally, the provider and staff comments regarding specific challenges and resources required for successful post-acute care transfers led to the development of discharge checklists and recommendations for both transitions to and from various levels of post-acute care facilities and home care. Recommendations for future studies include the validation and customization of transfer checklists tailored based on the patient’s condition and destination.
Ethical and Research Considerations
This study was approved by the Institutional Review Board as a full-board review category research study. All participants were provided written informed consent. This project was not funded by any agency or organization, and there are no financial relationships to disclose.
References
-
Burt J, Campbell J, Abel G, Aboulghate A, Ahmed F, et al. (2017) Improving patient experience in primary care: a multimethod programme of research on the measurement and improvement of patient experience. NIHR Journals Library.
-
Rider EA, Perrin JM (2002) Performance Profiles: The Influence of Patient Satisfaction Data on Physicians’ Practice. Pediatrics 109(5): 752-757.
-
Rapport F, Hibbert P, Baysari M, Long JC, Seah R, et al. (2019) What do patients really want? An in-depth examination of patient experience in four Australian hospitals. BMC health services research 19(1): 38.
-
Sheff A, Park ER, Neagle M, Oreskovic NM (2017) The patient perspective: utilizing focus groups to inform care coordination for high-risk medicaid populations. BMC research notes 10(1): 315.
-
Zgierska A, Rabago D, MillerMM (2014) Impact of patient satisfaction ratings on physicians and clinical care. Patient preference and adherence 8: 437-446.
-
Birkelien NL (2017) A Strategic Framework for Improving the Patient Experience in Hospitals. Journal of healthcare management / American College of Healthcare Executives 62(4): 250-259.
-
Cowan S, Mcleod J (2004) Research methods: Discourse analysis. Counselling and Psychotherapy Research 4: 102-102.
-
Onwuegbuzie AJ, Dickinson WB, Leech NL, Zoran AG (2009) A Qualitative Framework for Collecting and Analyzing Data in Focus Group Research. International Journal of Qualitative Methods pp: 1-21.
-
Nyumba TO, Wilson K, Derrick CJ, Mukherjee N (2018) The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods in Ecology and Evaluation 9(1): 20-32.
-
Bergen N, Labonté R (2020) Everything Is Perfect, and We Have No Problems. Detecting and Limiting Social Desirability Bias in Qualitative Research. Qualitative Health Research 30(5): 783-792.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda