Evaluating Self-Reported Patient Experience with Transitions from General Acute Care to Post-Acute Care Settings
In collaboration with 18 inpatient rehabilitation hospitals (IRFs), six long term acute care hospitals, and 14 skilled nursing facilities, a cross-sectional study was conducted in which 1264 adult patients were surveyed regarding their experience with post-acute care transitions and coordination of care. Multiple research questions were explored, including potential relationships and differences in self-reported patient experience levels overall and across specific items as well as perceptions of patient-centered care provided by staff and providers. Exploratory factor analysis and multiple linear regression analysis were used to evaluate the grouping of questionnaire items and the relationship between these separate measures of transfer experience and overall patient experience. Analysis illustrated significant differences in mean reported patient experience with post-acute care transfers across destination settings (F (2, 1261) = 6.11, p< .001), indicating that patients reported higher experience scores when admitted to IRF settings (m = 4.31, SD=1.5) than when admitted to other long term care settings (m = 3.10, SD = 1.1). The adjusted R square of 0.536 (p<0.001) indicated that the individual experience categories, such as dignity and respect and provider communication, account for more than half of the explained variation in overall patient experience with transitions to long term care environments.
Introduction
A variety of models of care and current reimbursement mechanisms have shaped the manner in which post-acute care is delivered and patients are transferred to lower levels of care following inpatient hospitalizations. Understanding the key factors that contribute to successful transitions, reduced readmissions, and patient-centered care is crucial to the development of best practices in post-acute care environments. Post-acute care transitions represent a key area of opportunity for improving patient satisfaction and care coordination [1]. As patients leave the acute care facilities and embark upon their rehabilitation (IRF), skilled nursing (SNF), or long term acute care (LTAC) stays, a new care team of providers and staff as well as concerned family members all need to be informed of their care and feel included in care plan decisions and the selection of that next destination. Using proactive approaches to assessing patient experience and identifying barriers to successful patient and provider communication during discharge transitions is critical for the effective management of populations [2]. While a 2015 study illustrated the potential for planning for transitions to post-acute care to receive less staff time and attention compared to discharge planning for “home with self-care” discharges, the proportion of acute medical center hospitalizations resulting in discharges to post-acute care facilities has actually increased by a relative increase of 49% from 9.2% of discharges in 1996 to 13.7% in 2010 [3]. In addition to a higher percentage of discharged patients being cared for in post-acute environments, patients discharged to those environments are at risk for adverse outcomes including a relatively high likelihood of experiencing a readmission within 30 days. A comprehensive review of claims of a large cohort of Medicare fee-for-service beneficiaries from 2006- 2011 revealed inpatient rehabilitation facilities experience 30-day readmission rates ranging from 5.8% to 18.8% for many different target diagnoses [4]. This trend presents a challenge for post-acute care administrators seeking to contract with or form relationships with integrated delivery systems.
While multiple studies have illustrated the relationship between elevated patient satisfaction and decreased readmissions [5, 6], a lack of specific data and best practices for post-acute care environments necessitates a better understanding of the processes and experiences associated with transferring patients from acute medical centers to post-acute care settings including inpatient rehabilitation facilities (IRFs), long-term care hospitals (LTCs), and skilled nursing facilities (SNFs). A review of data from the Medicare Current Beneficiary Survey illustrated a varied array of care patterns and post-acute care transitions experienced by Medicare beneficiaries, many of which were considered complicated transitions requiring complex care and multiple providers [1]. These complicated post-hospital care patterns frequently involve several transitions and facilities that present challenges for patient communication, engagement in decision making, and complex care management throughout the process.
Several factors have been shown to contribute to decreased patient satisfaction during patient discharge and facility transfers. Communication breakdowns between providers, staff, patients, and family can cause anxiety and stress and contribute to negative health outcomes and frequent returns to the acute care environment [7]. Another study illustrated a relationship between a lack of patient involvement in important care decisions and not receiving appropriate discharge instructions with a substantially higher likelihood of readmission [8].
Patients who perceive that they have not been consulted in major care decisions have an increased likelihood of unplanned readmissions, while the odds of readmission did not differ based on understanding of discharge medications, understanding of post-care instructions, or discussion planning for home discharge. Several studies have illustrated how patients and their caretakers are frequently poorly prepared to manage patient needs in the home post- discharge [9, 10]. However, there is an opportunity for additional research regarding the quality of care and patient experience with transitions between facilities and the impact on patient outcomes in the post-acute care environment. While many patients leave acute care medical centers without an understanding of all of their medications, and often even their primary diagnosis, health systems can improve patient understanding, realize cost savings, and improve overall perceptions of quality of care by improving the coordination of discharge, patient transfer, and follow-up processes [11]. Lastly, studies have also illustrated that patients and families often feel unprepared or ill-prepared for discharge, and report that post-discharge care is not tailored to individual patient needs and preferences [12].
Methods
The primary aim of this study was to provide additional insight into patient experience before, during, and after transfers to post-acute care settings from a higher level of care, and to open a dialogue with multiple facilities around potential solutions and tools to guide healthcare providers and administrators in improving their discharge processes. A secondary aim of this study was to collect additional narrative qualitative information in the form of comments to be used in a secondary study evaluating provider responses to patient experience comments related to care transitions and to encourage the development of best practice recommendations for improving those processes.
In collaboration with 18 inpatient rehabilitation hospitals (IRFs), six long terms acute care hospitals (LTAC), and 14 skilled nursing facilities (SNFs), a cross-sectional study was conducted in which 1264 adult patients in post- acute care settings were surveyed regarding their patient experience with post-acute care transitions and coordination of care. Questionnaire items were adapted from multiple validated self-report instruments, pilot-tested and edited from in 2018 and early 2019, and combined into a single 28-item questionnaire administered confidentially with no personal health information included and only demographic data collected. Between days three and five of the patient’s stay in the post-acute care setting, the survey was presented as a voluntary optional survey allowing participants to share their perspectives and provide feedback on their experience being transferred from the acute care medical center.
Only patients who were transferred from general acute care settings were eligible to participate in the survey in order to avoid including patients who experienced transfers from one post-acute care environment to the next, such as transferring from rehabilitation to skilled nursing facilities. While these transitions are also important, this study’s aim was to capture experiences with acute to post-acute care transfers. The survey was administered in two formats, allowing the patient to voluntarily select to either complete a paper-based survey and place the document in a sealed envelope or complete the survey by taking a digital photo or scanning a QR code linked to a confidential online survey. The survey defined care transitions as “your experience leaving the hospital and being transferred to this next level care at the current facility you are receiving care”. Surveys were distributed by case management staff during business hours, and patients who transferred from an inpatient acute level of care in the last 3-5 days were eligible to participate in the study.
Research Questions
Multiple research questions were explored, including potential differences in self-reported levels of patient experience and perceptions of patient-centered care provided by staff working in both inpatient and post-acute care environments. The study explored levels of patient preparedness for transfer to another level of care as well as perceptions of transfer experience and general patient experience across destination facility types, including skilled nursing facilities, inpatient rehabilitation facilities, and long term acute care facilities. Differences in patient experience were evaluated for general measures and sub-items in order to answer the question, “Do differences in patient transfer experience exist across post-acute care settings (inpatient rehab, skilled nursing, and long term acute care)?”.
Exploratory factor analysis and multiple linear regression analysis were used to evaluate the grouping of five questionnaire items and the relationship between these separate measures of experience with two primary constructs: (1) overall patient experience and (2) patient experience with post-acute care transitions. To provide additional context, focus group sessions were conducted with physicians and staff, including nursing, pharmacy, therapy, and case management across different care settings. Physicians and staff were asked to share where they felt most and least confident in their respective approaches, procedures, and models of care, and where they believed elements of their care met the standard of being a true best practice.
Variables and Factors
Five facets of patient experiences with post-acute care transfers were included in the modeling of the dependent variable of transfer experience. These facets were included based on meaningful roles and experiences common in the literature used to evaluate inpatient facility discharge planning [10, 13]. Figure 1 illustrates the five elements assessed when evaluating patients’ experience with post- acute care transfers.
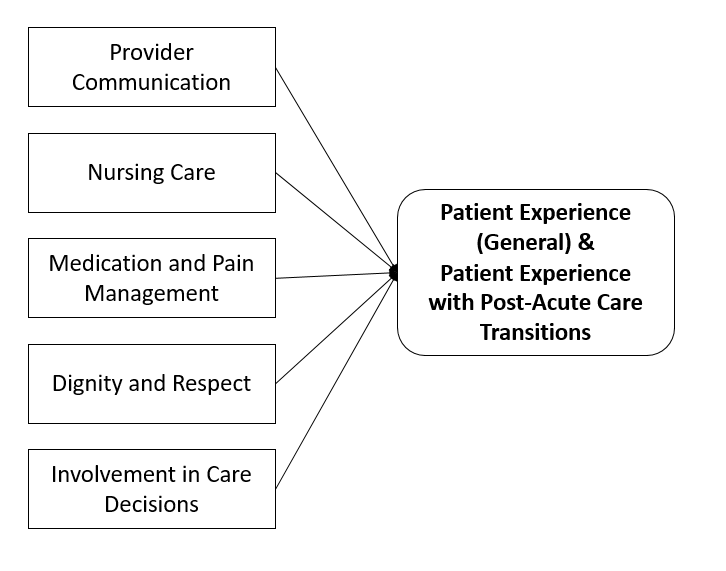
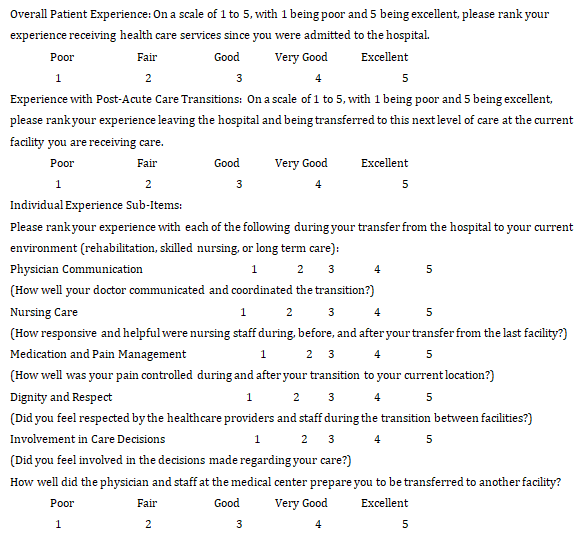
Study participants were asked to score (1) their overall experience and (2) their experience with their acute to post- acute care transfer (on a scale from 1 to 5, with 1 being poor and 5 being excellent) and to score the five specific areas of patient transfer experience illustrated in Figure 1 using the prompts and clarification questions included in Figure 2 below.
Analysis
A variety of analysis options were utilized to evaluate differences in patient experience and provide facility-level data to participating organizations. Several one-way analysis of variance (ANOVA) tests were conducted to compare differences in patient experience overall and across specific facets of discharge experience by patient destination setting LTAC, IRF, and SNF). To reduce the likelihood of a Type I error, a multivariate ANOVA (MANOVA) was used to evaluate differences in all patient experience elements across destination settings (LTAC, IRF, and SNF).
In addition to evaluating differences in patient transfer/ transition experience across post-acute settings, multiple regression analyses were conducted to evaluate the relationship between individual survey components, including nursing care experience and provider communication, and overall patient experience as well as patient experience with post-acute care transfers. Exploratory factor analysis was utilized to explore the use of the five sub-item questions as measurements for factors contributing to patient experience, both specific to care transitions and in general. The items included provider communication, nursing care, medication and pain management, dignity and respect, and involvement in care decisions, as shown in Figure 1.
Using the principles of grounded theory, a qualitative analysis was also conducted on a large sample of 5,349 comments collected from the combined 1264 surveys administered throughout 2018. These comments provided context for the quantitative analysis and served as the catalyst and driver for focus group discussions in the provider and staff perception study conducted in 2019.
Results
Patient Experience with Post-Acute Care Transfers
A one-way ANOVA revealed statistically significant differences in mean reported patient experience with post- acute care transfers across destination settings (F (2, 1261) = 6.11, p< .001), indicating that patients reported higher experience scores when admitted to IRF settings (m = 4.31, SD=1.5) than those transferred to other settings (m = 3.10, SD = 1.1). The multivariate ANOVA (MANOVA) conducted to evaluate differences in all patient experience elements across the three primary post-acute destination settings (LTAC, IRF, and SNF) revealed a significant difference in aggregate patient experience with post-acute care transfers across settings (F=4.83, p<.01).
The adjusted R squared of 0.536 (p<0.001) indicated that the individual experience categories, including items such as being treated with dignity and respect, nursing care experience, and provider communication, account for more than half of the explained variation in transfer patient experience leaving general acute care hospitals and moving to another level of care. Table 1 below includes results from the exploratory factor analysis illustrating the % of variance in general patient experience and post-acute care transition experience attributed to the items used in the patient experience with care transitions index.
| Item | Factor Loadings | |
|---|---|---|
| Patient Experience (General) | Patient Experience (Post-acute Care Transitions) | |
| Provider Communication | 0.391 | 0.61 |
| Nursing Care | 0.322 | 0.438 |
| Medication and Pain Management | 0.481 | 0.619 |
| Treated with Dignity and Respect | 0.326 | 0.516 |
| Patient Involvement in Care Decisions | 0.641 | 0.731 |
| Eigenvalue | 1.284 | 2.941 |
| % of Variance Explained | 41% | 54% |
Table 1: Summary of Exploratory Factor Analysis Results for Patient Experience Questionnaire Measure Using Maximum Likelihood Est
Patient Perceptions of Preparation for Transfer
On a scale of 1 to 5, with 1 being poor and 5 being excellent, patients across all settings provided a mean score of 3.18 in response to “How well did the physician and staff at the medical center prepare you to be transferred to another facility?”. An additional one-way ANOVA test revealed mean scores indicating that patients felt most prepared for transfer to inpatient rehabilitation facilities (IRFs) (m=3.81, SD=.6) and the least prepared for transfers to skilled nursing facilities (SNFs) (m=2.93, SD=.9) (p<.05).
Limitations
This study included several limitations due to the nature of self-reported data and the potential for self-report or social-desirability bias depending on the degree of privacy and comfort the patient perceived during the process of completing the survey. Additionally, the surveys administered in the long term acute care (LTAC) hospital environment may have been disproportionately completed by family members instead of patients due to the higher level of acuity of these patients, thus leading to potentially different responses. The decision to refrain from collecting identifying information from patient participants also limited the additional analysis options available. Had the researchers chose to collect identifiable information, potentially the individual sites could have used this information to perform further analysis evaluating satisfaction data in correspondence with other patient outcomes.
Another notable limitation was the ambiguity in the survey question language referring to “your experience being transferred from the hospital to this facility” as well as similar language used in the five sub-item questions. Participants could potentially become confused and refer back to a different type or occurrence of “transfer” and in fact not be reflecting back on their most recent move to their current post-acute care environment. The research team endeavored to develop and pilot test language that acutely described the various elements of patient transfers while still using plain language within an acceptable reading level in both English and Spanish.
Discussion
The assessment of patient experience with care transitions revealed higher patient experience scores in almost all questionnaire items for inpatient rehabilitation patients. Specifically, patients in inpatient rehabilitation facilities reported higher patient transition experience scores (m=4.31) than those transferred to skilled nursing facilities (m=3.27) or long-term acute care hospitals (m=2.72). Additionally, patients transferred to the IRF setting reported higher mean aggregate scores for the five sub- items compared to other settings (F=4.83, p<.01). (F=4.83, p<.01). Furthermore, this study also revealed that patients self-reported feeling most prepared for transfer to inpatient rehabilitation facilities (IRFs) (m=3.81, SD=.6) and least prepared for skilled nursing facilities (SNFs) (m=2.93, SD=.9) (p<.05). However, future research should consider whether this difference in patient confidence in and experience with their preparation for transfer could be impacted by levels of cognitive function or other differences between patients eligible for rehabilitation services and those sent directly from general acute care settings to skilled nursing facilities.
Exploratory factor analysis (CFA) was successfully utilized to further evaluate the use of the 5-item model previously piloted to understand and explain variation in experience with care transitions as well as opportunities to impact that experience by addressing individual elements and roles. The CFA illustrated patient involvement in care decisions as the single greatest contributor to both overall patient experience and patient experience with post-acute care transitions. Patient involvement in care decisions has also been shown to be a factor in patient experience and reduced readmission rates [14].
Conclusion
While there have been several studies evaluating discharge processes incorporating patient-centered care elements, this study illustrated the importance and need for similarly coordinated processes to facilitate transfers as a type of discharge. While patients and caretakers may not generally require the same level of education and instruction required for discharges to home/community settings, this study illustrated the great extent to which communication and involvement of patients and families during transfer processes is a driver of transfer patient experience and overall patient experience. This study also demonstrated the need for deliberate planning, cooperation, and joint accountability between facilities to improve transfer processes between care settings and develop improved documentation similar to discharge to home processes for general acute care medical centers.
Implications
This effort to capture patient experience feedback specific to post-acute care transfers has several implications for quality improvement professionals working across settings. These results prompt healthcare quality professionals to consider opportunities for improved inter- organization collaboration. Additional areas for future research include further evaluation of discharge processes of both acute medical centers and post-acute care settings, as well as the development and validation of best practices for incorporating specific clinical and financial outcomes using matched data linking specific patient care practices to those outcomes. Directly linking clinical outcomes such as readmissions and hospital acquired conditions (HACs) with specific patient experience information and associated providers could yield more actionable data allowing administrators to make targeted improvements in care transitions. Accomplishing this type of action research and performance improvement would require data transparency and cooperation between acute inpatient medical centers and post-acute care settings as part of a broader coordinated care approach. Developing an improved understanding of how patient experience with care transitions correlates with patient outcomes could better inform efforts to improve care coordination across settings.
Ethical and Research Considerations
This study was approved by the Institutional Review Board as a full-board review category research study (IRB #067-2021). All participants provided written informed consent. This project was not funded by any agency or organization, and there are no financial relationships to disclose.
References
-
Coleman EA, Min SJ, Chomiak A, Kramer AM (2004) Posthospital care transitions: patterns, complications, and risk identification. Health services research 39(5): 1449-1465.
-
Greenwald JL, Jack BW (2009) Preventing the preventable: reducing rehospitalizations through coordinated, patient-centered discharge processes. Professional case management 14(3): 135-142.
-
Burke RE, Juarez Colunga E, Levy C, Prochazka AV, Coleman EA, et al. (2015) Rise of post-acute care facilities as a discharge destination of US hospitalizations. JAMA internal medicine 175(2): 295-296.
-
Ottenbacher KJ, Karmarkar A, Graham JE, Kuo YF, Deutsch A, et al. (2014) Thirty-day hospital readmission following discharge from postacute rehabilitation in fee- for-service Medicare patients. JAMA 311(6): 604-614.
-
Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R (2011) Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. American Journal of Managed Care 17(1): 41-48.
-
Hachem F, Canar J, FullamF, Gallan AS, Hohmann S (2014) The relationships between HCAHPS communication and discharge satisfaction items and hospital readmissions. Patient Experience Journal 1(2): 1-9.
-
Baker P, Tytler B, Artley A, Hamid K, Paul R, et al. (2017) The use of a validated pre-discharge questionnaire to improve the quality of patient experience of orthopaedic care. BMJ Quality Improvement Reports 6: u212876. w5262.
-
Kyle AK, Hude Q, Maria J (2017) Lack of patient involvement in care decisions and not receiving written discharge instructions are associated with unplanned readmissions up to one year. Patient Experience Journal 4(2): 1-12.
-
Coleman EA, Smith JD, Frank JC, Eilertsen TB. Thiare JN, et al. (2002) Development and testing of a measure designed to assess the quality of care transitions. Int J Integr Care 2: e02.
-
Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, et al. (2007) Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA 297(8): 831-841.
-
Clancy CM (2009) Reengineering hospital discharge: a protocol to improve patient safety, reduce costs, and boost patient satisfaction. American journal of medical quality: the official journal of the American College of Medical Quality 24(4): 344-346.
-
Hesselink G, Flink M, Olsson M, Barach P, Dudzik Urbaniak E, et al. (2012) Are patients discharged with care? A qualitative study of perceptions and experiences of patients, family members and care providers. BMJ quality & safety 21(1): i39-i49.
-
Horstman MJ, Mills WL, Herman LI (2016) Patient experience with discharge instructions in postdischarge recovery: a qualitative study. BMJ Open 7: e014842.
-
Hesselink G, Zegers M, Vernooij Dassen M (2014) Improving patient discharge and reducing hospital readmissions by using Intervention Mapping. BMC Health Serv Res 14: 389.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda