Covid 19 Pandemic & Women’s Health Pregnancy, Parturition & Postpartum Problems & Vaccination Challenges
Th global dilemma of Covid 19 pandemic, is just 30-40% of COVID-19 cases have been disaggregated by both sex and age. Many anecdotal studies in different countries indicate a higher incidence, mortality, and fatality rates among men than among women. These rates vary widely by region, country, and men are at greater risk of COVID-19 death. The proportion of male and female Covid 19 patients was 51: 49 as against the proportion of Covid 19 deaths was 55:45. The mortality and fatality rates increased with age and were most predominant in men 50 years of age or older. Studies from around the world show that pregnant women are no more likely to get COVID-19 than other healthy adults. Only 1/3 of infected pregnant women had mild cold or flu-like symptoms. CDC data showed a highest number of COVID-19-related deaths in pregnant people in August 2021. It indicated that 97% of pregnant people hospitalized, either for illness or labour and delivery, with confirmed SARS-CoV-2 infection were unvaccinated. While worldwide Covid 19 vaccination emergency use was granted in December 2020, for the pregnant women it was withheld until from December 14, 2020, to February 28, 2021, about 36,000 pregnant women were tested for safety issue and emergency use was cleared in April 2021 by USFDA. Most Covid 19 infected pregnant women will be asymptomatic or have a mild disease and recover without any need for hospitalization. In less than 5% cases rapid deterioration in health occurs that sometimes affects the foetus too. In case of severe disease, like all other patients, pregnant women needed hospitalization, ICU care and ventilator support. The possibility of pre-mature delivery, low birth weight (< 2.5 kg) and in rare situations, still birth increases. Pregnant women Older than 35 years of age, Obese, having an underlying medical condition such as diabetes or high blood pressure and have a history of clotting in the limbs are at higher risk. Given the fact India is home for 27 million pregnancies each year, I estimate that at least 2.7 million women faced the consequences of Covid 19. The GOI and State Governments have accepted lack of exact data about Covid 19 among pregnant women and its consequences in the last 2 years. All component of maternal care did suffer throughout the country. Data suggested that women who were pregnant or recently pregnant are at an increased risk for severe illness from COVID-19 when compared to people who are not pregnant. Indian Government approved vaccinating pregnant women on 2 July 2021. A recent response in Rajya Sabha indicates that as of 2 February 2022 28.22 lakh dose were reported to have been given to pregnant women and 11.68 Lakhs of them had got both doses. With the birth of 25 + million children India accounts for nearly about 27 million pregnancies each year. As of 2/7/21, the day GOI cleared vaccination for pregnant women the country had an estimated 16 million (60% of annual pregnancies that could have been recognized as pregnant) pregnant women and added 2 .2 million pregnancies every month, taking the total of eligible to 25 million in the last 7 months of which we protected only 1.17 million a meagre 5%. Among those vaccinated by 31 January 2022, 64 had some adverse reactions of which 38 were severe in nature. Materials & Methods: Review of publications from different countries and press reports in major City editions of popular daily newspapers like Times of India, Hindu, Hindustan Times, India Express, Economic times etc. Periodical press releases and statements in Parliament and State Assemblies. Anecdotal studies form the scientific basis for this article.
Introduction
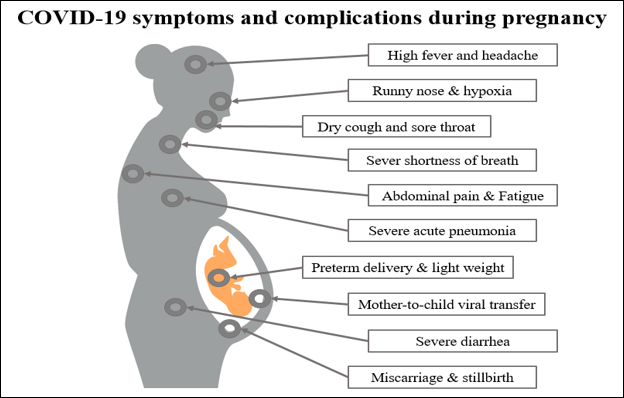
The clinical manifestation of COVID-19 among pregnant women has been characterized by mild and sometimes severe upper respiratory tract symptoms, such as dry cough and chest tightness, as well as other, less commonly observed symptoms such as high fever, fatigue, dyspnoea, diarrhoea, and headache. Typically, severe upper respiratory tract infections are confirmed using chest computed tomography (CT images). China’s case-control study revealed that 94% of pregnant women with confirmed COVID‐19 infections had severe infections. However, another study reported that most pregnant women with COVID-19 were asymptomatic upon admission to hospital, and none experienced any severe respiratory failure during their hospital stay. This suggests that different stages of pregnancy and different immune responses in each case may affect the presenting symptoms of COVID-19 in pregnant women. A study by Yang et al. found that COVID-19 positive cases did not show any expectoration, dyspnoea, or myalgia. However, CT images of their pulmonary systems resembled COVID‐19 pneumonia. Furthermore, pleural effusion was significantly higher among COVID-19 positive cases in pregnant women compared to non‐pregnant women. Figure below presents a summary of the symptoms and potential complications that can occur in COVID-19-infected pregnant women (Figure 1).
Adverse Outcomes of COVID‐19 among Pregnant Women
COVID-19 infection has been associated with maternal hypercoagulability and pyrexia (cytokine storm), which can lead to increased infarction, placental intervillous thrombosis, and maternal hypoxia38, 39. However, evidence regarding foetal morbidity and mortality due to COVID-19 infection is still limited. Still, maternal changes secondary to COVID-19-infected pregnant women may lead to hypoxia and foetal heart rate changes38. In two recent studies by Zhu et al. and Chen, et al. found that in eighteen middle-aged pregnant women infected with COVID-19, all had at least one or more common clinical symptoms, such as a dry cough, fever, sore throat, chest pain, or diarrhoea. A significant variation in new-born birth weight was observed in these mothers, with weights ranging from 1520 g to 3820 g. The authors reported that more than half of the pregnant women in the studies had preterm deliveries, which is a higher rate than seen in non-infected pregnant women. They also reported other obstetrical complications in these women, such as preeclampsia, irregular contractions, premature rupture of membrane, and stillbirth, indicating early pregnancy intervention. Anatomical changes during pregnancy, such as diaphragm elevation, increased thoracic cage transverse diameter, decreased maternal tolerance to hypoxia, put pregnant women at a higher risk from respiratory infections. Baud et al. observed contractive abdominal pain and fever among pregnant women suffering from COVID-19. A study from Iran reported that, out of nine COVID‐19 infected pregnant women who were displaying initial symptoms of pneumonia, seven women died following a few days of hospitalization. Of the two who survived, one of them was critically sick and ventilator-dependent, while the other was successfully cured after prolonged hospitalization 44. Table 1 summarizes the maternal outcomes of COVID-19-infected pregnant women and their neonates observed in various studies.
Foetal Outcomes in COVID‐19 Infections
The first reported new-born infant delivered by a COVID-19 positive mother was on February 5th, 2020. This was announced by the official Xinhua news agency. The infant had no fever or cough and stable vital signs but had observable shortness of breath, unusual chest radiographs, and abnormalities in liver function. Dashraath, et al. observed numerous adverse neonatal outcomes from COVID-19 positive mothers, including foetal distress (43%), preterm birth (39%), intrauterine growth restriction (10%), perinatal death (7%), and miscarriage (2%). These outcomes were mainly dependent on the stage and complications during the pregnancy. Increased effects of COVID-19 on pregnant women led to more adverse foetal outcomes. It remains unclear if Foetal distress reported in pregnant women; is caused by the COVID-19 infection or pneumonia. In their systematic review, Yang et al. reported that other COVID-19-related adverse foetal and neonatal outcomes like foetal distress, stillbirth, neonatal death, and neonatal asphyxia. In a different study, the prognosis of infected infants was reported to be good, although preterm births with significantly low birth weights were observed, and many new-borns suffered intrauterine foetal distress and respiratory distress syndromes. Some new-borns were immediately admitted to neonatal intensive care units as they had neonatal pneumonia, which requires neonatal mechanical ventilation. The placenta has been reported to execute and orchestrate the pathways of foetal growth. Some studies have revealed the ability of COVID-19 to induce placental gross pathological alterations. Vascular abnormalities that occur in the placentas of infected mothers included foetal vascular malformations and malperfusion in 50% of pregnancies. Chen et al. reported an increased incidence of spontaneous and induced abortions among infected mothers, suggesting the potential risks of abortion, premature gestational loss, and congenital defects in neonates in infected mothers [1].
Impact of Covid 19-Globla Status
Many anecdotal studies in different countries indicate a higher incidence, mortality, and fatality rates among men than among women. These rates vary widely by region, country, and men are at greater risk of COVID-19 death. The proportion of male and female cases was 51:49% as compared the proportion of deaths among Covid 19 patients was 55:45. The mortality and fatality rates increased with age and were most predominant in men 50 years of age or older.
Prior to the Covid 19 pandemic, it was estimated that one in three women will experience violence during their lifetimes. Economic and social stresses combined with movement restrictions and cramped homes are driving a surge in gender-based violence in the last 2 years worldwide. With more people spending time online, online forms of violence against women and girls in chat rooms, gaming platforms are reported have increased. Globally, women make up 70 per cent of the health workforce, especially as nurses, midwives and community health workers, and account for most service staff in health facilities as cleaners, launderers, and caterers. These people faced increased risk of violence as they navigate urban slums or remote rural public spaces as transportation services are disrupted under lockdown. The pandemic’s economic impacts are likely to increase sexual exploitation and child marriage.
Th worst impact of Covid 19 pandemic globally, is just 30-40% of COVID-19 cases have been disaggregated by both sex and age. Before the pandemic started, women did nearly three times as much unpaid care and domestic work as men. Due to social distancing measures, school closures and overburdened health systems have put an increased demand on women and girls to cater to the basic survival needs of the family and care for the sick and the elderly and existing gender norms have put the increased demand for unpaid childcare and domestic work on women. India and many developing countries have seen young women and girls living in poverty, with disabilities or in rural, isolated locations were pulled out of school first to compensate for increased care and domestic work at home. For many women migrant domestic workers, the pandemic has led to loss of income and jobs with their health, safety and well- being often ignored.
In several countries, domestic violence reports and emergency calls have surged upwards of 25% from around 40% who experienced violence and sought help prior to pandemic since social distancing measures were enacted as they serve to isolate many women trapped with their abusers from friends, families, and other support networks.
Hand hygiene and sanitation is a critical element in preventing the spread of COVID-19. UNICEF estimates that 3 billion people (40 %of the world’s population), do not have a handwashing facility with water and soap at home, and the world’s extreme poor around 689.4 million, over half of whom are women and girls were at immediate high-risk Covid 19 transmissions due this single factor. A recent study found that the routine health care is disruption and denial access to food and health care decreased, and increased child and maternal deaths in about 118 low- and middle-income countries 10-45% in under-5 deaths per month and an 8-39% rise in maternal deaths per month [2].
Impact of Covid 19 in India
COVID-19 can infect people of all gender and ages in India. However, some women and girls were at higher risk as either they are poorer and lack information and resources, or because they are at the front line as caregivers and workers in the health and service sectors.
A retrospective study of about 130,00 cases in May 2021 had inferred that the chances of being COVID-19 infected was higher for females of lower age categories (<35 years) which decreased with age. The chances of recovery declines with increasing age. The male COVID-19 cases were 65.39% as compared to 34.61% among females and mean age of infected and recovered patients was higher in men (39.47 ± 17.59 years) compared to women (36.85 ± 18.51). The age- adjusted odds for recovery among females was (O.R. = 1.779) higher than men were highest in 5-17 years age category (O.R. = 88.286) independent of gender [3].
In India, women make up a very high proportion of all frontline healthcare workers as more than 80% of nurses, ANMs, ASHA’s AWWs are women. Since women in India spend more hours caring for children, the elderly and sick family members, and masks and other personal protective equipment are often designed and sized for men, women may be at risk of more exposure to the virus. Initially there was a concern that less women are getting vaccinated than men and only in July 2021 vaccination was opened for 27 million pregnant women annually and nearly 40 million of pregnant women between January 2020 and July 21 missed the Covid vaccination in India. Lesser access to internet or smart phones also hindered registration for vaccination. Some rural and urban slum women found it difficult to go to the vaccination centres alone, and preference was given for male family members to get vaccinated first [3].
COVID-19 Impact on Women’s Employment in India
Wage inequality and the burden of unpaid care have pushed more women out of employment and into poverty. Women’s earned income in India was just one-fifth that of men’s even before the pandemic. Globally, and in India, more women have lost jobs during COVID-19. A recent report by the Center for Sustainable Employment at Azim Premji University in India shows that during the first lockdown in 2020, only 7% men lost their jobs, compared to 47 per cent of women who lost their jobs and did not return to work by the end of the year and in informal jobs women accounted for 80% job losses. Indian women spend more time doing unpaid care work at home than men. On an average, 10 times more than men on unpaid domestic chores and 4.5 hours a day caring for children, elders and the sick. During the pandemic, their share of unpaid care work grew by 30-40% [4].
My Observations of Pregnancies and Counselling for Covid 19 Infection or Vaccination Since 2020
I have counselled and observed at least 15 young pregnant mothers in known circle since early 2020. All of them were in the age range of 25-35 years. 10 were second para and remaining primigravida’s. Three of them are in Bay area, San Francisco, one in Berlin, Germany and five in Bengaluru, 1 in Pune and another 5 in northern districts of Karnataka Vijayanagar (2), Haveri, Kalburgi, Raichur one each. Five of them went through the pregnancy and post- partum period before vaccination has stared in July 2021 and had no problem except one of them had a premature delivery at 38 weeks, but both baby and mother gained normal growth pattern by 3rd month. The mother of this baby had long postpartum depression. Worrying about the baby for almost 3 months. While 2 of the USA and Berlin girl had normal vaginal deliveries, all but one Indian delivery, the obstetricians had advised and intervened with caesarean sections. I could observe a clear difference in the mental makeup of those who delivered without vaccination, worrying about the chances of getting Covid 19 during hospital stay and getting discharged within 2 days. One of the unvaccinated mothers in India in October 2021 was RTPCR positive, during a mandatory test when hospitalized for delivery. The post-partum period had no consequences and new-born was breastfed. Ten of them who had the advantage of getting vaccinated during pregnancy were well prepared and least worried. Though all of them had minor vaccine associated After effects of Immunization (AEFI) of local pain and fever for 2-3 days, one had prolonged local pain and fatigue for a week, and another had sore throat, for about a week and cough, loss of appetite for about 10 days. RTPCR tests of both these patients were negative. Overall, no serious consequences were observed.
Discussions
Investigating the Impact of COVID-19 during Pregnancy, CDC Atlanta, USA
CDC, Atlanta, USA, through multiple efforts to increase the global understanding of the impact of COVID-19 on pregnant women and infants since mid-2020. Data collected as part of these suggest that women who were pregnant or recently pregnant are at an increased risk for severe illness from COVID-19 when compared to people who are not pregnant. Women who have COVID-19 during pregnancy are also at increased risk for preterm birth (delivering the baby earlier than 37 weeks) and stillbirth and might be at increased risk for other pregnancy complications [5].
Other Observations in USA
Baylor Medical College Houston recently reported that even the healthiest pregnancies can have problems with little or no warning during labour and delivery. They opined that a hospital setting can give mother and the baby the best care if needed as the hospitals, hospital-based birth centres, and accredited freestanding birth centres follow strict procedures to clean and control infection. However, they advised persons in the hospital or birth centre, must wear a mask if patient had COVID-19 test positive. But during labour, wearing a mask may be difficult and therefore, health care team should wear masks or other protective breathing equipment and take other steps to reduce the risk of spreading the virus, including wearing goggles or face shields.
According to them it is not likely that COVID-19 can pass through breast milk and cause infection in the baby and therefore it is safe to feed breast milk to baby even if the mother has COVID-19. Emphasizing the fact that breast milk is the best source of nutrition for most babies and helps protect babies from infections, of the ears, lungs, and digestive system, they strongly advocated COVID-19 positive mothers not to stop giving their baby breast milk.
Commenting on the debate of Home Vs Hospital Delivery, they advised that the safest place giving birth is a hospital, hospital-based birth centre, or accredited freestanding birth centre and COVID-19 has not changed this recommendation. Their recommendations to Pregnant and recently pregnant women included steps to stay healthy, including, getting a COVID-19 vaccine, wearing a mask and take other steps to prevent infection as per local guidelines. They advised pregnant women to keep prenatal and postpartum care visits, and not to change timing and method of delivery. They preferred women who are sick to avoid a caesarean birth. Facilities were advised to limit the number of visitors based on local and state recommendations to help prevent the spread of COVID-19 [6].
United Kingdom Observations
The UK Obstetric Surveillance Study (UKOSS) report from January 2021 describes 1,148 pregnant women with COVID-19 who were admitted to hospital between March and September 2020. Nearly one in five women with symptomatic COVID-19 gave birth prematurely. However, women who tested positive for COVID-19 but had no symptoms were not more likely to give birth prematurely. The babies of women with COVID-19 were more likely to be admitted to the neonatal intensive care unit (NICU), but almost all these babies did well. There was no statistically significant increase in stillbirth rate or infant death for babies born to women who had COVID-19. Not all the babies were tested, but overall, only 1 baby in 50 tested positive for COVID-19, suggesting that transmission of the infection to the baby is low.
Another study from the UK compared 3,500 women who had COVID-19 at the time they gave birth to over 340,000 women who did not have COVID-19 at the time they gave birth. This study found that pregnant women who tested positive for COVID-19 at the time of birth were twice as likely to have a preterm birth, and their risk of stillbirth was twice as high, although the actual number of stillbirths remains low [7].
Covid 19 among African Women
In many African countries, women have borne the brunt of the harmful effects of the pandemic. They have had limited to no access to essential maternal and child health services for a significant time because of COVID-19 restrictions and scarce resources in already overstretched hospitals and health centres. While more data is needed to fully document the extent of the COVID-19 pandemic’s impact on women and children across Africa, some preliminary numbers have shown a drop in utilization of essential reproductive, maternal, and neonatal health services (Figure 2).
The number of women who attended the recommended medical visits during pregnancy dropped by 18 percent in Liberia, and the initiation of women seeking medical care during pregnancy fell by 16 percent in Nigeria, according to findings by the Global Financing Facility. Additionally, a recent modelling study across 118 of the world’s countries estimated that between 8.3 percent and 38.6 percent more pregnant women could die each month. In countries like the Democratic Republic of Congo and Nigeria, this would add an additional 1,280 and 6,700 maternal deaths to the already staggering 16,000 and 67,000 respective maternal deaths each year [8].
Rest of the World Observations
Studies from around the world show that pregnant women are no more likely to get COVID-19 than other healthy adults. Only 1/3 of pregnant women had mild cold or flu-like symptoms. But unvaccinated or not fully vaccinated pregnant women were at an increased risk of becoming severely unwell if they catch COVID-19, which can lead to them needing intensive care and their baby being born prematurely.
Current evidence suggests that the virus, is unlikely to cause problems with baby’s development, and there have been no reports of this so far. There is also no evidence to suggest that COVID-19 infection in early pregnancy increases the chance of a miscarriage. Transmission of COVID-19 from a woman to her baby during pregnancy or vertical transmission seems to be uncommon. Mode of birth i.e., vaginal birth or caesarean, feeding choice or whether the woman and baby stay together or not does not influence the transmission. In most of the reported cases of new-born babies developing COVID-19 very soon after birth, the babies remained well.
Studies have shown that there is a two- to three-times increased risk of giving birth prematurely for pregnant women who become very unwell with COVID-19, as it was recommended that their babies were born early for the benefit of the women’s health and to enable them to recover. Babies born before full term (before 37 weeks) are vulnerable to problems associated with being born premature – the earlier in the pregnancy a baby is born, the more vulnerable they are.
For 8 months from March 2, 2020, a study enrolled women 18 years or older at any stage of pregnancy or delivery with the diagnosis of COVID-19 during the present pregnancy based on laboratory confirmation of COVID-19 and/or radiologic pulmonary findings suggestive of COVID-19, 1 or 2 or more predefined COVID-19 symptoms. A range of different real-time polymerase chain reaction and antibody tests were used at participating institutions (eBox in the Supplement). Two immediately concomitant pregnant women 18 years or older without any of those diagnostic criteria were enrolled per woman with COVID-19 diagnosis to create an unbiased sample of all pregnant women without COVID-19 diagnosis in these institutions. Women were enrolled from 43 institutions in 18 countries (Argentina, Brazil, Egypt, France, Ghana, India, Indonesia, Italy, Japan, Mexico, Nigeria, North Macedonia, Pakistan, Russia, Spain, Switzerland, UK, and the US). Data on race were not collected.
A total of 706 pregnant women with COVID-19 diagnosis and 1424 pregnant women without COVID-19 diagnosis were enrolled, all with broadly similar demographic characteristics (mean [SD] age, 30.2 [6.1] years). Overweight early in pregnancy occurred in 323 women (48.6%) with COVID-19 diagnosis and 554 women (40.2%) without. Women with COVID-19 diagnosis were at higher risk for preeclampsia/eclampsia (relative risk [RR], 1.76; 95% CI, 1.27-2.43), severe infections (RR, 3.38; 95% CI, 1.63-7.01), intensive care unit admission (RR, 5.04; 95% CI, 3.13-8.10), maternal mortality (RR, 22.3; 95% CI, 2.88-172), preterm birth (RR, 1.59; 95% CI, 1.30-1.94), medically indicated preterm birth (RR, 1.97; 95% CI, 1.56-2.51), severe neonatal morbidity index (RR, 2.66; 95% CI, 1.69-4.18), and severe perinatal morbidity and mortality index (RR, 2.14; 95% CI, 1.66-2.75). Fever and shortness of breath for any duration was associated with increased risk of severe maternal complications (RR, 2.56; 95% CI, 1.92-3.40) and neonatal complications (RR, 4.97; 95% CI, 2.11-11.69). Asymptomatic women with COVID-19 diagnosis remained at higher risk only for maternal morbidity (RR, 1.24; 95% CI, 1.00-1.54) and preeclampsia (RR, 1.63; 95% CI, 1.01-2.63). Among women who tested positive (98.1% by real-time polymerase chain reaction), 54 (13%) of their neonates tested positive. Caesarean delivery (RR, 2.15; 95% CI, 1.18-3.91) but not breastfeeding (RR, 1.10; 95% CI, 0.66-1.85) was associated with increased risk for neonatal test positivity [9].
Pregnant Women and COVID-19 Infections in India
Ministry of Health and Family Welfare Govt. of India in its publication named ‘Counselling Pregnant Women for COVID-19 Vaccination’ summarize that Pregnancy does not increase the risk of COVID-19 infection. Most (>90 per cent) infected pregnant women will be asymptomatic or have a mild disease and recover without any need for hospitalization. In less than 5% cases rapid deterioration in health may occur that sometimes affects the foetus too. Symptomatic pregnant women appear to be at an increased risk of severe disease and death. In case of severe disease, like all other patients, pregnant women may also need hospitalization. In about 5% cases, COVID-19 infection in pregnancy may increase the possibility of pre-mature delivery, low birth weight (< 2.5 kg) and in rare situations, baby might end up in still birth. Pregnant women Older than 35 years of age, Obese, having an underlying medical condition such as diabetes or high blood pressure and have a history of clotting in the limbs are at higher risk. It is important that they take all precautions of using masks, frequent hand washing, avoiding going in crowd to protect them from acquiring COVID-19, and taking vaccination against COVID-19.
Covid has triggered an exponential rise in mental health issues among pregnant population. One in seven Indians were affected by mental disorders of varying severity in 2017, according to a study published in Lancet, while the National Mental Health Survey of India in 2016 found that one in 20 people in India suffers from depression. There is growing scientific evidence that mental health deteriorates with the coronavirus infection. During the pandemic, patients have been reporting anxiety and depression, as well as ‘Long Covid’, where recovered patients experience brain fog and are not able to think clearly. Patients are also showing neurological symptoms [10].
Data pertains to maternal and child health services being provided from public health facilities of District Sant Kabir Nagar in Uttar Pradesh, India, was analysed and compared for 2020 data from the pandemic phase with data from the year 2019 was done to determine the impact on services. Reduced coverage across all maternal and child health interventions was observed in the study. There was an overall decrease of 2.26 % in number of institutional deliveries. Antenatal care services were the worst affected with 22.91% decline. Immunization services were dramatically decreased by more than 20%. The response of the public healthcare delivery system to the Covid-19 Pandemic is negatively affecting both the provision and utilization of maternal and child healthcare services [11].
A researcher’s retrospective cross-sectional comparative study among the women and new-borns who received delivery or home-based new-born care (HBNC) in different ways across 36 territories in India, comparing the two years of the pandemic (2020 and 2021) with the two years before it emerged (2018 and 2019). Data were extracted from the Indian (HMIS) health management information system between January 2018 and May 2021. Variables like number of home deliveries by a Skill Birth Attendant (SBA), including doctors, nurses and midwives, the number of home deliveries that were attended by non-SBAs, including trained birth attendants (TBAs) and relatives, the number of pregnant women given Misoprostol during home delivery, the number of new-borns who received at least seven homecare visits, and data on institutional deliveries such as number of deliveries in total, number of women discharged within 48 hours, and number of new-borns receiving home visits following delivery at a healthcare institution were analysed, that showed that the average number of home deliveries attended by SBA across 2021, 2020, 2019, and 2018 were 15,491, 16429.25, 19006.58, and 21317.83, respectively – a decrease of ~27% between 2018 and 2021.
For the numbers of home deliveries attended by non-SBA a similar downward trend is observed, decreasing from 99830 in 2018 to 84592, 73351, and 66145 in years 2019, 2020, and 2021 respectively, a total decrease of 33.74% over the three years. The results for the number of pregnant women going for ANC saw a decrease across the four years from 2018 to 2021 by 9.72% (6718 to 6065). The mean number of new-borns receiving seven HBNC visits decreased by only 6.47% across the four years (78221 to 73158). Institutional deliveries decreased by 8.34% over the four years (566933 to 497037), the number of those new-borns that received 6 HBNC visits increased by 40.03%. The number of women discharged within 48 hours of delivery decreased by 12.32% [12].
Pregnancy Outcomes and Maternal Complications During the Second Wave of Coronavirus Disease 2019 (COVID-19) in Mumbai India
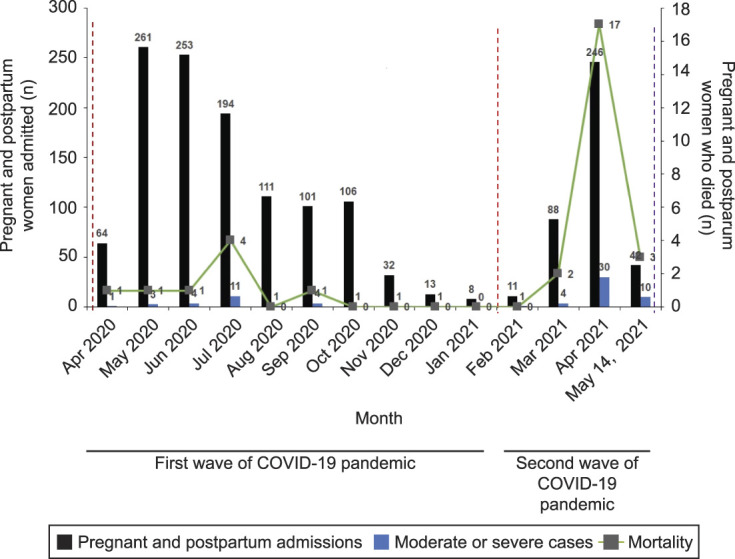
A retrospective observational cohort study of pregnant and postpartum women with COVID-19 admitted at BYL Nair Charitable Hospital, a dedicated COVID-19 tertiary care hospital in the Mumbai Metropolitan Region. COVID-19 was diagnosed as per the national testing guidelines. Pregnant women with confirmed COVID-19 who were near-term and those who needed obstetric interventions, those with high- risk pregnancies, and pregnant and postpartum women (up to 6 weeks) with moderate or severe disease were admitted after screening at a special screening outpatient department during both waves of COVID-19. Pregnancy outcomes and COVID-19 severity were compared between women admitted during the first and second waves of the COVID-19 pandemic in India. The severity of COVID-19 was categorized as per the Clinical Management Protocol for COVID-19 (in adults). Univariable comparisons were made using χ2. P<.05 was considered statistically significant. Statistical analysis was performed using SPSS Statistics Base 26.0.
A total of 1,530 pregnant and postpartum women were admitted as per the admission policy during the first (n=1,143) and second waves (n=387) of the COVID-19 pandemic. The rates of severe COVID-19, admission to the intensive care unit or high dependency unit, case fatality rate, and maternal mortality ratio were higher during the second wave. The preterm birth rate and stillbirth rate were not statistically different [13].
| parameter | 1st Wave | 2nd Wave | |
|---|---|---|---|
| (April 1, 2020-january 31, 2021) | (February 1-May 14, 202)* | P | |
| Total no. of pregnant and postpartum women treated | 1,143 | 387 | |
| Case fatality rate | 8(0.7) | 22(5.7a) | <.001 |
| Total no. of deliveries | 771 | 256 | |
| Total births | 783 | 264 | |
| Vaginal birth | 466(60.4) | 161 (62.9) | 0.48 |
| Cesarean births | 305(39.6) | 95(37.1) | |
| Gasrational age are delivery (wk) | 39(38-39) | 39(38-39) | |
| Preterm birth rate (per 1000 births) | 93.2 | 128.7 | 0.09 |
| Stillbirth rate( peer 1000 births) | 15.3 | 34.1 | 0.06 |
| Comorbid conditions and pregnancy complications | |||
| Cardiovascular disease | 5 (0.6) | 5 (1.9) | 0.6 |
| Anemia (Hb<11 g/dl) | 319.(41.4) | 134(52.3) | 0.002 |
| GDM | 15(1.9) | 6(2.3) | 0.69 |
| Gasrational hypertension | 39(5.1) | 56(10.20 | 0.03 |
| Preeclampsia | 46(6.0) | 9(3.5) | 0.13 |
| Eclampsia | 5(0.6) | 0(0.4) | 0.63 |
| Oligohydramnios | 39(5.1) | 4(1.6) | 0.01 |
| Covid-19 severity and outcomes | |||
| ICU or HDU admission | 27(2.4) | 45(11.6) | <.001 |
| severe covid-19 cases | 19(107) | 33(8.5) | <.001 |
| maternal mortality ratio (per 1000 births | 10.2 | 83.3 | <.001 |
Table 1: ** Pregnancy complication.
Covid-19, coronavirus disease; Hb, Hemoglobin; ICV, intensive care unit; HDU, high dependency unit. Dates are n, n (%), or median (interquartile range) unless otherwise specified. Chi-square test was applies at a significance level of P<0.05.
- The second waver of a pandemic is ongoing, and data were analyzed through May 14, 2021.
- Included rheumatic heart disease, peripartum cardiomyopathy, and congenital heart disease.
- Of 33 patients with severe disease, two recovered completely, 13 two recovered completely, 13 are currently admitted, and four are critically ill. The severity of COVID-19 disease was categorized as per the clinical management protocol for COVID-19 (in Adults). Table 1: Pregnancy complication.
In another study between March 1, 2020, to January 31, 2021, the data of 4203 women with COVID-19 were analysed for the present study. Most pregnant and post-partum women with COVID-19 were recruited from the Mumbai metropolitan region (1684, 40%) followed by Vidarbha (1155, 27.5%), Pune (853, 20.3%), Marathwada (351, 8.4%) and Khandesh region (160, 3.8%). Most women (3441, 82%) were in the age group of 18-30 yr, 92 % of the women were in the third trimester and the median gestational age was 38 wks (interquartile range: 36-39). For multiple comparisons to predict the risk associated with disease severity, binominal logistic regression was applied using SPSS Base V26 (SPSS South Asia Pvt Ltd., Bengaluru).
Only 534 (12.7%) women were symptomatic. The COVID-19 disease severity was classified as per the Clinical Management Protocol for COVID-19 (in adults) 17 as mild (382, 71.5 %), moderate (112, 21%) and severe (40, 7.5%). Pregnant and post-partum women aged ≥30 yr had two times higher severity of COVID-19 disease as compared to women aged <30 yr. Among severe COVID-19 cases, the most common presenting symptoms were shortness of breath (34, 85%), dry cough (23, 57.5%) and fever (22, 55%). Of the 494 mild–moderate cases, fever (317, 64.2%) and dry cough (248, 50.2%) were the most common symptoms. Shortness of breath and diarrhoea were significantly higher in severe cases as compared to mild–moderate cases (P<0.005) (Table 2).
| Variable | Severe (n=40), n (%) | Mild-moderate (n=494), n(%) | OR (95% cl) |
|---|---|---|---|
| Age (n=528)3 | |||
| <30 | 21(52.5) | 344(70.5) | Reference |
| ≥30 | 19(47.5) | 144(29.5) | 2.1 (1.1-4.1)* |
| Pregnancy complications versus none hypertensive disorders of pregnancy | 11(47.8) | 51(18.3) | 3.3(1.5-7.0)** |
| Symptoms vs. no symptom | Adjusted OR 95 percent CI | ||
| Fever | 22(55) | 317()64.2 | 0.95(0.4-2.0) |
| Dry cough | 23(57.5) | 248()50.2 | 1.4(0.6-3.2) |
| Shortness of breath | 34 (85.0) | 76(15.4) | 49.1(15.7-154.1)* |
| Running nose | 2(5.0) | 56(11.3) | 0.85(2.15-4.8) |
| Throat pain | 2(5.0) | 44(8.9) | 1.5(0.24-9.2) |
| Cough with sputum | 5(12.5) | 34(6.9) | 2.0(0.6-6.8) |
| Fatigue | 4(10.0) | 27(5.5) | 1.4(0.3-6.0) |
| Nausea, vomiting | 3(7.5) | 24(4.9) | 1.1(0.9-16.4) |
| Myalgia | 5(12.5) | 19(3.8) | 4.0(0.9-16.4) |
| Diarrhea | 2(5.0) | 12(2.4) | 15.7()2.5-100)* |
| Comorbidities versus no comorbidities | |||
| Diabetes mellitus | 1(2.5) | 4(0.8) | 2.1(0.1-36-4)* |
| Chronic hypertension | 2(5.0) | 10(2.0) | 3.8(0.5-29.0) |
| Tuberculosis | 5(12.5) | 7(1.4) | 18.4(4.3-80.0) |
| Hypothyroidism | 4(10.0) | 29(5.9) | 3.1(0.8-12.0) |
| Sickle cell disease | 1(2.5) | 5(1.0) | 4.8(0.4-54.0) |
| Anemia | 28(70.0) | 255(51.6) | 2.8(1.26-3) |
| Multiple comorbidities | 8(20.0) | 47(9.5) | 0.43(0.1-1.7) |
Table 2: Risk factors associated with severity of coronavirus disease-19 in pregnant and post-partum women.
Age was not available for six mild moderate covid-19 women, includes gestational hypertension, pre-edampsia, P*<0.05, **<0.01. Bonferroni correction was applies for multiple comparisons P*<0.005 (0.05/10). OR, odds ratio. Table 2: Risk factors associated with severity of coronavirus disease-19 in pregnant and post-partum women.
There were a total of 34 deaths reported among pregnant and post-partum women with COVID-19. Out of 34 maternal deaths, 10 women died during the post-partum period. Twenty-five women (73%) were ≤30 yr of age while the others were in the age range of 30-45 yr. Women with comorbidities of anaemia, tuberculosis and diabetes mellitus had a higher risk of death (P<0.05) (Supplementary Table). Respiratory failure (22, 64.7%), multi-organ failure (7, 20.6%), acute kidney injury (3, 8.8%) and heart failure (5, 14.7%) were commonly associated with maternal deaths. The overall case fatality rate (CFR) in pregnant women and post- partum women with COVID-19 was 0.8 per cent (34/4203). Higher CFR was observed in Pune (9/853, 1.1%) and Marathwada (4/351, 1.1%) regions as compared to Vidarbha (9/1155, 0.8%), Mumbai metropolitan (11/1684, 0.7%) and Khandesh (1/160, 0.6%). A recent systematic review has indicated that comorbidities such as obesity (OR 2.48), diabetes (OR 5.7) and asthma (OR 2.02) are significantly associated with maternal mortality. The study demonstrates the adverse outcomes including severe COVID-19 disease, pregnancy loss and maternal death in women with COVID-19 in Maharashtra, India.
The study revealed that there were 3,213 live births, 77 miscarriages and 834 undelivered pregnancies. The proportion of pregnancy/foetal loss including stillbirths was 6%. Five hundred and thirty-four women (13%) were symptomatic, of which 382 (72%) had mild, 112 (21%) had moderate, and 40 (7.5%) had severe disease [14]. • Maharashtra: In their first large-scale study report of systematically collected, multicentre data on the clinical presentation, pregnancy outcomes and maternal deaths amongst women with Covid-19 in Maharashtra, it was observed that nearly 30% of the symptomatic cases had moderate to a severe disease requiring ICU/HDU admission. The experts analysed data of 4,203 women with Covid-19 for the study. Most pregnant and post- partum women in Maharashtra with Covid-19 were recruited from the Mumbai metropolitan region (1684, 40%) followed by Vidarbha (1155, 27.5%), Pune (853, 20.3%), Marathwada (351, 8.4%) and Khandesh region (160, 3.8%). The experts analysed that most women (3441, 82%) were aged 18-30 years, with 92% being in the third trimester and the median gestational age was 38 weeks.
Out of 4,203 women, 3,865 were registered during their ongoing pregnancy and 338 were enrolled during the post-partum period. According to the study, majority (3669, 87.3%) of the pregnant and post-partum women with Covid-19 were asymptomatic and only 534 (12.7%) were symptomatic. The study found that pregnant and post- partum women above 30 years of age had “two times higher severity” of Covid-19 disease as compared to women aged less than 30 years of age. The study revealed that there were 3,213 live births, 77 miscarriages and 834 undelivered pregnancies. The proportion of pregnancy/foetal loss including stillbirths was 6%. Five hundred and thirty-four women (13%) were symptomatic, of which 382 (72%) had mild, 112 (21%) had moderate, and 40 (7.5%) had severe disease. Among severe Covid-19 cases, the most common presenting symptoms were shortness of breath (34, 85%), dry cough (23, 57.5%) and fever (22, 55%) [14]. • Karnataka: While precise number or proportion of Covid 19 infected or vaccinated is not readily available, HOD of OB & Gynaecology. Department of Vani Vilas hospital, Bengaluru. Most private Obstetricians in Bengaluru endorse that nearly 50% of pregnant women were RTPCR positive but less than 20% had any symptoms in the recent 3-6 months. In the second wave, many pregnant women who contracted Covid 19 had faced abortions, premature deliveries, and needed management in ICUs as compared to the current phase where most of them had fever and minor symptoms for 3-5 days. Most Covid 19 infections found positive are incidental following a mandatory test in the hospitals. HSIS Gosha hospital, Bengaluru a dedicated Covid-19 hospital, reported only 3 out of 90 women delivered in January 2022, had their Baby positive for Corona virus [15]. In conclusion it can be inferred that every pregnancy starts out with a 3-5% chance of having a birth defect, known as the background risk. The available studies and reports on COVID-19 infections in pregnancy have not reported birth defects related to COVID-19. Fever is a possible symptom of COVID-19. A high fever in the first trimester can increase the chance of certain birth defects.
Studies have shown that people who are pregnant or recently pregnant and have COVID-19 have a higher chance of becoming very sick than people who are not pregnant or recently pregnant. This includes higher chances of being admitted to intensive care and needing to be put on a ventilator (machine that helps you breathe). Some studies have also reported a slightly higher chance of death from COVID-19 among people who are pregnant. The chance of these outcomes is higher among pregnant people who also have other underlying health conditions, such as obesity, pre-pregnancy diabetes, and/or chronic hypertension, and among those who are not fully vaccinated against COVID-19. Having COVID-19 in pregnancy increases the chances of preterm delivery (having a baby before 37 weeks of pregnancy) and stillbirth, and some studies have reported increased chances of preeclampsia (dangerously high blood pressure) and the need for emergency C-section. The chance of pregnancy complications appears to be higher if the person with COVID-19 has symptoms (symptomatic) than if they do not have symptoms (asymptomatic). Pregnant people who are fully vaccinated are expected to have less severe symptoms if they get COVID-19. Researchers are gathering more information about pregnancy outcomes in fully vaccinated people. More research will also help us learn how the timing of an infection in pregnancy affects outcomes. In rare cases, the virus can infect the placenta (called placentas), which can lead to problems with how well the placenta works to support the pregnancy and the baby’s growth and development. Some cases of stillbirth have been associated with placentas from a COVID-19 infection. Researchers are learning more about other possible effects of placentas caused by a COVID-19 infection.
COVID-19 infection can increase the chance of developing blood clots, especially if the infection is severe. One study of women giving birth in hospitals reported that those with COVID-19 had a higher chance of heart attack and blood clots than those who did not have COVID-19 (even though the overall chance of heart attack or blood clots was still small). The American Society of Haematology recommends that all adults who are hospitalized with COVID-19 be given treatment to prevent blood clots. People who are pregnant and admitted to the hospital with COVID-19 should discuss treatment options with their healthcare providers.
In reports of infants born to people with COVID-19 around the time of delivery, most new-borns have not had evidence of infection. However, the virus has been found in the (umbilical) cord blood and amniotic fluid of people who have COVID-19 at or near the time of delivery, and a small number of new-borns have tested positive for the virus soon after birth. Although this suggests that the virus could pass from a person who is pregnant to their baby during pregnancy, this appears to be rare. The chance of the baby getting the virus during or shortly after delivery may be higher if the mother has an active infection at the time of delivery. However, most infants who test positive have only mild or no symptoms, and fully recover from the virus. Severe illness in babies is rare, although it may be more likely in infants who are born preterm or have other health problems [16].
Vaccinating Pregnant women
One of the biggest sources of concern was the lack of data showing beyond doubt that the vaccine was safe in women. Now that COVID-19 vaccines have been given to millions of people, studies are showing they are safe in pregnancy. By now, millions of pregnant women have been vaccinated worldwide and no safety concerns have been identified.
When the COVID-19 vaccines were undergoing clinical trials in 2020, pregnant women were excluded, as is standard practice with new treatments or vaccines. From the beginning, scientists could provide robust evidence to show there was no reason to believe vaccines wouldn’t be safe in pregnancy. But this lingering uncertainty over safety reflects in vaccination numbers even today.
A study published in September 2021 showed that half the people surveyed reported disrupted menstrual cycles due to COVID-19-related stress rather than infection or vaccination. Research shows no difference in pregnancy success rates among women who have been vaccinated compared to those who had the disease or were never infected despite temporary blips in periods. The overall inference of the research and observations so far indicates that the vaccine is a more controlled imitation of the body’s response to infection and gives our immune system the chance to learn how to recognise a pathogen, while reducing the chance of it making mistakes and self-reacting. Therefore, COVID-19 infection is always going to be more dangerous for a pregnancy than the vaccine. Getting vaccinated is the best way to protect mother and the babies. Moreover, pregnant women can pass on antibodies against COVID-19 to their babies, giving them added protection [17].
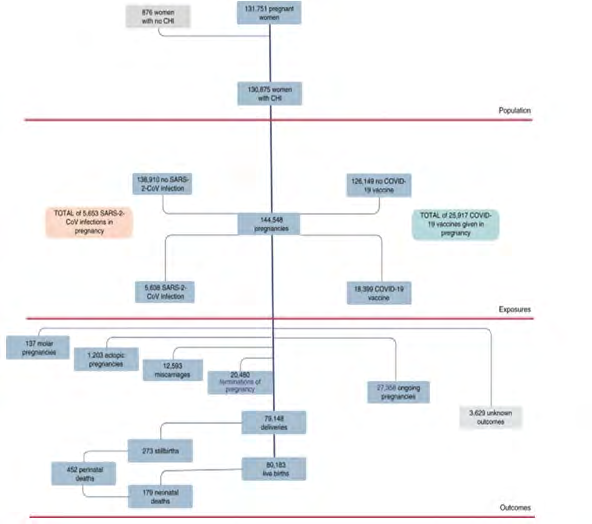
Between the start of a COVID-19 vaccine program in Scotland, on 8 December 2020 and 31 October 2021, 25,917 COVID-19 vaccinations were given to 18,457 pregnant women. Vaccine coverage was 32.3% of women giving birth in October 2021 had two doses of vaccine compared to
77.4% in all women. Between 1 March 2020 and 31 October 2021, there were 5,653 confirmed SARS-CoV-2 infections in pregnancy. Overall, rates of SARS-CoV-2 infection in pregnancy showed similar patterns to those in the general female population of reproductive age, with peaks of infection in October 2020, January 2021, and September 2021.
The extended perinatal mortality rate for women who gave birth within 28 days of a COVID-19 diagnosis was 22.6 per 1,000 births. Overall, 77.4% of SARS-CoV-2 infections, 90.9% of SARS-CoV-2 associated with hospital admission and 98% of SARS-CoV-2 associated with critical care admission. All baby deaths had occurred in pregnant women who were unvaccinated at the time of COVID-19 diagnosis. Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic [18].
Covid 19 Vaccination for Pregnant Women in India
On 2 July 2021 Indian Government approved vaccinating pregnant women. As per a GOI response in writing to Rajya Sabha as of 2 February 2022 28.22 lakh doses are reported to have been given to pregnant women and 11.68 Lakh PWs had got both doses. Among those vaccinated by 31 January 2022, 64 had some adverse reactions of which 38 were severe in nature.
With the birth of 25 million children India accounts for nearly 26.25 million pregnancies each year. As of 2/7/21 the country had an estimated 16 million (60% of annual pregnancies that could have been recognized as pregnant) pregnant women and added 2 .2 million pregnancies every month, taking the total of eligible to 25 million in the last 7 months of which we protected only 1.17 million a meagre 5%. We also know the data from private sector may be missing. Even if we add an equal number the protection will not beyond 10% of the eligible by no means a tall claim.
Conclusion
Despite the increasing number of published studies on COVID-19 in pregnancy, there are insufficient good-quality data to draw unbiased conclusions about the severity of the disease or specific complications of COVID-19 in pregnant women, as well as vertical transmission, perinatal and neonatal complications.
The long-term adverse effects and safety of the vaccine for foetus and child is not established yet. Very rarely (one in 1 to 5 lakh persons), the pregnant women may experience some of the symptoms like Shortness of breath, Chest pain, persistent abdominal pain with or without vomiting, Pain
in limbs/pain on pressing the limbs or swelling in the limbs (arm or calf), petechiae or bruising of the skin occurring, Persistent vomiting without any obvious reason, Seizures with or without vomiting, Severe and persistent headaches with or without vomiting (in the absence of the previous history of migraine or chronic headache), Blurred vision/ pain in eyes, Weakness/paralysis of limbs or any particular side of the body, within 20 days after receiving any COVID-19 vaccine need immediate attention.
Pregnant women must get a COVID-19 vaccine during pregnancy, as it helps both mother and her foetus and as pregnant women have a higher risk of severe illness from COVID-19 than nonpregnant women. The vaccines are very effective at preventing infection, severe illness, and death from COVID-19. The reports show that these women have had similar pregnancy outcomes.
When pregnant mother gets vaccinated, the antibodies made by her body pass to the foetus that help protect the baby from the virus after birth, though how much protection is given is not known.
References
-
Jumaat F (2020) Impact of COVID-19 on Pregnancy and Maternal Health. Biomedical research and therapy 8(1): 4655-4667.
-
(2020) How covid-19 impacts women and girls.
-
Kushwaha S (2021) Biological attributes of age and gender variations in Indian COVID-19 cases: A retrospective data analysis, Clin Epidemiol. Glob Health 11: 100788.
-
(2021)Women and COVID-19 in India.
-
(2021) Investigating the Impact of COVID-19 during Pregnancy, coronavirus.
-
(2022) Coronavirus (COVID-19), Pregnancy, and Breastfeeding: Lisa Hollier, Baylor College of Medicine, Houston, Texas.
-
(2020) coronavirus-pregnancy/covid-19-virus- infection-and-pregnancy.
-
(2020) COVID-19 Pandemic Leads to drop of Maternal Health Care in Africa, Raising Fears of Increased Mortality.
-
José Villar (2020) Maternal and Neonatal Morbidity and Mortality Among Pregnant Women with and without COVID-19 Infection, The INTERCOVID Multinational Cohort Study.
-
(2021) Counselling Pregnant Women for COVID-19 Vaccination pp: 1-8.
-
Singh AK (2020) Impact of COVID-19 pandemic on maternal and child health services in Uttar Pradesh, India.
-
(2022) Effect of the COVID-19 pandemic on deliveries and home-based new-born care in India, By Sam Hancock, Reviewed by Danielle Ellis, B.Sc.
-
Niraj P, Mahajan N (2020) Pregnancy Outcomes and Maternal Complications During the Second Wave of Coronavirus Disease 2019 (COVID-19) in India, Obstet Gynecol 138(4): 660-662.
-
Thacker T (2021) Many-pregnant-women-likely-to-get- sick-from-covid finds new ICMR study.
-
Sunitha R (2022) Positivity among pregnant women rising in Bengaluru.
-
(2022) COVID-19. Mother to baby.
-
(2022) COVID-19 vaccines and pregnancy, here’s what you need to know.
-
Stock SJ (2022) SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda