Want a Horse to Run but not Eat? Conflict Objectives and Policy Dilemmas in China’s Medical Reform
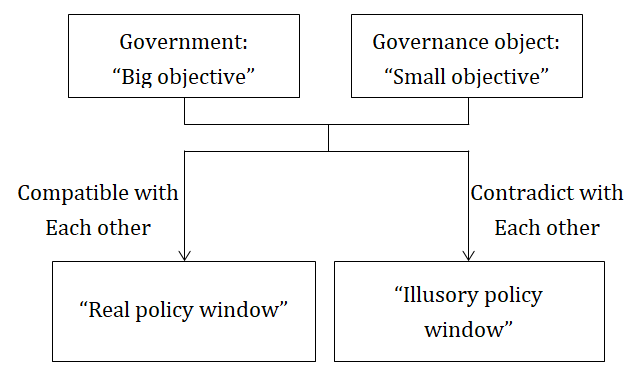
Medical reform is not only closely related to the interests of the public, but it also reflects the interdependence of government, the market, and society. Within a country’s medical reform coexists the “big objective” of the government and the “small objective” of the governance object. Their interactions will affect the policy stream and the policy window. If the “big objective” is compatible with the “small objective”, then the “real policy window” will open. If the two are in conflict, they will grind together, enlarging the discretion of the governance object. The result will be the opening of an “illusory policy window” that will slow the policy reform or even hinder it. The multiple reforms of the Chinese medical industry are the result of the four competitive governance logics coexisting in public hospital governance. The first two-the country’s logic (public welfare dominant) and bureaucratic logic (executive order-led) -have shaped the “big objective” of public welfare. Enterprise logic (market-oriented) and the logic of professional organizations (led by experts) have shaped the “small objective” of effective operation. The conflict and balance between “big objective” and “small objective” have seriously affected the process of Chinese social policy reform.
Introduction
Medical reform is a popular and difficult issue in academia and politics. It promises to promote social welfare through national legislation or government administration. It also directly affects people’s interests and their evaluation of government. Medical reform reflects the interdependence between government, market, and society, as well as the competition between various stakeholders.
In developing countries like China, India, and Brazil, medical policy reform is even more important. With large populations, scarce resources, and obvious regional differences, these developing countries must ensure economic growth and deliver public services through effective governance [1, 2, 3]. Existing research focuses mainly on developed countries like the United States or Europe. Studies of China’s medical reform tend to concentrate on the vertical or horizontal relationships within government. Observations of the dynamic interactions between government and governance objects are scarce. The institutional logics and policy dilemmas in the process of medical policy reform deserve further research. In this article, we ask two general questions. First, in the context of different countries, how do interactions between the government and the governance objects affect medical policy reform? Second, what are the institutional logics and policy dilemmas behind the tortuous changes of medical policy in a specific country?.
Current Chinese medical policy reform studies usually regard government as leading resource allocation and agenda setting, but they ignore the role of the governance object. Although these organizations can’t participate in the national agenda setting process, their “small objective” will offset the government’s “big objective” in policy reform. This paper argues the continuous interaction between government and governance object will influence the formation of the policy stream and finally influence the effect of the policy window. When the “big objective” of national governance is compatible with the “small objective” of the governance object, a “real policy window” opens; when the two objectives are in conflict, the grinding of the objectives will enlarge the discretion of the governance object and an “illusory policy window” will open to slow down or even hinder policy reform. This is because the policy objectives of government and the governance object are created separately by their own organizational logics. When those are in conflict, their different objectives will slow the progress of policy reform and influence the effect of policy implementation.
The “government-governance object relation” studied in this paper is different from the “central-local government interaction” studied in other literature. Even though both research paths involve policy deviation and policy failure [4], interactions in the former are more complex. The game of interests played between different levels or departments reveals the internal coordination of policy subjects within the government. The “government-governance object interaction” investigated in this paper is not only influenced by government policy subjects but is also affected by the governance objects (enterprises, institutions etc.). Essentially, this is a break-in problem between different organizations. It shows the tortuous pathway facing medical policy reform as well as the intriguing interplay of practical governance.
This paper takes medical and health-care reform as the starting point to explain the social policy evolution of centralization, decentralization, and recentralization in China. The author believes the “big objective-small objective” interaction between government and governance object should not be ignored in medical policy reform in any country, because the process of policy reform is influenced by both organizational goals. The “big objective” is the macro-policy objectives and governance logic of government. The “small objective” is the governance object’s own microstructure goals and operation logic. If the two objectives are aligned, they may boost, strengthen, and accelerate the impact of top- down pressure and help open a “real policy window”. If not, even needed changes can be delayed or even suppressed and the impact of top-down pressure and target implementation may open an “illusory policy window”. Only by realizing the compatibility and coordination between these two objectives can medical policy reform be achieved smoothly.
In addition, based on long-term investigation of many hospitals in central China, this study took China’s public hospital reform to examine how the above “big objective- small objective” framework works in Chinese medical policy reform and shapes the tortuous process of public hospital reform. This paper claims that “public welfare” and “effective operation” are contradictions in Chinese public hospital governance. “Public welfare” represents the priority objective of government (“big objective”), while “effective operation” embodies the priority objective of the governance object (“small objective”). These two different policy objectives are determined by their separate organizational logics, namely, the country’s logic (public welfare dominant) and the bureaucratic logic (executive order-led), respectively. These two logics have shaped the “big objective” of public welfare. But enterprise logic (market-oriented) and the logic of professional organizations (led by experts) have shaped the “small objective” of effective operations in Chinese public hospitals. And the complexity of Chinese medical reform is that at present these four logics are embedded, restrict each other, cause serious internal friction, and lead to policy dilemmas.
This paper contributes to our understanding in three ways. First, it expands the research vision of Kingdon’s Multiple Streams Model [5]. No longer limited to research within a single type of organization (such as: government- government), this study has expanded it to interactions between different types of organization (such as: government- enterprise, government-institution). We claim the constant interaction between government and governance object will affect the process of medical policy reform. In the top- down diffusion of policy goals, it is inevitable the governance object will influence policy goals. Government can allocate resources, set the agenda, and assess progress, but someone must do the work [6]. Each governance object has its internal development goals and needs; they cannot be ignored. This is the important internal environment of policy change, which reflects the efficiency mechanism of the organization [7].
Second, this paper examines Chinese medical policy reform to elaborate on the run-ins between the “big objective” and the “small objective”, how different organizational logics shape their different organizational goals, and the cause of the policy dilemma that delay real changes. This further explains why medical policy reform in a given country can be slowed or even halted. Because, for example, in China, in policy mobilization or assessment, the governance object may respond to the “big objective” by temporarily making the government’s objective play a leading role. But, as time goes on, the governance object’s “small objective” will become the main target again. As the “big objective” of the reform policy is diluted, delayed, or hindered, the process of policy reform will cycle through will new policies or even stagnate.
Third, this paper analyzes the deep reasons of conflict objectives and policy dilemmas in medical policy reform in China’s health-care reform, but our framework and conclusions have wider research significance. For health (government-pharmaceutical enterprises interaction), housing (government-real estate enterprises interaction), education (government-university interaction), and the environment (government-industrial enterprises interaction), the “big objective-small objective” framework and conflicts in governance logics have explanatory power, and the research results of this study have significance for social policy research in other countries.
Insight into Policy Dilemma: “Real Policy Window” or “Illusory Policy Window”?
Existing research on China’s medical policy failures are mostly studies of horizontal and vertical relationships within the government. But in the real medical policy reform process, the governance object is not completely in a supporting role. Rather than passively and blindly response or accept policy, it constantly weighs the pros and cons and compares the external “big objective” with its internal “small objective”. When the “big objective” is consistent with the “small objective” or without substantial conflict, the governance object will comply with the government’s objective for policy reform. Its response can boost, reinforce, and even accelerate national top-down pressure and a “real policy window” can open.
But, when the “big objective” competes or conflicts with the “small objective”, the governance object will either support the “big objective” ostensibly, but through the process of policy interpretation and implementation within the organization, it will blend in their organization’s “small objective”, thus offsetting the effect of “big objective”. Or, in the short period of policy mobilization and assessment, the governance object will temporarily comply with government “big objective” or identify the “big objective” as a priority in response to external pressure or to seek the survival and development of the organization. When these critical period passes, the governance object will instinctively go back to its original “small objective” as a priority. Thus, it will breach, change, delay, and even restrain the national top-down pressure of medical policy reform. In this case, the medical policy reform opens only the “illusory policy window”. The various forces will not integrate the resources of stakeholders and will slow down or even distort policy intentions. The reform’s timeliness is unlikely to be met. From this perspective, it is not difficult to understand why many social policy reforms have twists and turns.
From the perspective of government, there is a convergence of the politics stream, the problem stream, and the policy stream. A policy entrepreneur may also play a positive role. The opening of the policy window seems inevitable. However, in the process of policy making by the government, the “small objective” and operational logic of the governance object can be ignored. Again, from the government’s perspective, it has all kinds of formal or informal means of pressing the governance object to take up the reform, such as resource allocation, project promotion and even political mobilization. It can interrupt or even rearrange the governance object’s priorities of work, can affect the governance object’s attention allocation, or force it to deal with and carry out the policy orders passively. A singular focus on the national “big objective” that ignores the governance object’s “small objective” is very unwise and lacks foresight. The best it is likely to do is open an “illusory policy window”.
From the perspective of the governance object, the legality mechanism and the efficiency mechanism are two important mechanisms for the operation of the organization. According to the literature of institutions, the legitimacy mechanism of social culture and institutional facilities is the basis of institutional organization. However, the efficiency mechanism emphasized in economic literature is also an important consideration for the organization. These two distinct organizational development environments and the different goals derived from them are sometimes contradictory. The legality mechanism requires an organization to accept and adopt a universal approval method. It must avoid the “crisis of legitimacy”, regardless of whether these practices are efficient. The efficiency mechanism advocates the organization to pursue efficiency and to run the organization as best as possible. Therefore, the actual operation of the organization is a struggle between the two objectives, and the need to adapt the efficiency mechanism often leads to the organization ignoring the legality mechanism. And the response to the legality mechanism often conflicts with the organization’s efficiency mechanism. Only by realizing the compatibility and coordination between these two objectives can the “real policy window” be opened (Figure 1).
In China, for example, a striking feature of top-down policy is the united policy goal for a huge population with obvious regional differences spread over large distances. No policy maker could ever fully consider all these areas and the different organizational cultures that might be affected. It is impossible to have enough resources or the ability to fully understand and effectively regulate all the governance objects. Therefore, the “small objective” of a grassroots organization is ignored in the process of policy design. From the micro perspective, the governance object is the real carrier of policy reform, the organization’s “small objective” will play an imperceptible role and directly affect the organization’s operational efficiency, determine the effect of the policy window, and ultimately affect the process of medical policy reform.
The tortuous path of Chinese medical and health-care system reform is a true reflection of this phenomenon. Since 2009 and the implementation of new healthcare reform, all levels of government have developed numerous policies. With strong policy instructions and political pressure, some irregularities were changed in a short period of time. But relapse is inevitable. These reforms, to the extent they changed anything, have only been allowed to “cure the symptoms”.
To sum up, opening a “real policy window” requires not only the convergence of the political stream, the problem stream, and the policy stream, and the promotion of policy entrepreneurs [8], but also a government willing to pay attention to and recognize the “small objective” of the governance object. To achieve compatibility between the “big objective” and the “small objective”, conflicts among multiple policy objectives must be avoided lest they magnify the discretion of the governance object, dilute the effect of the government’s “big objective”, and delay or even hinder the process of social policy reform.
Horses: Caged, Scattered, or Mixed Feeding? The Path of Chinese Medical and Healthcare Reform This article takes the Chinese medical and healthcare system reform and the public hospital reform as examples to illustrate China’s centralized and decentralized governance path and its influence on medical policy reform.
External government regulation and internal environment are foundations of the organization. The medical and healthcare system of any country is determined by its economic and political systems [9, 10]. China is unique when compared with other countries. Its healthcare reform has been a process familiar to traditional authoritarian governments which cycle through centralization and decentralization. These cycles can be roughly divided into three, namely, the state does everything period, the market- oriented period, and the state-led period. For purposes of exploring contemporary China’s medical and health-care system reform, this article will start from 1949 (Table 1).
| Period | Major difficulties | Primary goal | Governance model | Governance characteristics |
|---|---|---|---|---|
| 1950s-1970s | inadequate supply of medical services, low level services | coverage, accessibility | centralization | the government does everything |
| 1980s-1990s | Government’s financial difficulties, slow development of pharmaceutical industry and public hospital | efficiency | decentralization | government relinquishes power and profit |
| 2000s to date | difficult and expensive to seek medical care | quality | moderate centralization | strengthen government accountability, encourage the market to work well |
Table 1: Three period of Chinese health-care reform.
The State does Everything Period: Horses in Captivity (1950s-1970s)
After the People’s Republic of China was founded in 1949, its leaders faced a vast territory, a large population, a weak economy, an imbalance in regional development, and the influence of the Soviet model. China’s political system and governance model throughout this period centralized state power over the economy and society. At the same time, it strengthened the political leadership of the central government in some areas of public service supply so that market effects were ignored, weakened, or even eliminated.
China’s medical and health-care system was also highly centralized system. First, in public hospital governance, the hospital dean was under the leadership of the Party committee and the decision-making power is highly concentrated. The dean was appointed and evaluated by the government. Governmental instructions about day-to-day management were followed. Punishments and incentives also depended on the evaluation of the government. Inside the public hospital, the management system was like an administrative department. The medical staff was managed according to the establishment; subordinates obeyed their superiors and acted according to the instructions of the superior. The government’s financial management of public hospitals adopted “unified collection and allocation” (1950s), or “classification management, fixed allowance, all-in budget” (1960s), and all the medical staff wages were included in the state budget.
Secondly, in the 1950s, medical insurance was established through the social insurance system for urban workers as well as civil servants. The rural cooperative medical system also gradually became a fixed part of government after springing up spontaneously. As of 1976, China had about 90% of farmers taking part in the cooperative medical care system. The establishment of the medical systems laid down the public welfare orientation of basic medical and health services during this period.
Finally, during this same period, the government took control of the pharmaceutical industry. It ordered comprehensive controls for drug prices based on a three-level system that determined the ex-factory price, the wholesale price, and the retail price. In 1954, public hospitals were operating at a loss. The government allowed them to have a 15% premium on drug prices as part of the public hospitals’ income. As a compensation mechanism, this kind of “medicine for the doctors’ wage system” at that time was beneficial. It maintained the normal operation and development of public hospitals. But a danger was also planted. As times changed, public hospitals began chasing their own interests in the late 20th century.
To sum up, China’s medical and health institutions at all levels during this period were the state machine’s nerve endings. Public hospitals and doctors didn’t want to pursue profits, state governance offered “weak development, strong control”, and the medical and health-care system had the characteristics of public welfare.
Within that political and economic environment, the state does everything model could quickly and effectively integrate resources and provide a low level but wide coverage of medical and health services. Without a profit motive, medicine and health-care costs were effectively controlled. This public health system gradually became the dominant force in China’s basic medical and health service supply. In the 1970s, 80% to 85% of China’s population had basic medical and health-care services. This kind of low cost, wide coverage system was hailed as a model of public health services around the world [11].
At the same time, with the continuous development of the economy and society, the strong government and weak industry mode was increasingly showing its limitations. Due to the path dependence effect of centralization, government at all levels carried too many governance functions and were increasingly overwhelmed and unsustainable. Dominated by the central government, political mobilization was the main lever of social policy reform. This depressed the market’s vigor and considerably slowed down the long-term development of the nation’s economy and society.
To sum up, the wild horse was living in a paddock. Away from the natural world, it avoided starving by being captive to a master. Under the master’s absolute authority, it survived but did not thrive. The wild horse faded as it got used to not being free.
Market Dominant System: The Period of Horses in Free-Range (1980s-1990s)
Since 1978, decentralization and the reduction of the government’s burden had become an important goal of national governance. As in the previous period, the reform of China’s medical and health-care system followed the nation’s social and economic changes. The central government gradually delegated its power to local governments. The push and pull of decentralization gradually became the main theme of the central local relationship, and the corporatization of public institutions gradually became an important feature of social development.
In public hospital governance, under the dominant idea of “only policy but not money” and “construction relies on the state, eating depends on oneself”, the government’s financial management system for public hospitals adopted a “fixed allowance, release of power” (1980s) which called for significantly reducing the proportion of financial compensation and increasing the proportion of business income. In 1987, the average business income of hospitals had expanded by 4.1 times compared with 1980. However, the proportion of state budget appropriation for hospital revenue decreased from 23.87% in 1980 to 10.18% in 1987. The government gradually “expanded health institutions’ autonomy” (1990s). At the same time, government continued to maintain its ownership and authority in public hospitals through appointment of the hospital dean, establishment management of medical staff, and regular assessment. Under this development orientation, scale expansion became more important than public welfare in public hospitals.
Regarding healthcare, the disintegration of the people’s commune directly resulted in the loss of the organizational foundation of cooperative medical care which had played a huge role in the countryside. The rapid decline in the coverage of cooperative medical care led to a 20 year “gap” in medical care for the roughly 70% of China’s population living in farming communities. This would not be restored until the promotion of a new rural cooperative medical [6].
Regarding medical and pharmaceutical relations, local governments had to be enticed to rapidly stimulate the pharmaceutical industry, so the central government gradually ceded power to them. They were encouraged to support pharmaceutical enterprises and develop public hospitals. As a result, private pharmaceutical companies proliferated, and public hospitals across the country increased their beds and buildings as the main means of expansion. Due to their low investment thresholds and technical abilities, these private companies had no advantage in market competition. Many resorted to kickbacks to doctors, public hospitals, and related pharmaceutical administrators through “pharmaceutical sales representatives” as a shortcut to expand drug sales. As the government’s financial input ebbed, doctors’ salaries remained relatively low. This was totally incompatible with doctors’ social status, professional input, and hard work. Much like the compromise around drug sales to benefit the hospitals in the 1950s, doctors received enormous kickbacks from pharmaceutical sales representatives and pharmaceutical enterprises. The public hospitals and their doctors had strong profit motives that influenced the direction of their non-profit medical institutions. Predictably, seeking medical care became very difficult and expensive [12].
During this period, the governance theory was “strong development, weak control”. The government’s supervision of the medical and health-care industry deferred to the development of the industry. At that time, it alleviated the problem of low efficiency and inadequate supply of medical services. However, decentralization in national governance caused a shortfall in the government’s fiscal subsidies. Cash-strapped hospitals had limited funds, enterprises had an incentive to bribe hospitals, patient-doctor information asymmetry, etc., led to the short-term development-oriented behavior of China’s local governments and public hospitals. Chinese health-care reform during this period reflects the multiple game of economic development and social transformation.
In conclusion, due to the limited resources and energy of the master, the life of the horse begins to change. The master cuts down on feeing the horse but lets it out of the paddock. If the ownership of the horse is in the master, the master does not limit where the horse forages for food. The horse goes again into the wild, appreciates the charm of freedom, experiences the struggle of finding food sources, and gradually starts growing again.
Government-Led System: The Period of Horses’ Mixed Feeding (2000s to Date)
Since the late 20th century, with the rise of regulatory national construction around the world, the Chinese government began to gradually change the structure of governance through deregulation in the economic field and increased supervision in the social field. Policy reforms are usually triggered by a public crisis or social conflict. Whenever a country encounters significant challenges or a serious failure in bureaucracy, the mobilized governance mechanism will become an effective choice.
Similarly, in the field of healthcare, every time a major public health event occurs and the system is found inadequate, medical and health-care system reform is triggered. After government decentralization and the outbreak of the SARS crisis in 2003, the Chinese government began to re-think the public service supply system. This was the beginning of China’s “administrative accountability system”. The government reintegrated the medical and health-care system reform into important issues of governance, and government input into the system began its slow recovery.
Public hospitals were the main body of China’s medical service system, so they became the focus of reform. On March 17, 2009, China initiated a new medical and healthcare reform and made public hospital reform the key content of this reform. On February 11, 2010, six national ministries jointly issued <The guidance on the pilot reform of public hospitals>, marking the newest period of China’s public hospital reform. Compensation was modified from the old system of “rely on three channels” (fiscal subsidies, service charge and drug income) to “two channels” (fiscal subsidies and service charge), reducing the direct relationship between drug income and doctors’ salaries. At the same time, medical and health-care system coverage expanded, from 11% in 1949 to the current coverage of over 95%.
In medical and pharmaceutical relations, the government began to regulate the distribution of drugs, trying to break the grey interests between pharmaceutical companies and public hospitals and doctors. On December 26, 2016, the state council medical reform office together with seven national ministries issued a document, to carry out the “two invoice system”, in order to “regulate the circulation of drugs, reduce the price and purify the circulation environment”. This is an important policy directive released by the government for reform of drug circulation and the “medicine for the doctors’ wage system” in public hospitals.
It is apparent the government intended to interrupt or stop the behaviors of the governance object subjectively, hoping through top-down policy mobilization it could accomplish specific policies. Things did not go so smoothly. The government’s good original intention inevitably affected the vested interests of stakeholders. Conflicts and frictions occurred between the government’s “big objective” and the governance object’s “small objective”. What the government wanted was “a horse to run but not to eat”. Despite the reforms, Chinese citizens still find “seeking medical care very difficult and expensive” [13]. Government regulation of health care in the form of “strong development, strong regulation” is illusory. the government needs to transform from “cover all” into “limited field”, from “excessive control” into “moderate control”, from “lack of control” to “strengthen control” in medical policy reform.
To sum up, when the master let the horse work in the past, the horse was willing to work hard and sincerely, never caring about personal gain or loss. However, when the master let the horse work again after being free, the horse not only has special requirements, but also likes to bargain. Adapted to growing in a free environment, accustomed to the pleasure of grazing, the horse is unhappy with the master’s constraints. It is even willing to defy the master’s orders for its own benefit. When the master becomes gradually aware of the previous liberal style of management is now unable to control the increasingly strong horse again, it’s too late. The master must find a balance between the horse’s individual will and the master’s to achieve effective governance of mixed feeding.
Conflict Objectives and Policy Dilemmas in Public Hospital Governance: Public Welfare and Effective Operation
Taking China’s public hospital reform as an example, this paper elaborates on the “big objective-small objective” framework. The purpose is to examine the deep institutional logics behind those objectives and how a “real policy window” or an “illusory policy window” may be opened.
The legality mechanism and the efficiency mechanism are two important mechanisms of organization [7]. However, these two distinct perspectives are sometimes contradictory. With the new health-care reform of the 2000s, the government gradually shifted from “the state does everything system” under the centralization regime to the “market dominant system” under decentralization, and eventually to the “government-led system”. Public welfare and effective operations are the profound tensions in China’s public hospital governance. The government requires public hospitals to provide cheap and sufficient public services, but the public hospitals operate effectively with reduced investment from government. Good quality at a low price as far as possible is a fine public health goal but the lack of profit motive weakened China’s public hospitals. But, once profit-making was allowed, the public hospitals began to shirk their responsibilities to the broader public.
For China’s public hospitals, the above conflict between the government’s “big objective” with the governance object’s “small objective” is easy to see. In the process of policy implementation, public hospitals must balance these interests. When the “small objective” is compatible with “big objective”, then it opens the “real policy window”. If the two objectives are in conflict, then an “illusory policy window” will open, thus shaping the undulating history of China’s medical policy reform.
Four Coexist and Competing Governance Logics
The objectives of the government and governance objects are shaped by the logics of their organizations. The conflict between the government’s “big objective” (public welfare) and the public hospital’s “small objective” (effective operation) is made up of four competing governance logics. They are the country’s logic (public welfare dominant), the bureaucratic logic (executive order-led). These two logics have shaped the “big objective” of public welfare. The enterprise logic (market-oriented) and the logic of professional organizations (led by experts) have shaped the “small objective” of effective operations in Chinese public hospital governance. In contemporary China, the four logics are embedded into and restrict each other. The internal friction is serious enough that it may lead to magnifying the discretion of the governance object. This is how an “illusory policy window” can open and a governance dilemma appears.
Logic of the State: Policy Orientation and Public Welfare Needs: Public hospitals are non-profit, public institutions organized by the state. They are an important part of China’s medical and health-care industry. From this perspective, public hospitals’ properties and mission determine their public welfare characteristics and should reflect the demands of the government and public. However, every organization must coexist with its environment. To survive and develop smoothly, public hospitals had to exchange resources with a rapidly changing society. As a result, they became embedded in a certain culture and are bound to its social and institutional environment [14].
In China, government is the main actor in institutional environments. As the largest unitary state in the world, governments at all levels have the dominant power of resource allocation and social governance. All aspects of national governance will be deeply affected by government policies. Government at all levels, especially the central government, can influence the distribution of attention. They control personnel changes, resource allocation, project promotions, and political mobilization. They can interrupt or reschedule the priorities of their governance objects [15]. Driven by the country’s unified system as governance objects, public hospitals will inevitably follow the policy guidance, or cleverly deal with and carry out the top-down policy instructions. At the same time, they look out for their own survival and development space between the gaps in the system environment and policy pressure.
At the macro level, especially when a public health crisis triggers medical and health-care reform, government at all levels will intervene in the daily operations of public hospitals through policy mobilization, inspection comparison, evaluation, and motivation. The effect of any “big objective” on public hospitals will be the most significant at this time. The medical and health-care reforms and national governance introspection after SARS in 2003 is the best example.
On May 5, 2017, the state council issued a document that stressed “we should have one local principal leader (either from Party committee or local government) act as leader of ‘group of deepening the reform of medical and health-care system of local government’ and should build the constraint mechanisms of local government leaders’ assessment by including the reform effect”. Along with health-care effects gradually being included into local officials’ performance evaluations, officials at all levels will be more sensitive and pay more attention to medical and health-care policy and instruction. The influence of policy orientation on public hospitals will also grow.
The imprinting of the unified system logic has deeply affected the daily operations of public hospitals. For them, the policy-oriented logic shapes the corresponding institutional environment, affects the strategy selection and response behavior of public hospitals, and determines the policy orientation and public welfare demand of the institutional environment for public hospital governance.
Logic of Quasi-Bureaucratic System: “Upward Responsibility System” of the Hospital Dean: Max Weber defined a bureaucratic organization as a formal hierarchy run by rules; he believed a formal organization characterized by bureaucratic hierarchy is the organizational form of modern society [16]. The basic characteristic of bureaucratic organization is a set of organizational structures with clear power relations and hierarchy. Through a series of formal regulations, professional personnel can improve the efficiency of decision making and policy implementation. In the policy implementation process, through the high mobilization of governments at all levels, instructions will be decomposed and layered, and the pressure system will be generated.
Bureaucratic organizations often use an agency system to stair-step their administrative power. Lower levels of government will be entrusted with providing public goods, economic development, social stability, employment promotion, and so on. At the same time, the power of appointment, management, and assessment of lower-level officials are granted to the next upper-level government. This is known as the “administrative contract system”.
What changed in China is the development of the market economy. In many specific areas of governance, the Chinese government gradually relaxed its control and granted greater autonomy to local governments and various organizations. For those important fields of the national economy or people’s livelihood, the government still used top-down personnel management and strong incentive design to ensure national unity and social stability [17]. In medicine and health-care, China has also implemented a similar bureaucracy. The dean of a public hospital is fully responsible for the medical practice, teaching, research, and administration of the hospital.
Although the dean is usually a medical expert, the position most resembles that of an administrative official, subject to the selection, appointment, and assessment processes of a civil servant. The dean must manage a hospital while being extremely sensitive to policy directives from the “upward responsibility system”. In addition, the organizational structure and personnel system of a public hospitals is like other government institutions. This quasi-bureaucracy system in public hospital is not only a traditional product of path dependence, but also a feasible path to achieve effective stimulation [18].
In terms of personnel and organizational structure, public hospitals are like bureaucratic organizations. Operationally, there are some differences. The dean’s performance assessment, appointment, and promotion will follow certain formal standards. But these standards differ by region and largely depend on the superior’s evaluation. The hospital must also maintain distinct professional requirements that are like those of professional organizations. Therefore, this paper argues that although public hospitals cannot be treated as strictly bureaucratic organizations, they show obvious characteristics of quasi-bureaucracies.
Logic of Enterprise: Profit-Making Demand after the Government’s Decentralization: China’s reform and opening-up that began in 1978 was in part due to the limited government financial resources and realistic difficulties of managing an enormous, top-down bureaucracy. Governments at all levels gradually delegated their power and gave greater autonomy to governance objects to stimulate the market vigor.
Public hospitals also became economic entities of independent management and professional organizations under the “dean accountability system”. Under the pressure of organization survival and effective operation, public hospitals have more incentive to pursue economic benefits. Government subsidies could not make up for the huge costs they incurred. They had to broaden their funding sources. Public hospitals became like enterprises. They needed to perform the basic functions of medical services, but they also had to think about cost accounting, economic benefit, and increasing the income of doctors, nurses, and the hospital. Although the public welfare requirement did not change, financial pressures incentivized public hospitals to blend some enterprise organizational logic to meet profit demands.
Logic of a Professional Organization: Regulatory Difficulties Caused by Professional Barriers: Every organization has an internal, operations logic based on its own characteristics. In a specialized organization, norms and behavior formed by the specialization process have strong effects that do not easily bend to external restrictions. The institutional logic of the unified system is conducive to unified objectives but is incompatible with the professional logic of organizations. The development of professional organizations needs relative independence to form professional authority. This is hard to integrate into a unified system as it may question authority and cause conflicts between different logics.
In the process of policy assessment, government will also have asymmetric information, information collection difficulties, and other complex governance problems, which are hard to coordinate because of the different interests of organizations. Public hospitals as professional organizations with professional barriers amplify coordination difficulties. The top-down policy signal in China is usually strong and powerful, while the bottom-up feedback is often weak and useless. Governance objects, unable to participate in policy agenda setting, can only blend its “small objective” into the implementation process; it does not always conform to the government’s “big objective”.
Competition between Four Governance Logics: The process of governing a public hospital is the result of interaction between the government’s “big objective” and the hospital’s “small objective”. In different periods, the government has different demands for public hospitals, and public hospitals’ prioritization between public welfare (the “big objective”) and effective operation (the “small objective”) will also be slightly different, resulting in obvious differences in strategic choices, the behavior of the public hospital, and its stakeholders (Table 2).
The dean of each public hospital must actively respond to policy requirements, and perform well for the annual evaluation, win the trust and praise of superior departments, and show the characteristics of “upward responsibility”. However, in daily management, the dean must also acquire support from hospital directors, pharmacists, clinicians, and other internal professional personnel, to reduce internal friction and resistance and to achieve the sustainable development of the hospital. Compared with government officials, a dean will usually have a longer working term. They need to complete policy instructions as well as be concerned with and maintain long-term relationships with internal employees, to get understanding and support from the medical staff.
In addition, the hospital is a professional organization with regulatory barriers. Compared to government officials, deans usually have working experience as doctors or office directors. They are more familiar with the actual difficulties of a hospital, they understand the concerns of medical staff. They are more likely to form long-term strategic alliances. Deans must balance the “big objective” and “small objective”. During policy mobilization or an assessment period, when the external environment is very intense, the “upward responsibility system” may become the priority choice. There may also be temporary frictions between the dean and doctors due to the difficulty of achieving the “big objective”. However, the pressures of the external environment will always lessen. The strategic alliance between the dean and doctors will be rebuilt. Public hospitals will return to their daily operating mechanism, pursuing their “small objective”.
Therefore, the government needs to balance carefully. The government’s absence will cause competition and scarcity of medical services. The government’s intrusion will impair the autonomy and professionalism of doctors and hospitals. The government’s dislocation will lead to complexity and chaos in hospital governance.
| State does everything period(1950s-1970s) | Market dominant period(1980s-1990s) | Government-led period(2000s to date) | |
|---|---|---|---|
| Institutional reform | Regulation and operation unification | Decentralization of power and transfer of profits | Separating management from enforcement |
| Market effect ↓ Government regulation ↑ | Market effect ↑ Government regulation ↓ | Market effect ↑ Government regulation ↑ | |
| Internal governance | Legality mechanism ↑ | Efficiency mechanism ↑ | Legality mechanism vs. Efficiency mechanism |
| State logic & Quasi-bureaucracy logic are dominant | Enterprise logic & Professional organization logic are dominant | Competition between the four governance logics | |
| Priority objective | Public welfare ↑ Big objective ↑ | Effective operation ↑ Small objective ↑ | Public welfare vs. Effective operation Big objective vs. Small objective |
| Governance effect | Low level but wide coverage medical service | Rapid development of medical and pharmaceutical industry | very difficult and expensive to seek medical care |
| Effect of policy window | Real policy window | Real policy window | Illusory policy window |
Table 2: Interaction of the government’s “big objective” with the public hospital’s “small objective”.
It is very difficult to achieve effective governance when the four competing logics coexist in one organization [19]. Governance mechanisms will have different incentive mechanisms and organizational structures. This will cause conflict in the process of policy implementation [20]. Once a governance logic forms an institutionalized mechanism, it will be incompatible with other mechanisms and mutual transformation or alternative between different mechanisms are easy to cause the organization’s internal conflict, thereby increase difficulties, and even lead to instability of the organization (Figure 2).
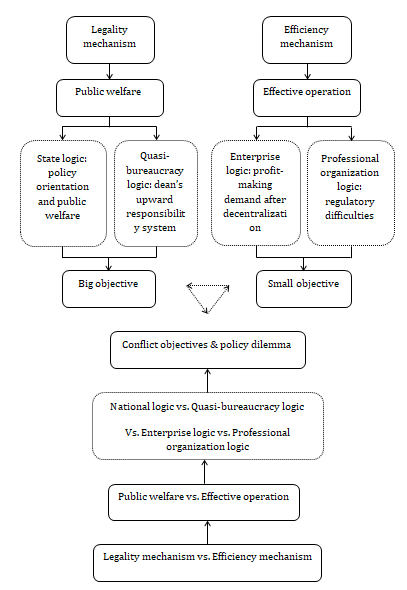
The government’s “big objective” and the governance object’s “small objective” often conflict. When we design incentive mechanisms based on one organization’s goal, the behavior induced by this goal is likely to run up against the logics created by the other organizations’ goals. Therefore, the unified system delivered by political signals, the dean responsibility system decided by the bureaucracy, the public welfare oriented by “upward responsibility system”, the demand of lightening fiscal burden of government, the profit- making pressure surged by decentralization, as well as the professionalism and independence required by professional organization, make the contradiction between public welfare (the “big objective”) and effective operation (the “small objective”) gradually highlighted.
Public hospital governance provides a unique social space for the above four competitive logics. They often conflict but they must interact. If we don’t understand and analyze these competitive governance logics, then we won’t understand the competition between the “big objective” and the “small objective” in the process of Chinese social policy reform. And, instead, we will only see the twists and turns of failing policy reforms.
Conclusion and Discussion
Medical policy relates closely to people’s vital interests. It also reflects competition among various stakeholders’ and the interdependence of government, the market, and society. Most current studies have taken the government as the protagonist of agenda setting but ignored the role of governance objects. This paper extends Kingdon’s Multiple Stream Framework by claiming that in the process of one country’s medical policy reform, there are two very different policy objectives. One is the government’s “big objective”, and the other is the governance object’s “small objective”. The interaction between these two objectives will influence the formation of the policy stream and ultimately influence the opening of policy window. When the “big objective” is compatible with the “small objective”, it opens a “real policy window”. When these two are in conflict, the discretion of the governance object will expand and an “illusory policy window” will open that will delay or even hinder the policy reform.
In this paper, we take the China’s medical and health- care reform as a breakthrough point to elaborate the “big objective-small objective” framework in the social transformation process of a particular country. China’s experience reveals how the “real policy window” and the “illusory policy window” are formed, as well as the centralization and decentralization process. In addition, we took the trickiest governance problem, public hospital reform, to explain the significance of the above framework.
An “illusory policy window” caused by “big objective-small objective” conflict eventually will cause the governance dilemma of wanting “a horse to run but not to eat” that leads to the delay and even blocking of the medical policy reform.
This is because the different objectives of the government and the governance object are determined separately by their own organizational logic. When they conflict with each other, it will slow the policy reform and influence the effect of policy implementation. The complexity and challenge of China’s medical reform is that there are four competitive governance logics coexist in public hospitals, namely, the country’s logic (policy oriented and public welfare demand), the logic of quasi-bureaucracy (dean’s “upward responsibility system”), the logic of enterprise (profit-making requirement after the government’s decentralization strategy), and the logic of professional organization (difficult to regulate ). All of the above must balance between public welfare (“big objective”) and effective operation (“small objective”) or the long-term conflict will continue, thus seriously affecting China’s medical policy reform.
Considering the interactions between government and governance object help us identify the obstacles and difficulties faced by top-down national policies; especially if we adopt a bottom-up perspective. The framework and conclusions of this article may also have some significance for medical policy reform in other countries.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgement
This research was supported by National Natural Science Foundation of China (Grant No. 72104084).
References
-
Heilmann S (2008) Policy Experimentation in China’s Economic Rise. Studies in Comparative International Development 43(1): 1-26.
-
Greenstone M, Rema H (2014) Environmental Regulations, Air and Water Pollution, and Infant Mortality in India. American Economic Review 104(10): 3038-3072.
-
Malesky E, Cuong VN, Anh T (2014) The Impact of Recentralization on Public Services: A Difference-in- Differences Analysis of the Abolition of Elected Councils in Vietnam. American Political Science Review 108(1): 144-168.
-
Mei CQ, Margaret MP (2014) Killing a Chicken to Scare the Monkeys?. Deterrence Failure and Local Defiance in China. The China Journal 72: 75-97.
-
Kingdon JW (1984) Agendas, Alternatives and Public Policies. 2nd (Edn.), New York: Harper Collins.
-
Zhu XF, Zhao H (2018) Experimentalist Governance with Interactive Central-Local Relations: Making New Pension Policies in China. The Policy Studies Journal 49(1): 13-36.
-
Meyer JW, Brian R (1977) Institutionalized Organizations: Formal Structure as Myth and Ceremony. American Journal of Sociology 83(2): 340-363.
-
Tang N, Cheng L, Cai CK (2020) Making collective policy entrepreneurship work: the case of China’s post-disaster reconstruction. Journal of Asian Public Policy 13(1): 60- 78.
-
Hsu RC (1977) The Political Economy of Rural health Care in China. Review of Radical Political Economy 9(1): 134-140.
-
Albrecht GL, Tang XY (1990) Rehabilitation in the People’s Republic of China: A reflection of social structure and culture. Advances in Medical Sociology (1): 235-267.
-
Martin KW, Sun ZX (2010) The Impact of China’s Market Reforms on the Health of Chinese Citizens: Examining Two Puzzles. China: An International Journal 8(1): 1-32.
-
Karen E (2010) Kanbing Nan, Kanbing Gui: China’s Healthcare System Reforms, 1980-2007. In: Jean Oi, Rozelle S, et al. (Eds.), Growing Pains: Tensions and Opportunities in China’s Transition, Washington, DC: Brookings Institution.
-
Tang N, Ding Z, Xu YN (2018) Corruption and Anti- Corruption Research in China: A Critical Review of Chinese Top Journal Publications (1989-2017). Chinese Public Administration Review 9(2): 79-98.
-
Stinchcombe AL (1965) Social Structure and Organizations, In: Handbook of Organizations, In: JG March (Ed.), Chicago, USA, pp: 142-193.
-
Zhou XG, Hong L, Leonard O, Ye YY (2013) A Behavioral Model of Muddling through in the Chinese Bureaucracy. The China Journal 70: 120-147.
-
Weber M (1946) From Max Weber: Essays in Sociology. In: Gerth HH, Wright Mills C (Eds.), New York: Oxford University Press, pp: 490.
-
Schurmann F (1968) Ideology and Organization in Communist China. Berkeley, CA: University of California Press.
-
Miller GJ (1992) Managerial Dilemmas. New York: Cambridge University Press.
-
Williamson OE (1985) The Economic Institutions of Capitalism. New York: Free Press.
-
Baker G, Gibbons R, Murphy K (2001) Bringing the Market inside the Firm?. American Economic Review 91(2): 212-218.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda