Health Care System Decentralization, the Case of Venezuela Historic Evolution, Results, and Consequences of its Institutional Reversal
The author exposes the political, social, and technical foundations that motivate and justify the decentralization of health care services, as a means, not as an end. He highlights the Venezuelan constitutional and legal framework that establishes the foundations of transference and sets competencies. Throughout the article, the author highlights the fundamental role of the decentralization of modern Health Systems, for the equitable and efficient achievement and quality health services and products, with the participation of the communities, as well as the conditions and requirements for its application; the purposes, objectives, benefits, and new challenges derived from its implementation. A historical recount is made on the experience garnered by the decentralization of the health care sector in Venezuela. The process for the construction of the Decentralization and Transfer of Competencies Agreements is briefly described, as well as the scope, limitations, and implementation results in the Venezuelan health care system. Briefly I explain the process of nonapplication of the Constitutional norm, and later reversal of the decentralization in health care which occurred from 2007, and its consequences. Finally, I pose strategic proposals for the defense of decentralization.
Introduction
Decentralization is a process of “redistribution” of powers of the State, in favor of greater autonomy, efficiency, and prominence of the role of the regions (States) and municipalities, and of more direct participation of society in the fulfillment of “public affairs.” It includes the delegation of the power of control to the lower levels of organizations.
Investigation Paper
It implies the distribution of the attributions of centralized power towards the authorities of the regions or local governments, be it State, Region, or Municipality, with a political component [1].
Decentralization constitutes a principle of the Administrative Organization, which lies in the transfer of decision-making powers, from a territorial political entity to another, (or others) different from the territorial public body that transfers them [2].
It is the transfer of powers that provides autonomy for all public services, but that, at the same time, depends on the National State, in such a way that the new autonomous entities cannot attempt against the State [3].
It necessarily includes the community, through citizen participation, in the administration and disposal of the goods and services that the regions possess, which leads to their intervention in decision-making at the State and Municipal level [4].
The decentralization processes that began in many Latin American countries in the 1970s, including Venezuela, were due to the governance crisis among those nations, with the disproportionate growth and accumulation of State power, (Centralism), bureaucratic, with an exhausted and inefficient management model, to deliver goods and services to the communities. The dissatisfaction of the population led to the aforementioned governance crisis, which demanded greater equity and efficiency in the distribution and access to State goods and services. To greater democracy and participation. In response, proposals for reform and modernization of the State were produced, promoted by multilateral organizations, with varied results from country to country [4, 5].
Decentralized governance of health care services means the transfer of authority in planning, management, and decision-making from the national to the subnational level, from higher to lower levels in the governance hierarchy [5].
The purpose of this article is to describe experiences of the decentralization process that occurred in Venezuela, particularly in the Health Care System (HCS).
For the effective application of the decentralization plans, a set of requirements and conditions was required: political will and commitment between the stakeholders. The existence of fundamental rules that would guide the relationship among the stakeholders; the centralizing element is the National Constitution because it is applied throughout the territory, which makes it common to all involved; a law of Decentralization, Delimitation, and Transfer of Competencies. The evaluation of the conditions for the approval of Decentralization and Transfer Agreements. Moreover, conditions of the political, economic, human, technical, and social resources would allow its feasibility [3]. Because it is a complex process, it is progressive, requiring learning by the parties involved. Responsibilities and new challenges are assumed [6]. It is not decreed. It is an Intergovernmental Agreement.
The purposes of the Agreement can be summarized as:
- The achievement of efficiency, to reach the objectives, and access to goods and services with equality.
- Citizen participation.
- Prevention of threats and the promotion of social wellbeing.
- Control of corruption, among others.
- Decentralization is a means, not an end. It is a necessary condition to improve access to, quality, and equality of the services intended to provide care to the population.
The objectives to be achieved were clearly defined:
- Strengthen the Central Organs as normative entities, while delegating to the state and local governments the execution of services and benefits. Namely: Regulatory Centralization and Operational Decentralization.
- Strengthen State and Municipal Bodies in planning, programming, management, and service control capabilities.
- Stimulate and organize human, physical, and financial resources.
- Train executive and administrative staff.
- Provide permanent advice to state governments.
- Act with the greatest transparency.
- Conduct technical and administrative actions, adjusted to rules and procedures specifically designed in the Decentralization Agreement.
- Select human resources, curating by merit and public tenders, thus avoiding corrupt patronage.
Likewise, the socio-political, cultural, technical, economic, and administrative benefits, among others, that were expected after its application was:
- A balanced distribution of power, separating it from the Central Power towards the States and Municipalities.
- With decentralization, administrative and functional autonomy was given to the municipalities.
- That autonomy implied breaking with the predominantly Centralist form of the State.
- Promotion of greater efficiency and importance of the regions (States and Municipalities).
- Empower the regions to make appropriate decisions for their benefit.
- Greater ability to obtain, execute, and control local resources.
- Legitimize regional and local leaders.
- Produce favorable changes in the socio-territorial and political structures in the regions and localities.
The implementation of the agreement would lead to the necessity of addressing new challenges [7], for example:
- Modify the redistribution systems to ensure equality and acknowledge regional differences through an adequate combination of social and territorial distribution systems; the social one ensures equal access to public goods and services, and the territorial one takes advantage of collective contributions and local initiatives.
- With decentralization, the states and municipalities assume relevance in the administration of delivery of public services, attending to the specific needs of the localities.
- The central level of government is forced to strengthen its non-competitive powers of stewardship, coordination, governance, control, supervision, and auditing.
- Perform the evaluation, prior diagnosis, monitoring, control, and fulfillment of requirements, of the skills to be transferred, the administrative regulations, and the coordination of services.
The new Constitution establishes that Venezuela is a “Decentralized Federal State,” which implies that its form of organization as a State must inherently include certain elements of a Federal State; one of these elements is decentralization [10].
Decentralization, as it pertains to the form of a State, should bring with it the redistribution and political-territorial reorganization of the powers and decision-making, assigned to the Central Power by the Constitution, towards other political-administrative entities.
In the Statement of Motives, it states: “... are characteristic of the cooperative federal model, in which the authorities and communities of the different territorial political levels participate in the formation of public policies common to the Nation, integrating themselves in a sphere of shared government for the exercise of the competencies in which they concur.” And, in the Preamble, “… with the supreme purpose of re- founding the Republic to establish a democratic, participative, and leading, multiethnic and multicultural society in a federal and decentralized State of justice, that consolidates the values of freedom, independence, peace, solidarity, the common
Constitutional Framework for Decentralization
Although the decentralization processes in Venezuela began in 1989, with the Organic Law of Decentralization, Delimitation, and Transfer of Public Powers (LOD) [8], 10 years later, with the approval of the Constitution of 1999 [9], it was hoped that it would be possible to advance and consolidate the decentralization process; regrettably, this was not the case (Figure 1).
good, territorial integrity, coexistence, and the rule of law for this and future generations...”; here, the existence of the federal and decentralized State is recognized, incorporating society in the functioning of the State to achieve those ends.
In Article 2, a “democratic, social, and legal” State is proposed, for which the Public Power must be decentralized, and then goes on:
In Article 4, “The Bolivarian Republic of Venezuela is a decentralized Federal State in the terms enshrined in this Constitution, and is governed by the principles of territorial integrity, cooperation, solidarity, concurrence, and co- responsibility.” Article 6, “the government is and will always be…. Decentralized;” conceiving decentralization as an essential policy that entails the deepening of democracy and the effectiveness and efficiency of the State, for which it includes political entities in this content, as an integral part of its structure.
To develop this policy, public systems were foreseen: fiscal, judicial, education, health, among other areas; that would guarantee the administrative decentralization of government entities.
Article 157 has an essentially decentralizing content since it states that the Legislative Power, represented in the National Assembly, by majority decision, will attribute to the Municipalities or the States powers that correspond to the National Power, and adds “…to promote decentralization.” Article 158 attributes decentralization as a national public policy and states, among other things, that “... democracy should be deepened, bringing power closer to the population...”, with the idea that the purposes of the State are effective and efficient in their achievement. In Article 185, the Federal Council of Government is defined as: “…body in charge of planning and coordinating policies and actions for the development of the process of decentralization and transfer of powers from the National Power to the States and Municipalities…” “...The Inter-territorial Compensation Fund will depend on the Federal Council of Government, destined to finance public investments aimed at promoting the balanced development of the regions, cooperation and complementation of the development policies and initiatives of the different public entities…” This Body, based on regional imbalances, would annually discuss and approve the resources that would be allocated to the Inter-territorial Compensation Fund and the priority investment areas to which said resources will be applied.
The Federal Power would have Constitutional Guarantees to know [11].
- Federation and decentralization are irreversible characteristics of the Republic and the State.
- The National Power cannot modify the structure of federal power.
- Decentralization must be fiscally sustainable and protect territorial balances.
- Decentralization is progressive and agreed upon by the parties.
- Decentralization is flexible and adaptable to territorial diversity. To guarantee financial security, the Constitution provided for:
- The application of principles of Autonomy and Financial Balance of states and municipalities: Subsidiarity, Inter- territorial Equity, and Coordination.
- The development of state and municipal finances, taxes, fees.
- The creation of the Inter-territorial Compensation Fund, attached to the Federal Council of Government.
Legal Framework of Decentralization
On December 28, 1989, the Organic Law of Decentralization, Delimitation, and Transfer of Powers of Public Power (LOD) was approved [8]. I highlight its content:
- Article 4 established ¨The services will be transferred progressively¨.
- Article 7 defined the procedures to approve transfer and decentralization agreements: When the initiative comes from the National Executive, a proposal is presented to the Senate of the Republic, which will agree or deny the transfer and its modality. If the initiative comes from the State Government, the request is made via the State Legislative Assembly to the National Executive and this to the Senate, which decides.
- And Article 8: Any of the transferred services can be reversed, through a request from the National Executive addressed to the Senate or from the Government, where the incompetence of the region to efficiently comply with the contracted commitment is exposed.
- The projects of Agreements of Decentralization and Transfer of Competencies were carefully analyzed by a High-Level Commission, in particular: Diagnosis of the characteristics of the skills to be transferred.
- An Operational Evaluation, dynamic procedure, during the co-management regime (one year), before the definitive assignment of the transfers.
- The Temporary Assignment (two years), with the annual evaluation of health indicators, and in completed activities. Accountability, evaluation of management capacity, and satisfaction with the quality of services provided.
- The Reversal of the transfer was contemplated in case of breach of commitments.
- The transfer approval process included:
- Evaluation by the High-level Commission for analysis and evaluation of decentralization proposals made up of the Ministry of Health and Social Assistance (MSAS), the Ministry of Internal Affairs, and the State Government.
- Analysis by OCEPRE. (Central Budget Office), OCP (Central Personnel Office), and Ministry of Finance.
- Evaluation of the project and opinion by the National Attorney of the Republic and “Cordiplan” (Ministry of Planning).
- Evaluation and Opinion by the Senate of the Republic of the Republic that finally approved or denied the Co- administration Agreement or the Transfer Agreement.
A summary of Decentralization in Health Care in Venezuela
First Stage (1989-1999)
We can identify the first stage before the approval of the new Constitution, whose antecedents are located in 1984, after the study of the Governing Commission of the Health System. The result was the approval of the Organic Law of the National Health System LONS on June 23, 1987. Articles
10 and 29 establish the decentralization of the Organization of Regional Health Services [12]. ¨The MSAS (Ministry of Health and Social Welfare) will progressively attribute to the regions or federal entities the administrative functions of the health subsystems¨...¨The regional bodies of the National Health System will adjust to the principles of regionalization with technical-regulatory centralization and administrative decentralization¨. The Central Body (MSAS) retained the power to order actions through rules and procedures and left the States and Municipalities free to act in a manner agreed upon by both. It was an intergovernmental system. Activities and operations were decentralized and the management and control of Programs were reserved.
After the approval of the Organic Law of Decentralization, Delimitation, and Transfer of Powers of Public Power (LOD), the effective period of decentralization in the HCS in Venezuela begins Figure 1. The first Co-management and Co-administration Agreements were approved in the second half of 1992 [13]. Until the end of 1998, 17 states were decentralized; 88% of the country’s population lived in them, inhabitants who could receive the benefit of decentralization.
Two states were in the process of being studied and 5 had not been decentralized [14] (Figure 2).
On November 11, 1998, the new Organic Health Law [15] (Still in force) was approved, which included provisions related to decentralization in its Articles: 4.9,15, and 17. Simultaneously with the decentralization of the HCS in the States, from 1994 to 1999, in addition, the MSAS Program of Municipalities towards Health was carried out with the support of the Pan American Health Organization [16]. Whose purposes sought: offer the Mayors, tools for the design and management of projects that allow the participation of the community, promote the Proposals of Co-management Agreements between the Regional Power (State) and the Municipal Power, create the State Networks of Healthy Municipalities. The first 64 experiences of the Healthy Municipalities Agreements were applied in 19% of the country’s Municipalities, in 18 states, (some of them that had not been decentralized at the state level); 256 projects were produced with the participation of the communities [17] (Figure 2).
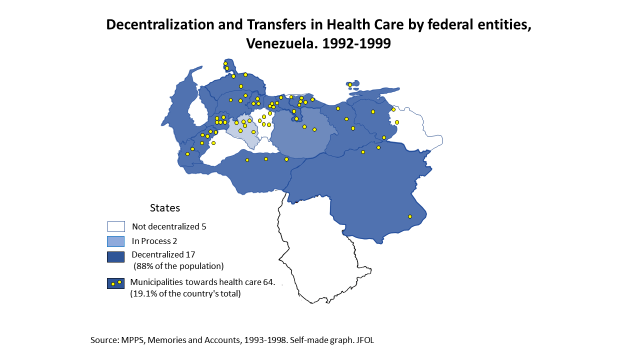
This experience of municipal decentralization and community participation was carried out with great passion and commitment, efficiency, little bureaucracy, and a very low budget. It was very frustrating that this valuable experience was discontinued and discarded as of February 1999, by the administration of the first Chávez government.
The evaluation of the results of the first stage of decentralization in health, from 1989 to 1999, has been published by various authors [18, 19, 20, 21]. Failures were identified in the allocation of budgetary resources to the decentralized states, in the scope of goals, and in Response Capacity. Indicators of performance and quality of the health system, for example, Maternal and Child Care, were favorable in the decentralized states, as well as the coverage of Immunizations, prenatal controls, infant deaths, and maternal deaths.
Efficiency in Performance in the period (2003-2004) showed regular budget execution goals, fully met in the Decentralized States and only 87.53% in non-decentralized States [22]. It was also higher in decentralized states Evaluation of Performance Monitoring Systems and Evaluation of Service Management and Quality.
The data processed by Professor Jorge Diaz Polanco, et al. [23] to evaluate Efficiency in Health Expenditure, before 1989, during decentralization until 1998 and after 1999, taking as reference the change in the Infant Mortality Rate and the Maternal Mortality Rate, and their respective Average Annual Reduction Rates (AARR), before decentralization, in the effective period of decentralization and after this period, showed that the indicators were more favorable during the effective period of decentralization (Figures 3-5). Likewise, the Health Expenditure Effectiveness Index, as a percentage volume of GDP, concerning the Infant Mortality Rate, increased during the effective period of decentralization and subsequently decreased, despite the increase in Health Expenditure Figure 6.
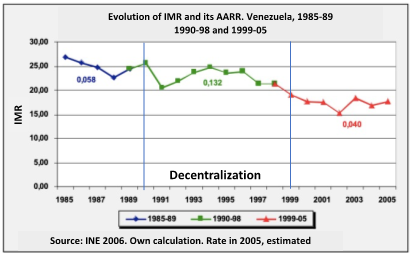
IMR: Infant Mortality Rate. AARR: Average Annual Reduction Rate Figure 3: Evaluation of results of decentralization infant mortality.
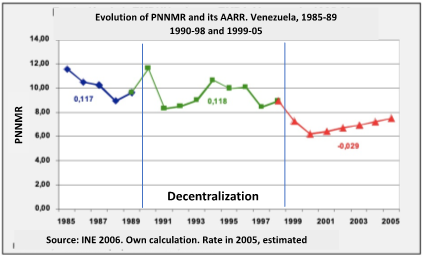
Source: Diaz Polanco, Jorge 2008. PNNMR: Post Neo Natal Mortality Rate Figure 4: Evaluation of results of decentralization infant mortality.
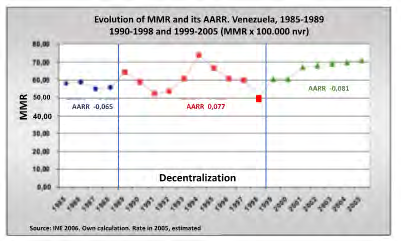
MMR: Maternal Mortality Rate AARR: Annual Average Rate Source: Diaz Polanco, Jorge 2008 Figure 5: Evaluation of results of decentralization maternal mortality.
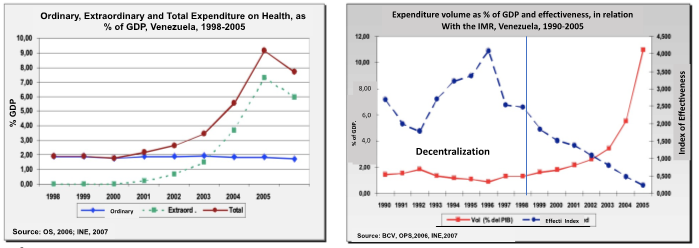
Source: Index of effectiveness of health expenditure: expenditure/infant mortality rate by the square root of the average rate of reduction (change) or annual AAR of the considered period. Spending as GOP or gross domestic product. IE=(PIB/TM) ×√ AARR. Figure 6: Efficiency of health expenditure before, during and after decentralization.
Second Stage (1999-2006)
After the approval of the 1999 Constitution, the first Chávez government advanced in the approval of a set of laws related to decentralization: Laws of the National Planning System and within it, the Public Policy Planning and Coordination Councils (CEPLACOP) and the Local Public Planning Councils (CLPP) 2006. Likewise, the creation of Communal Councils, to make the constitutional provisions effective. Also, the Organic Law of the Municipal Public Power and the Law of the Special Regime of the Metropolitan District.
Additionally, the National Assembly approved the State Public Treasury Law and the Federal Council of Government Law, as the most relevant constitutional body within the planning system and decentralization policies [20]. Both laws were vetoed by the National Executive, and returned to the Assembly. This body decided not to discuss them again, eliminating the possibility of their entry into force. The LOD was reformed in 2003, modifying articles 14 and 15 of the Organic Law of Decentralization, Delimitation, and Transfer of Powers of Public Power (LOD) of 1989. To progressively increase the Municipal situation up to 20% and a direct transfer mechanism from the Central Power to the Municipalities was introduced.
Serious contradictions between the various government forces prevented the approval of the New Organic Health Law, which should have been sanctioned in 2004, to develop the constitutional mandates in health, contained in Constitutional Article 83: “The State will create, exercise leadership and manage a national public health system, among multiple sectors, decentralized, and participatory, integrated into the social security system, governed by the principles of free, universality, comprehensiveness, equity, social integration, and solidarity” [9]. Between 1999 and 2006, no new Health Decentralization Agreement projects were evaluated or approved.
Third Stage (2006 onwards), Reversion to the Centralized and Authoritarian System
After the presidential elections in December 2006, the National Government began an accelerated process of re- centralization of all sectors and progress towards an autocratic model of society, contrary to the National Constitution, which is summarized in the concept of “revolutionary protagonist democracy”, established in the Simón Bolívar Project and converted into the “Plan de la Nación 2007-2013,” as the “First Socialist Plan” and its successive versions up to the present time. This plan was approved by the National Assembly in 2007 before submitting to a referendum the Constitutional Reform Proposal introduced by the President of the Republic, to create a new “socialist social order” in the country and is applied from that date as a “framework law” to create this new order outside the Constitution. Laws that continue to be applied, although the constitutional reform was denied in the Constitutional Referendum of December 2007.
However, with the Socialist Plan, the idea of “participatory democracy”, contained in the Constitution, was abandoned, understood as the extension of the direct participation of citizens in public affairs, within a federal and decentralized State structure.
It was adopted authoritatively and is still trying to impose the: “revolutionary democracy.” The expression of “true democracy” in which all the original power of the individual is handed over to the community and a “general will” is produced, not representative but moral and collectively sustained, which forces the associates to conduct themselves for justice, equality and freedom of the collective body politic. “The State guarantees the well-being of all above equality before the law and mercantile despotism [24].
Subsequently, the National Assembly approved an Enabling Law for President Chávez and he promulgated 66 decree-laws in 18 months (from 1-2-2007 to 7-31-2008), to promote rapid changes in the legal system to build the foundations of a “socialist society.” With these decrees, government functions were centralized in a Central Planning Commission, an open letter was given to a process of functional and territorial dispersion, to directly serve the communities through national public programs and services, and legal authorization was given to the Executive to create a new territorial delimitation with regional authorities appointed by the President and declare territories, goods, and services of “public utility”. All contrary to the new National Constitution.
Within the same guidelines of the Socialist Plan, between February and March 2010, the National Assembly approved the Law and Regulations of the Federal Council of Government, in which a new concept of Federalism was adopted, defined as the political organization that it aims to build a socialist society, against the attempts of “national and international oligarchies” to monopolize economic and political power.
With this Law, the Constitutional order was altered, by ignoring the Federal and decentralized structure of the Venezuelan State and all decentralization process within that structure was canceled. (4.11,19.20). In open disregard of the Constitution, the states and municipalities ceased to be the entities to which powers of the National Power are decentralized and transferred. On the contrary, it is these entities that must decentralize theirs to the “base organizations of People’s Power” (non-existent in the Constitution), of a socialist nature, by decision of the autocrat and aligned with the centralized planning regime. In addition to this, the law attributes to the President of the Republic himself the power to create new territorial units under the management of national authorities, called Motor Districts, which are governed by a system of communes in which property passes into the hands of the State.
On April 24, 2007, Chavez publicly declared: “The decentralization of the Health System is over… this decentralization is the cause of the disaster in which public health finds itself” [25]. Therefore, its re-centralization was imposed. To this declaration, the former Ministers of Health and other personalities, responded by a Public Letter. On the Recentralization of Health. Public opinion and the President of the Republic. 04-25-2007 [26]. It was never answered. A few months later, on January 28, 2008, through Decree 5,836, Chavez ordered the creation of the Metropolitan Health System and the Transfer of hospitals and health establishments in the Metropolitan Area of Caracas, attached to the Mayor’s Office of the Metropolitan District, to the MPPS. With which he centralized again the health services of a large part of the Metropolitan Area of Caracas. Later, through another Decree 6,543 of December 2, 2008, it transferred to the Ministry of People’s Power to Health establishments and mobile medical care units, attached to the Government of the Bolivarian State of Miranda and repealed the Transfer Agreement to the State of Miranda for Health Services
provided by the Ministry of Health and Social Assistance and by attached Organizations, dated 10/25/1995 [27].
Other LOD modifications were made. Posted in Official Gazette No. 39,140 the Partial Reform thereof, on March 17, 2009; provided in article 8, that the National Executive was empowered to reverse, for strategic reasons, merit, opportunity, and convenience, the transfer of powers granted to the states over goods or services considered of general public interest [24].
Subsequently, Heads of Government, State Protectors, Single Health Authorities were appointed, who usurped the functions and powers of the officials elected or legitimately appointed in the Federal entities governed by the political forces of the Opposition.
Consequences of Reversal of Transfers and Recentralization of Health
The decisions of the Executive Power put into practice through presidential decrees, violated the Constitution, concentrated the decisions in the Central Power, undermined the powers of State and Municipal governments [7, 10, 11, 24] and advanced in ways contrary to modern health systems, based on high participation of organized communities, in the Primary Health Care strategy.
We again warned and publicly denounced the consequences of these decisions: ¨Venezuelans have the right to discuss and choose our health system since it is a complex decision, which requires a general agreement, which involves building a new ¨Social Health Contract¨, so it cannot be the result of a hasty decision without consultation, protected by a decree, but by the constitutional principles that guarantee the right to health¨ [28].
Consequences in the political sphere: Such measures had regressive implications for public good guarantees, such as State obligations strengthened through decentralization [24].
They raised the intervention of the National Government in attributions and competencies that belong to the states and municipalities by constitutional mandate.
They regressed towards a model of the centralized organization of the State, which was largely superseded in the 1999 Constitution, in addition to imposing “intervention” and “reversal” measures not contemplated in the Constitution.
They took away from the states and municipalities the means to exercise their powers and competencies. [29]. They affected the fundamental citizen rights, from the very moment that the 1999 Constitution assumed the figure of concurrent powers, in which states and municipalities share responsibilities in all those matters that guarantee a decent life for all its citizens, specifically in timely access to health services, justice and the exercise of the vote.
Regarding the freedoms and citizen rights, the measures to revert powers and recentralize health produced serious consequences both for the democratic political system and for the Human Rights of the Venezuelan population, including the right to health, which is translated into:
- Threats to the fundamental freedoms of citizens through authoritarian practices.
- Social inclusion is limited by the abandonment of public policies.
- The adoption of welfare measures allows greater political control over the population.
- The loss of the right to participation and the means to exercise it, by establishing restrictions on the autonomy of citizens and their organizations.
- Criminalize those who question or do not share the government’s policies and close the instances of participation to those who do not adhere to the socialist ideology.
Specifically, on the Health System, it has been condemned, since then, to a condition of progressive deterioration and extreme precariousness, which makes it unfair, inequitable, inefficient, fragmented, and incapable of satisfying the basic health needs and demands of the population.
The application of legal instruments and decrees contrary to and in violation of the Constitution has had a negative influence on the normative principles of the right to health in Venezuela, namely: universality, equity, promotion and participation, and consequently, the dignified life of the population in a democracy, by affecting the organization of the health system, now centralized, authoritarian and exclusive. Such circumstances make it incapable of responding to the complex and ongoing humanitarian crisis that has affected the country in the last 6 years and efficiently preparing for new threats to collective health [30]; with responsiveness to an epidemic. Venezuela, in 2019, ranked last out of 33 countries in Latin America and the Caribbean and ranked 176th out of a total of 195 countries according to the Global Health Security Index, prepared by a panel of international experts [31]. That was the situation of the health system before the emergency of the COVID-19 pandemic, as of March 2020. What strategic proposals can be developed in a situation of this nature? With an outlaw regime that does not respect the Constitution and democratic norms, which has fraudulently implemented a Communal State, rejected in the Constitutional Referendu [32]. Will decentralization survive “Chavismo-Madurismo”? The actions of municipal weakening and the creation of communal councils only recognized by ideological coincidences, which have been experienced in Venezuela, represent the denial of values and the collapse of the democratic system [33].
In the search to optimize public policies, including the HCS in Venezuela, a set of optimistic proposals stand out, aimed at restoring constitutional mandates, ordering and respecting the powers of the various government levels, and guaranteeing the participation of organized citizens [11].
- That the State and Municipal Governments fully assume the powers and competencies emanating from the Constitution, making the rights of the people prevail above all. Promoting and building an agenda for the development and rescue of Decentralization.
- That political and social agreement be promoted in terms of decentralization linked to the development of exclusive and concurrent powers.
- Promote, extend and deepen the associative links between different sectors of civil society, states, and municipalities of the country, to unite efforts of citizen calls to build alliances and networks to mobilize support.
- Expand the channels of communication and free dissemination of information to citizens, through new strategies and tools.
- Strengthen response capacities in situations of restriction or threat to civil rights and democratic guarantees, recovering public spaces and the civic sense of politics.
In 2014, we proposed the restitution and promotion of the decentralization process in Health Care. To revert re-centralization of Health Care System (HCS) executed by decrees that infringed the Constitution of 2008. To perfect the processes of transference of goods, services, and competencies of the health care services to the states and, in turn, from the states to the municipalities and communities. To set the decentralization process in order, correcting the mistakes and deficiencies of the past, strengthening the governance functions of the National Government in health care, which are substantial and non-delegable, by “regulatory centralization,” and in turn to apply and set in order the “operational and management decentralization” of health services toward other government entities and the communities. To increase the monitoring, comptrollership, and evaluation mechanisms for processes and results, as well as to stimulate the evaluation process for user satisfaction [34].
Conclusion
The progress made during the Health Care Services decentralization that was effectively carried out in Venezuela between 1989 and 1999, which made it possible to start coverage and care for 89% of the country’s population, through the application of intergovernmental agreements and the more efficient use of public resources, suffered a notorious setback and paralysis, to the detriment of the health care rights of Venezuelans, from 2007, with the presidential decision to re-centralize health services by decree. This decision was executed without any prior evaluation of the results of the decentralized management of population health statistics.
Some numbers showed that the decentralized management was more efficient in the use of resources, and overall improvement in health and spending efficiency statistics (Infant Mortality Rate, Maternal Mortality Rate and AARR) were observed during the period of decentralization, when compared with the period before and after the interruption of the constitutional norm, and the recentralization of health care service delivery.
This highlights the discursive contradiction of the government regarding the promotion of citizen participation and protagonism, arranged in the Constitution of 1999 and several other laws, and the contrary actions later applied in the area of health care, which distanced the decision-making and free participation of the communities, and it can be inferred that part of the current low quality and response capacity of the Venezuelan health system is associated with the recentralization process.
References
-
Orjuela LJ (1993) Decentralization and Governance in Colombia. Editorial Elizabeth Ungar. Department of Political Science. The University of the Andes. Colombia.
-
Frallicciardi BE (2012) Organization Theory and Public Administration. Legal Chair. Buenos Aires.
-
Lopez VM (2001) Potential of the Municipality for the local development of Venezuela. Venezuelan Management Magazine 6(15): 446.
-
Mills A, Vaughan JP, Smith DL, Tabibzadeh I (1990) Decentralization of health systems: concepts, aspects and national experiences edited by Anne Mills ... [et al.]. World Health Organization.
-
Robalino DA, Picazo OF, Voetberg A (2001) Does fiscal decentralization improve health outcomes? Evidence from a cross-country analysis. Policy Research Working Paper 2565. Washington.
-
Vargas Hernández JG (2007) Political and Administrative Decentralization as a Governance Mechanism. Technological Institute of Ciudad Guzmán. Jalisco Mexico.
-
García MP (1991) Ambiente, Estado y Sociedad. Crisis, Estado y Sociedad Civil: Conflictos Socio-Ambientales. Universidad Simón Bolívar. Centro de Estudios del Desarrollo (CENDES).
-
(1989) National Congress Republic of Venezuela Law of Decentralization and Delimitation and Transfer of Competencies. Official Gazette of the Republic of Venezuela, Venezuela 4153 of 12-28-1989.
-
(1999) Constitution of the Bolivarian Republic of Venezuela. Extraordinary Official Gazette N° 36,860.
-
Brewer Carías A (2001) Political Decentralization in the 1999 Constitution: Federalism and Municipalism
-
D´Elia Y (2010) In defense of decentralization in Venezuela, ILDIS. pp: 1-14.
-
Montbrun F (1997) Strategies for a health system. Incorporation Work. National Academy of Medicine, Caracas, Venezuela. 1995. Press Solutions Printing, Miami Fla, USA.
-
Pablo Pulido M (1993) Special Annexes to the Memory and Account. pp: 86.
-
MSAS Report (1998) January 1999 Minister José Félix Oletta, L. Exhibition. 4: 602.
-
Organic Law of the National Health System (1987). Official Gazette 33: 745
-
Stangl JM, Darriba T (1999) Municipalities towards health: the Venezuelan experience: a silent revolution / Cities towards health project: the Venezuelan experience: one silent revolution Caracas; Pan American Health Organization pp: 184.
-
Oletta López JF, Stangl JM, Darriba T (1999) Municipalities towards Health. Where are we going? On: Municipalities towards health: the Venezuelan experience: a silent revolution. 2: 73-83.
-
González M (2001) Reforms of the health system in Venezuela (1987-1999): balance and perspectives. ECLAC, Financing for Development Series. pp: 1-46.
-
Jorge Diaz Polanco (2001) The Health Reform in Venezuela. Business Foundation Polar. CENDES - CIID- MSDS-Corpo Salud, Venezuela.
-
Mascareno C (2010) Decentralization and Democracy in Latin America. CENDES, UCV.
-
Human Rights Program for Venezuela PROVEA (2000) Annual Report 1999-2000 United Nations Human Rights Commission. pp: 1-265.
-
Program for Human Rights in Venezuela (2003-2004) Right to health. pp: 1-38.
-
Díaz Polanco J, Cendes UCV (2008) Personal communication.
-
Mata Sandoval M (2015) Doctoral Thesis. Decentralization in Venezuela by mandate of the 1999 Constitution and the centralizing tendency of the Government. The National University of Distance Education. Law School. Department of Political Law. Madrid, Spain, pp: 1-137.
-
(2007) Chávez announces centralization of the Health Sector in Venezuela.
-
Venezuelan Medical Federation (2008) Central Presentation. Diagnosis of the Health Sector in Venezuela. Study of Emerging and Re-Emerging Diseases. Chapter on Decentralization. Punto Fijo, Falcon State, USA, pp: 41-50.
-
Bolivarian Republic of Venezuela (2008) Decree 6,543, Transfer to the Ministry of Popular Power for Health establishments and mobile medical care units, attached to the Government of the Bolivarian State of Miranda and repeal of the Transfer Agreement to the State of Miranda for Health Services provided by the Ministry of Health and Social Assistance and by attached Bodies.
-
Oletta López JF, Walter Valecillos C, Orihuela AR, Pulido P, Bruni Celli B, et al. (2008) Recentralization of the health system, ill-advised and unconstitutional. pp: 1-5.
-
Melean Jorge S (2002) Past Present and Future of Decentralization in Venezuela. Province Magazine. pp: 9.
-
Venezuelan Alliance for Health (2018) Statement. Complex emergency and exercise of the rights to life, health, and nutrition in Venezuela.
-
Global Health Security Index (2019) 2019 GHS Index Country Profile for Venezuela.
-
Brewer Carías A (2015) The Ruin of Democracy. Fifth part: The contempt for the Constitution with the creation of the Communal State. Political Studies Collection, No. 12 Editorial Jurídica Venezolana Caracas/2015 pp: 187- 226.
-
Rangel Guerrero CH (2010) Municipalities, communal councils, and democracy in Venezuela. Historical Processes. University of the Andes Merida, Venezuela, pp: 70-92.
-
Oletta López JF, Walter Valecillos C, Orihuela AR (2014) Ideas To Rebuild A Health Care System Based On Social Development And Protection, to Combat Poverty and Exclusion In Health Care pp: 13-41.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda