The Impact of Pneumococcal Vaccination on SARS-CoV-2 Infection in Health Care Workers Vaccinated Against Influenza in the 2021- 2022 Vaccination Campaign
Introduction: Widespread administration of vaccines should be considered the best preventive strategy in Public Health. Influenza, pneumococcal disease, and Sars-CoV-2 are major public health problems. The last influenza vaccine season, as well as the previous one, took place in the midst of a pandemic. This led to the need to evaluate the possible relationship between influenza and pneumococcal vaccines in the susceptibility and severity of COVID-19 disease. Secondary bacterial infections (SBI) contribute to a significant proportion of influenza-related mortality, with Streptococcus pneumoniae as the main co-infecting pathogen. Vaccines against bacterial pathogens can reduce the incidence and severity of co-infections. The Influenza Vaccination Campaign runs annually for four months, from October 1 to January 31 of the following year; for the Pneumococcal Program, it is recommended to use the influenza vaccination campaign as an opportunity to immunize against pneumococcus as well. Aim of the study: The study aims to compare the trend of COVID infections - during the period from November 1, 2021 to May 31, 2022 - among health care workers who received regular flu vaccination, and to assess, whether among those who also received pneumococcal vaccination during their lifetime, they were better protected against SARS-CoV-2. Materials and Methods: The scenario was defined through extrapolation of data recorded in the Lazio Region's Regional Vaccine Registry (AVR). The sample of 964 individuals consisted of healthcare workers who underwent influenza vaccination during the last Vaccine Campaign (October 2021-January 2022 period) in the ASL of Viterbo. We explored the relationship between pneumococcal vaccination and COVID-19 test positivity. Within the identified cohort, the number of pneumococcal vaccinations administered over a lifetime and the swab positivity for Sars-CoV-2 was noted. The following data were considered: • Number of HCP who underwent influenza vaccination during the last vaccination campaign; • Number of HCP who underwent influenza vaccination who also received pneumococcal vaccination during their lifetime; • Number of HCP who underwent influenza vaccination and contracted SARS-CoV-2 during the period from November 1, 2021 to May 31, 2022; • Number of HCP who received influenza vaccination and also received pneumococcal vaccination during their lifetime and were infected with SARS-CoV-2 during the period from November 1, 2021 to May 31, 2022. Results: Analysis of the data collected shows that 65.5% of the healthcare workers in our sample, all of whom were vaccinated against influenza during the last Vaccination Campaign, did not contract Sars-CoV-2 infection during the observation period (November 1, 2021-May 31, 2022). Among the 172 HCP who had also undergone pneumococcal vaccination during their lifetime, only 10.4% contracted SarsCoV-2 infection, compared with 39.7% infections found among those who had undergone only influenza vaccination. Conclusion: Pneumococcal vaccinations were found to be associated with a lower likelihood of SARS-CoV-2 infection in healthcare workers vaccinated against influenza in the last CVA. For the upcoming fall-winter season, it will be important to develop a strengthened vaccination strategy, achieving higher vaccination coverages in those at risk. It is also necessary to implement information, education and awareness campaigns for health care workers and the general public.
Introduction
Widespread administration of vaccines should be considered the best preventive strategy in Public Health, as demonstrated in the case of influenza, pneumococcal disease, shingles, meningococcal disease, pertussis, diphtheria [1] and, most recently, SARS-CoV-2 infection. The frail, the elderly and the particularly exposed, including health care workers, must be protected as a priority through vaccination [2].
Influenza, Pneumococcus and Sars-CoV-2 are major Public Health issues and a source of costs in terms of work and school absences, general practitioner consultations and hospital admissions due to possible implications [2].
Seasonal influenza is a major cause of morbidity, mortality and access to healthcare services globally [3]. In accordance with the World Health Organization (WHO), up to 650,000 deaths are associated with seasonal influenza respiratory infections annually [4].
HCP are at increased risk for influenza infection, and have been often identified as sources of infection for vulnerable patients [5].
The rationale for immunizing HCPs against influenza relies on the need to protect them, especially those with co-morbidities, their patients, and to provide healthcare services particularly at a time of high demand [4].
The last flu vaccine season, as well as the previous one, was unique in that it took place in the midst of a pandemic. This led to the need to evaluate the possible relationship between the influenza and pneumococcal vaccines in the susceptibility and severity of COVID-19 disease [6].
Influenza vaccination prevents influenza-related diseases and thus reduced the burden on National Health Systems during the COVID-19 pandemic [7], even if it remains a serious Public Health problem, since seasonal epidemics affect approximately 5-10% of the population [8].
Most people with influenza recover within a week without complications; however, in some cases, serious complications up to death can occur in the high-risk population [9].
The Lazio region’s recommendations for the Influenza Vaccination Campaign indicate the need to offer vaccination to all individuals in the target groups, among which health care workers, adults aged ≥60 years and pregnant women are identified with the highest priority. Given the likely co-circulation of influenza and SARS-CoV-2 viruses in the coming autumn-winter season, it is necessary to reaffirm the importance of influenza vaccination to simplify diagnosis and management of suspected cases, given the similar symptoms between SARS-CoV-2 and Influenza [10].
The vaccines available in the Lazio Region in the last CVA for the health care population were Flucelvax Tetra® and Fluad Tetra® [10].
Synergistic interactions between respiratory viruses and Streptococcus pneumoniae have been extensively investigated [11].
In the COVID-19 pandemic, Pneumococcus is the most common coinfecting pathogen. The weakening of immune function caused by COVID-19 remains a high-risk factor for pneumococcal disease, which has similar symptoms and risk factors with COVID-19. COVID-19 is now considered a primary risk factor for pneumococcal pneumonia and invasive pneumococcal disease. Thus, pneumococcal vaccination during the COVID-19 pandemic has become more critical than ever [12].
Secondary Bacterial Infections (SBIs) contribute to a significant proportion of influenza-related mortality, with Streptococcus pneumoniae as major coinfecting pathogen. Vaccines against bacterial pathogens can reduce coinfection incidence and severity [13].
Streptococcus pneumoniae, with its more than 90 serotypes - with different epidemiological characteristics and pathogenicity - is a pathogen of considerable importance to Public Health because it causes morbidity and mortality on the world population. Some categories of the population are particularly vulnerable to infection [14].
The pneumococcal vaccine used in the Lazio Region during the last Vaccination Program for the health care population was Prevenar 13 [15].
Starting in late 2019, the world was faced with SARS- CoV-2, the etiological agent of coronavirus disease 2019 (COVID-19) [3, 16]. The pandemic was declared on March 11, 2020 [16]. In this context, shortages of health personnel have been found, with HCPs, especially those in the frontline, disproportionately affected [17], and high rates of absences from work were recorded [18].
The Coronavirus Disease 19 (COVID-19) outbreak continues to be a burdensome, multifaceted Public Health concern, and as of 26 September 2022, the number of confirmed worldwide cases has risen to 611.671.073. It has also been responsible for 6.517.805 deaths. At this date a total of 12.640.866.343 vaccine doses have been administered [13, 19]. In Italy, at the same date, there were 22,241,369 confirmed cases of Covid-19, with 176,775 deaths [19].
The COVID emergency has been of great impact for Health Systems: among the various causes mainly for the rapidity of spread and the lack of intervention plans of immediate implementation [20].
A recent study of more than 30,000 people found that those who had been vaccinated against influenza were nearly 90% less likely to develop severe coronavirus disease in the following months than those who had not been vaccinated [21]. The study, conducted prior to the introduction of COVID-19 vaccines, confirms that boosting immune defenses with flu vaccines could help the body reject the SARS-CoV-2 [22].
These considerations have led to the hypothesis that influenza and pneumococcal vaccinations could stimulate an immune response and potentially lower the risk and the severity of other infections, including COVID-19 [12].
In Italy, data on incidence over time of influenza vaccine coverage show a clear peak in the 2020-2021 Campaign, clearly correlating with the advent of the Covid-19 pandemic. The incidence, in the 2021-2022 Campaign, is still at higher levels than in the past two decades, although down from the 2020-2021 Campaign [23].
In the Lazio Region, data on the incidence of influenza vaccine coverage over time are almost overlapping with national data, with the peak at the 2020-2021 Campaign even more pronounced than at the national level [23].
For HCP, influenza vaccination is recommended and offered free of charge. These individuals can be vaccinated by GPs or by the Vaccination Centers of the Local Health Authorities.
Influenza vaccination of HCPs is effective in reducing the incidence of the disease and related absences from work among them, saving financial resources and preventing mortality among patients [24].
The Influenza Vaccination Campaign runs annually for four months, from October 1 until January 31 of the following year; for the Pneumococcal Program it is recommended that the flu vaccination campaign should be used as an opportunity to immunize against pneumococcus as well, for which - since it is not a vaccination to be repeated annually - the opportunity is granted during the whole year [15].
Co-administering of the two vaccinations - influenza and pneumococcal - is recommended due to the fact that the results obtained in terms of safety and immune responses to co-administered pneumococcal and influenza vaccine are not inferior compared with each vaccine given alone [25].
Aim of the Study
The study aims to evaluate the possible correlation between pneumococcal vaccine administrations and SARS- CoV-2 virus infection found among HCPs from the Local Health Authority of Viterbo vaccinated against influenza in the last vaccination Campaign. The study did not consider Covid vaccination, as it was made mandatory in Italy for all healthcare workers by the 24 March 2022 Decree [26].
Specifically, the study aims to compare the trend of COVID infections - during the period from November 1, 2021 to May 31, 2022 - among health care workers who received regular flu vaccination, and to assess whether those who also received pneumococcal vaccination during their lifetime were better protected against SARS-CoV-2.
Materials and Methods
The scenario under study was defined through the extrapolation of data recorded on the Lazio Region’s Regional Vaccination Registry (AVR).
The sample of the 964 individuals consists of HCPs who underwent vaccination during the last Vaccination Campaign
by GPs or at one of the vaccination centers of the Local Health Authority (ASL) of Viterbo.
Lazio is a region in central Italy, with Rome as its capital, covering about 17,232 km2 [27], with a population of 5,715,190 [28]. The Province of Viterbo, with a population of 307,592 inhabitants [28] and an extension of 3,615 km2 [29], represents its largest province, after the Metropolitan City of Rome Capital [27].
Using data from patients who received the flu vaccine, we explored the relationship between pneumococcal vaccination and COVID-19 test positivity in healthcare workers in the ASL of Viterbo who were vaccinated against influenza in the last Flu Campaign.
Data on influenza vaccinations administered to healthcare workers in the ASL of Viterbo refer to the period October 2021-January 2022. Within the identified cohort, the number of any pneumococcal vaccination administrations performed over a lifetime was noted.
The following data referring to health care personnel in the ASL were considered: a. Number of healthcare workers who underwent influenza vaccination during the last vaccination Campaign;
b. Number of health care workers who underwent influenza vaccination during the last vaccination Campaign and also received lifetime pneumococcal vaccination;
c. Number of health care workers who underwent influenza vaccination during the last vaccination Campaign and were also infected with SARS-CoV-2 during the period November 1, 2021 to May 31, 2022;
d. Number of health care workers who received influenza vaccination during the last vaccination Campaign and also received pneumococcal vaccination during their lifetime and were infected with SARS-CoV-2 during the period November 1, 2021 - May 31, 2022.
The scenario identified was reprocessed using Windows Access, Excell software and access to the Lazio Region’s AVR platform in use at the Public Health and Hygiene Service of the Prevention Department of the Local Health Authority of Viterbo.
Results
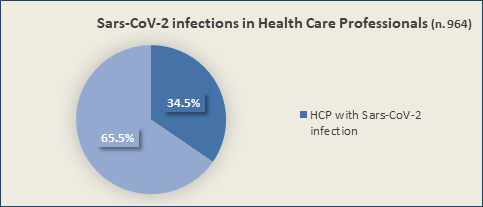
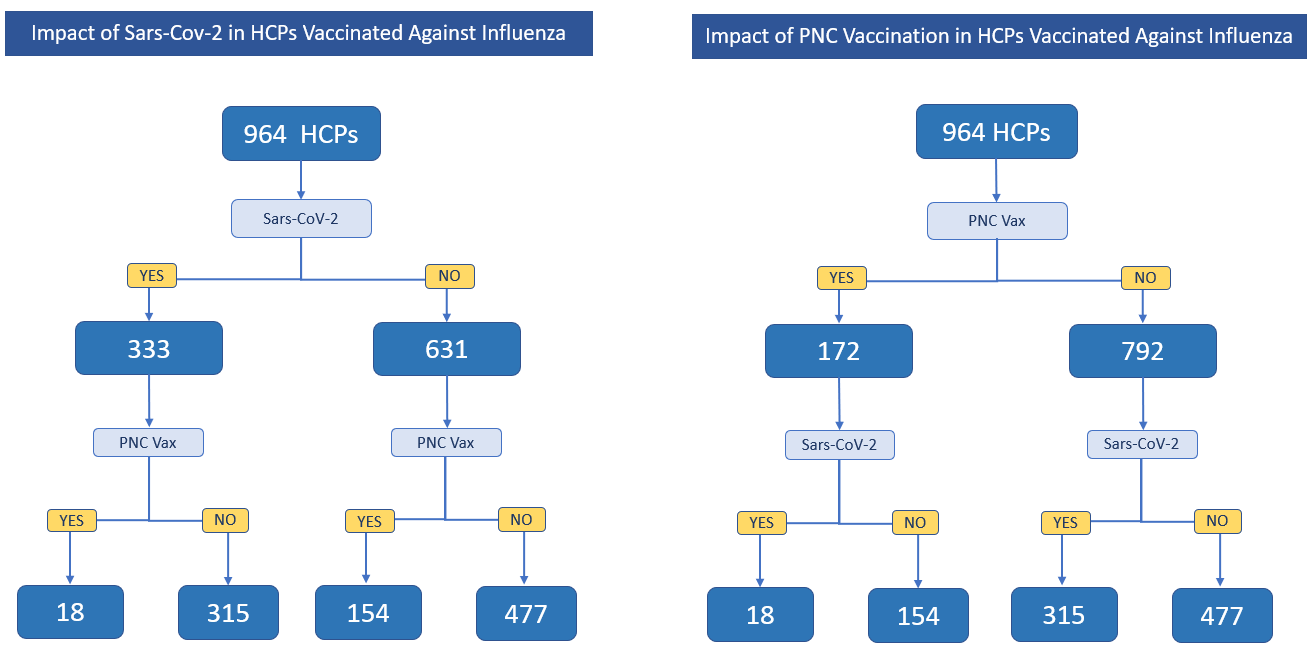
Among the 964 HCPs in the Local Health Authority of Viterbo who had been immunized for influenza in the last Vaccination Campaign, 333 - corresponding to 34.5% - were found to be infected with Sars-CoV-2 during the period November 1, 2021 to May 31, 2022. HCPs who did not contract the infection during the reporting period were the 65.5% (631 HCPs) (Figure 1).
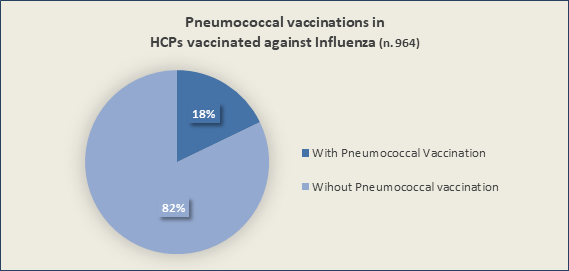
The 964 HCPs who were immunized for influenza, 172 (18%) had also received the pneumococcal vaccination in their lifetime, compared to the 792 (82%) who had never received pneumococcal vaccination in their lifetime (Figure 2).
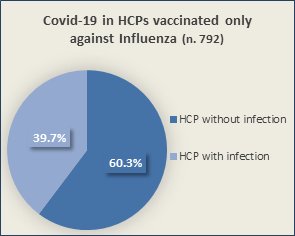
Among the 792 health care workers who underwent influenza vaccination during the last vaccination Campaign and had never received pneumococcal vaccination in their lifetime, 39.7% (315 HCPs) contracted SARS-CoV-2 infection during the period November 1, 2021 to May 31, 2022 compared with 477 (60.3%) uninfected (Figure 3). In
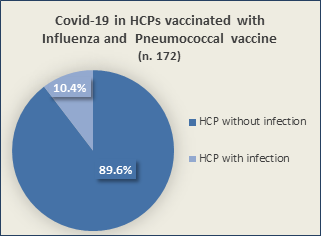
Among the 631 Sanitarians who did not test positive for Covid-19 during the reporting period, 154 (24.4%) were those who had received pneumococcal vaccination during their lifetimes, compared with the 477 (75.6%) who received only influenza vaccination during the last vaccination Campaign but never received pneumococcal vaccination contrast, during the same period, among the 172 health care workers who had also received pneumococcal vaccination in their lifetimes, 10.4 percent (18 HCPs) swabbed positive for Sars-CoV-2, compared with 154 (89.6%) without infection (Figure 4).
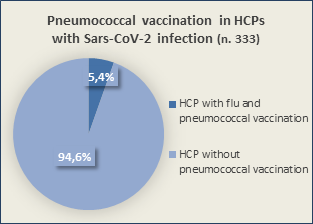
(Figure 5). In contrast, when analyzing the 333 health care workers who tested positive on swabs for SARS-CoV-2, only 18 (5.4%) had undergone pneumococcal vaccination during their lifetime, compared with 315 (94.6%) who had never undergone pneumococcal vaccination (Figure 6).
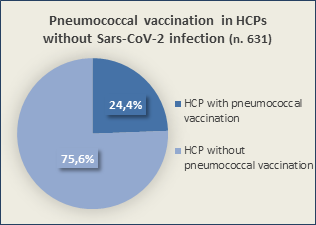
Figure 5. Pneumococcal vaccination in HCPs without Sars- CoV-2 infection Figure 6. Pneumococcal vaccination in HCPs with Sars-CoV-2 infection The figure below (Figure 7) shows the results, in numerical terms, regarding Sars-CoV-2 infections in the 964 sanitarians vaccinated against influenza during the last Vaccine Campaign according to their adherence to the Pneumococcal Vaccine Program.
Data analysis shows that 65.5% of the HCPs in our sample, all of whom were vaccinated against influenza
during the last Vaccine Campaign, did not contract Sars- CoV-2 infection during the observation period that ran from November 1, 2021 to May 31, 2022.
Among the 172 HCPs who had also undergone pneumococcal vaccination during their lifetime, only 10.4% had Sars-CoV-2 infection, compared with 39.7% infections among those who had had only flu vaccination.
Discussion and Conclusion
Our study shows that pneumococcal vaccinations were found to be associated with a reduced likelihood of SARS- CoV-2 infection in healthcare workers vaccinated against influenza in the last CVA. These findings need to be confirmed by further investigation, but they are relevant given the likelihood of coexistence of influenza, bacterial infections, and COVID-19 in the upcoming fall-winter season.
It is likely that the upcoming fall-winter season will see a resurgence of influenza activity to levels similar to or even higher than pre-pandemic levels; the potential co-circulation of influenza, Sars-CoV-2 and other respiratory pathogens could substantially increase the pressure on our National Health Service.
In addition, the gradual abandonment of individual protection systems and social distancing, could lead-in the coming autumn-winter season-to increased co-circulation of pathogens, viral and bacterial.
One of the most important measures to counteract this problem is to develop an enhanced vaccination strategy during the next vaccination season, achieving higher vaccination coverages in those at risk. Awareness campaigns are also needed for populations through targeted and appropriate communication consistent with scientific evidence. All health professionals should be encouraged to vaccinate and promote vaccination [30].
Analysis of the collected data suggests that pneumococcal and influenza vaccinations are associated with a lower likelihood of infection by SARS-CoV-2.
Considering that multiple respiratory co-infections can lead-especially in the frail and elderly-to serious and even fatal consequences, our findings support the need for Public Health Programs to strengthen the upcoming Pneumococcal and Influenza Vaccination Campaigns, to be combined with that for SARS-CoV-2.
References
-
Doherty TM, Connolly MP, Del Giudice G (2018) Vaccination programs for older adults in an era of demographic change_._ Eur Geriatr Med 9(3): 289-300.
-
Dari S, Simeone V, Aquilani S (2019) Tetravalent Flu Vaccine in Italy. A Budget Impact Analysis (BIA). 2(2): 000115.
-
Maltezou HC, Theodoridou K, Poland G (2020) Influenza immunization and COVID-19. Vaccine 38(39): 6078- 6079.
-
Iuliano AD, Roguski KM, Chang HH (2018) Global Seasonal Influenza-associated Mortality Collaborator Network. Estimates of global seasonal influenza- associated respiratory mortality: a modelling study_._ Lancet 391(10127): 1285-1300.
-
Maltezou HC, Poland GA (2016) Immunization of Health- Care Providers: Necessity and Public Health Policies_._ Healthcare (Basel) 4(3): 47.
-
Conlon A, Ashur C, Washer L (2021) Impact of the influenza vaccine on COVID-19 infection rates and severity. Am J Infect Control 49(6): 694-700.
-
Wang X, Kulkarni D, Dozier M (2020) Influenza vaccination strategies for 2020-21 in the context of COVID-19. J Glob Health 10(2):0 21102.
-
Gasparini R, Amicizia D, Lai PL (2016) Influenza vaccination: from epidemiological aspects and advances in research to dissent and vaccination policies. J Prev Med Hyg 57(1): E1-4.
-
Epicentro (2022) Istituto Superiore di Sanità.
-
(2022) ALLEGATO A. Campagna di vaccinazione antinfluenzale 2022-23 - Protocollo operativo.
-
Howard LM (2021) Is There an Association Between Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Streptococcus pneumoniae?. Clin Infect Dis 72(5): e76-e78.
-
Smith AM, Huber VC (2018) The Unexpected Impact of Vaccines on Secondary Bacterial Infections Following Influenza. Viral Immunol 31(2): 159-173.
-
Dari S, Verginelli F, Aquilani S (2014) Aspetti di farmacoeconomia collegati al vaccino antipneumococcico ASL Viterbo Health economics and therapeutic pathways 15(4): 155-159.
-
ALLEGATO B (2022) Programma di vaccinazione con vaccino anti-pneumococcico. Nota operativa.
-
(2022) World Health Organization. Coronavirus disease (COVID-19) pandemic.
-
Heinzerling A, Stuckey MJ, Scheuer T (2020) Transmission of COVID-19 to Health Care Personnel During Exposures to a Hospitalized Patient - Solano County, California, February 2020. MMWR Morb Mortal Wkly Rep 69(15): 472-476.
-
Maltezou HC, Dedoukou X, Tseroni M (2020) SARS- CoV-2 Infection in Healthcare Personnel with High-risk Occupational Exposure: Evaluation of 7-Day Exclusion from Work Policy. Clin Infect Dis 71(12): 3182-3187.
-
WHO (2020) Health Emergency Dashboard.
-
Dari S, Bragaglia G, Aquilani S (2022) Implementation and Monitoring of the Vaccination Campaign against Sars-CoV-2 virus in the Local Health Authority of Viterbo_._ Journal of Quality in Health Care & Economics 5(2): 000261.
-
Tayar E, Abdeen S, Alah MA (2022) Effectiveness of influenza vaccination against SARS-CoV-2 infection among healthcare workers in Qatar_._
-
Callaway E _(2022)_ Flu vaccine could cut COVID risk. Nature 605(7911): 602.
-
EpiCentro (2020) Coperture della vaccinazione antinfluenzale in Italia.
-
Fateh-Moghadam P, Lechthaler T, Monterosso M (2020) La vaccinazione antinfluenzale del personale sanitario dell’ospedale S. Chiara di Trento_._
-
Thompson AR, Klein NP, Downey HJ (2019) Coadministration of 13-valent pneumococcal conjugate and quadrivalent inactivated influenza vaccines in adults previously immunized with polysaccharide pneumococcal vaccine 23: a randomized clinical trial_._ Hum Vaccin Immunother 15(2): 444-451.
-
(2020) Decreto legge 24 marzo 2022 n. 24 Disposizioni urgenti per il superamento delle misure di contrasto alla diffusione dell’epidemia da COVID-19, in conseguenza della cessazione dello stato di emergenza.
-
(2022) Tutta Italia, le provincie Laziali per densità.
-
(2022) Geo Demo ISTAT.
-
(2022) Provincia di Viterbo.
-
Ieraci R (2020) Vaccinazione autunno-inverno, tra influenza e Covid cosa ci aspetta.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda