Neurodegenerative Disorders Tendency in Adult Cuban Population
Introduction: Neurodegenerative diseases have a multifactorial etiology, based on genetics and triggering environmental factors, associated with the aging process of the population. Objectives: To describe the mortality and trend of Amyotrophic Lateral Sclerosis, Alzheimer's dementia and Parkinson's disease in Cuba and other countries during the period from 2015 to 2020. Methods Longitudinal descriptive observational study was carried out, which it classifies as chronological or temporal series, on mortality and behavioral trend of Amyotrophic Lateral Sclerosis, Alzheimer's disease and Parkinson's disease in Cuba, during the period 2015 to 2020. Results: The data obtained show that Alzheimer's disease has a tendency to decrease mortality, unlike Parkinson's disease that is observed a slight increase, while in Amyotrophic Lateral Sclerosis the behavior is stable. Deaths in Parkinson's and Alzheimer's disease occurred between 75-79 years of age, while in Amyotrophic Lateral Sclerosis it was 65-69 years old. There was predominance of the male sex in Parkinson's and Amyotrophic Lateral Sclerosis. Women predominated in Alzheimer's disease. The three neurodegenerative diseases occurred in patients with white skin color. The highest number of deaths were shown in the provinces of Havana and Holguín. Conclusions: The prevalence and incidence of dementia and Alzheimer's disease increases exponentially, in relation with Parkinson´s disease the incidence vary widely throughout the world and the most significant risk factors are aging and men. Finally, the prevalence of Amyotrophic Lateral Sclerosis remains low due to high mortality, due to the lack of effective treatment at present.
Introduction
The prevalence and incidence of numerous neurological diseases has increased considerably in recent decades, especially those related to the aging process [1]. Global population growth aged 60 and over is expected to happen exponentially; thus, in the next 15 years the number of older people in Latin America and the Caribbean will increase by 71%, followed by Asia (66%), Africa (64%), Oceania (47%), North America (41%) and Europe (23%) [2].
Cuba is the fourth oldest country in Latin America. According to the current population pyramid, it has 11,326,616 inhabitants, with a female population of 50.35% of the total, slightly higher than that of men. Since 2017, the proportion of the population aged 60 and over has experienced an uninterrupted increase that reached 20.1%, with projections of becoming in 2025 the second oldest country in Latin America and that by 2030 the population aged 60 or older will exceed 30%. The provinces with the highest degree of aging are Villa Clara 24%, Havana 21.9% and Sancti Spíritus 21.8% [3].
Neurodegenerative diseases acquire great prominence due to their high prevalence and social cost. They are defined as pathologies, hereditary or acquired, in which progressive dysfunction of the Central Nervous System (CNS) occurs, according to the National Institute of Neurological Disorder and Stroke Study (NINDSS), more than 600 are recognized, among which Alzheimer’s Disease (AD), Parkinson’s Disease (PE), Huntington’s Disease (HD), Amyotrophic Lateral Sclerosis (ALS) and Multiple Sclerosis (MS) stand out for their high prevalence and severity [4].
Taking into account these data, it is expected that mortality in Cuba from Parkinson’s Disease, Alzheimer’s Disease and Amyotrophic Lateral Sclerosis will increase in older adults in the coming years, so we propose the study of the trend of these diseases, which would serve as an evaluation tool in the analysis of the situation and public health care whose mortality data will serve as a To attend to and design action plans for improvements in early diagnosis, risk factors, lifestyles and social inclusion.
Disease trends fall in the field of epidemiology which has important predictive means, not only in terms of the possibility of getting sick, it also allows to predict the behavior of a disease in the community and even calculate the projection that the disease will have in the following year or years. This article aims to describe the mortality and trend of Amyotrophic Lateral Sclerosis, Alzheimer’s dementia and Parkinson’s disease in Cuba, during the period from 2015 to 2020. The data presented here will serve as a scientific contribution for the planning of material and human resources to decision makers, which will make it easier to maintain and improve the quality of care according to the needs of the population to attend and design plans of measures for improvements in early diagnosis, risk factors, lifestyles and social inclusion.
Methods
Context and Classification of the Study
Longitudinal descriptive observational study was carried out, which classifies as chronological or temporal series, on the trend of 3 neurodegenerative diseases; Amyotrophic Lateral Sclerosis, Alzheimer’s dementia and Parkinson’s disease in Cuba during the period 2015 to 2020. First, the method of documentary analysis and bibliographic review was used. In a second moment, a time series or chronological analysis was carried out with the mortality statistics of each of the diseases included in the study.
For the selection of the sample of the first objective, the following criteria were taken into account: Inclusion criteria: full-text articles, related to the topic of the work (Dementia and/Alzheimer, Parkinson’s disease and Amyotrophic Lateral Sclerosis), date of publication between 2015 and 2020 and documents written in English and/or Spanish. Exclusion Criteria: final degree, master’s and doctoral theses.
Statistical Processing of the Data
During the search process, MEDLINE (via PubMed), Cochrane Library, Scielo, UpToDaTe, Dialnet and academic Google were used as databases, in order to ensure a wide and effective search. First, the search in the different databases is limited by combining the search terms DeCS and MeSH, using the Boolean operator AND and applying the inclusion criterion: publication date between 2015 and 2020.
| Decs: | MesH: |
|---|---|
| Demencia y Enfermedad de Alzheimer, | Dementia and Alzheimer Disease |
| Enfermedad de Parkinson | Parkinson Disease |
| Esclerosis Lateral Amiotrófica | Amyotrophic lateral sclerosis |
| Enfermedad | Disease |
| Epidemiología | Epidemiology |
| Etiología | Etiology |
| Diagnóstico | Diagnostic |
| Tratamiento | Treatment |
| Cuidados | Care |
| Enfermería | Nursing |
Analysis of the Information
For the analysis of time series, the mortality statistics of Alzheimer’s dementia, Parkinson’s disease and Amyotrophic Lateral Sclerosis in Cuba from 2015 to 2020 were used, the control variables requested were age group, sex, skin color and provinces.
Sources of Information Used
Statistical Yearbook of Cuba for the years 2015, 2016, 2017, 2018, 2019 and 2020. Cuban Mortality Database available at the National Directorate of Statistics of the Ministry of Public Health and made up with the outputs of the Statistical Information System of deaths that are available at the National Directorate of Statistics of the Ministry of Public Health.
Statistical Processing
Mortality statistics have been processed in accordance with the provisions of ICD-10. The series of data collected from the different neurological diseases under study from 2015 to 2020, was stored in a database that were statistically processed. The trend analysis was carried out for each disease. Time series were built and percentage indicators, general and sex-specific rates were calculated.
Seasonal decomposition methods were used to decompose the series, the moving average method was used. To forecast, an adjustment of the trend of the series was made. A linear adjustment was used, with a p less than 0.05. The adjusted coefficients were determined. This analysis made it possible to evaluate the percentage of variability of the data explained by the model so that the closer to 1 is the
Results
value, the better represented the data are.
To forecast and provide reasonable forecasts for immediate prediction horizons, in this case two years; smoothing or smoothing methods were used.
- In the case of series without trend or seasonality, the moving average model and the exponential smoothing model were applied.
- In the case of trendy non-seasonal series, Holt’s classic model was applied. The results were summarized in statistical tables and simple arithmetic graphs. In all cases, the equation of the adjustment model and the adjustment coefficient R2 were specified.
Ethical Considerations
The research was carried out in accordance with the ethical principles of the research.
The information requested from the Directorate of Medical Records and Health Statistics was used only for the purpose of the thesis.
Limit and Scope of the Investigation
The present study presents some limitations that are specific to the characteristics of this type of descriptive analysis and that would be associated with the quality and quantity of health records. In addition, it must be taken into account that the data comes from several sources, there may be no recorded information or initial inaccuracies. However, this is a limitation attributable to most of the studies published in this field.
| Province | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | % | No | % | No | % | No | % | No | % | No | % | |
| Pinar del Rio | 15 | 4,34 | 17 | 5,11 | 23 | 6,42 | 18 | 4,76 | 12 | 2,75 | 16 | 3,66 |
| Artemisa | 16 | 4,62 | 23 | 6,91 | 22 | 6,15 | 16 | 4,23 | 30 | 6,88 | 29 | 6,64 |
| Havana | 142 | 41,04 | 124 | 37,24 | 127 | 35,47 | 108 | 28,57 | 136 | 31,19 | 136 | 31,12 |
| Mayabeque | 15 | 4,34 | 9 | 2,70 | 10 | 2,79 | 12 | 3,17 | 18 | 4,13 | 11 | 2,52 |
| Matanzas | 21 | 6,07 | 28 | 8,41 | 22 | 6,15 | 32 | 8,47 | 45 | 10,32 | 30 | 6,86 |
| Villa Clara | 16 | 4,62 | 22 | 6,61 | 23 | 6,42 | 42 | 11,11 | 31 | 7,11 | 42 | 9,61 |
| Cienfuegos | 22 | 6,36 | 12 | 3,60 | 20 | 5,59 | 23 | 6,08 | 27 | 6,19 | 20 | 4,58 |
| Santi Spíritus | 17 | 4,91 | 12 | 3,60 | 18 | 5,03 | 22 | 5,82 | 33 | 7,57 | 44 | 10,07 |
| Ciego de Ávila | 6 | 1,73 | 8 | 2,40 | 8 | 2,23 | 14 | 3,70 | 13 | 2,98 | 7 | 1,60 |
| Camagüey | 18 | 5,20 | 12 | 3,60 | 13 | 3,63 | 12 | 3,17 | 19 | 4,36 | 17 | 3,89 |
| Las Tunas | 11 | 3,18 | 8 | 2,40 | 16 | 4,47 | 11 | 2,91 | 15 | 3,44 | 17 | 3,89 |
| Holguín | 21 | 6,07 | 23 | 6,91 | 21 | 5,87 | 31 | 8,20 | 23 | 5,28 | 32 | 7,32 |
| Granma | 6 | 1,73 | 9 | 2,70 | 8 | 2,23 | 11 | 2,91 | 7 | 1,61 | 13 | 2,97 |
| Santiago de Cuba | 14 | 4,05 | 19 | 5,71 | 20 | 5,59 | 18 | 4,76 | 18 | 4,13 | 16 | 3,66 |
| Guantánamo | 4 | 1,16 | 6 | 1,80 | 6 | 1,68 | 6 | 1,59 | 6 | 1,38 | 4 | 0,92 |
| Isla de la Juventud | 2 | 0,58 | 1 | 0,30 | 1 | 0,28 | 2 | 0,53 | 3 | 0,69 | 3 | 0,69 |
| Total | 346 | 100 | 333 | 100 | 358 | 100 | 378 | 100 | 436 | 100 | 437 | 100,00 |
Table 2: Deaths in Alzheimer’s disease as a direct cause of death according to provinces, Cuba, 2015-2020.
Source: Database. National Directorate of Health Statistics, Cuba, 2015-2020. Table 1: Deaths in Alzheimer’s disease as a direct cause of death according to provinces, Cuba, 2015-2020.
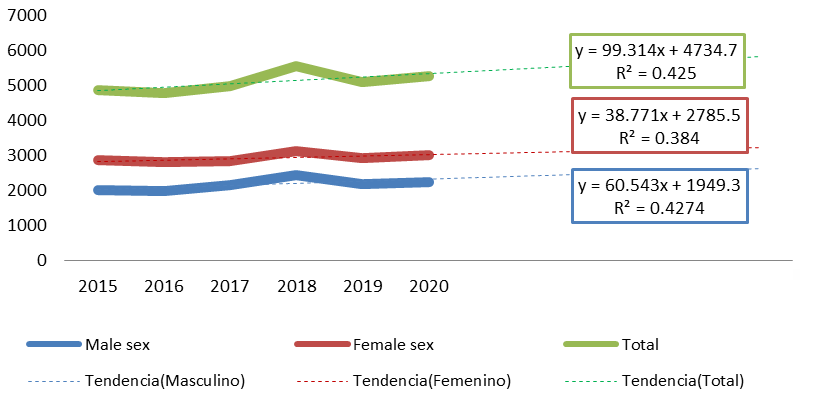
Source: Database. National Directorate of Health Statistics. Cuba. 2015-2020 Graph 1: Deaths in Alzheimer’s disease according to sex in Cuba during the years 2015 to 2020.
| Province | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | % | No | % | No | % | No | % | No | % | No | % | |
| Pinar del Rio | 13 | 2,37 | 25 | 4,50 | 21 | 3,38 | 26 | 3,96 | 45 | 6,17 | 35 | 5,22 |
| Artemisa | 26 | 4,74 | 18 | 3,24 | 15 | 2,42 | 17 | 2,59 | 27 | 3,70 | 20 | 2,98 |
| Havana | 102 | 18,61 | 113 | 20,36 | 129 | 20,77 | 129 | 19,63 | 131 | 17,97 | 112 | 16,69 |
| Mayabeque | 18 | 3,28 | 10 | 1,80 | 18 | 2,90 | 18 | 2,74 | 21 | 2,88 | 18 | 2,68 |
| Matanzas | 36 | 6,57 | 35 | 6,31 | 47 | 7,57 | 35 | 5,33 | 53 | 7,27 | 32 | 4,77 |
| Villa Clara | 64 | 11,68 | 63 | 11,35 | 69 | 11,11 | 80 | 12,18 | 86 | 11,80 | 83 | 12,37 |
| Cienfuegos | 21 | 3,83 | 25 | 4,50 | 26 | 4,19 | 41 | 6,24 | 34 | 4,66 | 38 | 5,66 |
| Santi Spíritus | 36 | 6,57 | 44 | 7,93 | 41 | 6,60 | 45 | 6,85 | 59 | 8,09 | 39 | 5,81 |
| Ciego de Ávila | 19 | 3,47 | 16 | 2,88 | 25 | 4,03 | 26 | 3,96 | 23 | 3,16 | 17 | 2,53 |
| Camagüey | 34 | 6,20 | 46 | 8,29 | 44 | 7,09 | 45 | 6,85 | 49 | 6,72 | 48 | 7,15 |
| Las Tunas | 26 | 4,74 | 13 | 2,34 | 28 | 4,51 | 22 | 3,35 | 18 | 2,47 | 28 | 4,17 |
| Holguín | 62 | 11,31 | 56 | 10,09 | 77 | 12,40 | 70 | 10,65 | 79 | 10,84 | 80 | 11,92 |
| Granma | 35 | 6,39 | 40 | 7,21 | 29 | 4,67 | 44 | 6,70 | 46 | 6,31 | 63 | 9,39 |
| Santiago de Cuba | 46 | 8,39 | 36 | 6,49 | 36 | 5,80 | 50 | 7,61 | 41 | 5,62 | 44 | 6,56 |
| Guantánamo | 10 | 1,82 | 12 | 2,16 | 12 | 1,93 | 6 | 0,91 | 15 | 2,06 | 10 | 1,49 |
| Isla de la Juventud | 0 | 0,00 | 3 | 0,54 | 4 | 0,64 | 3 | 0,46 | 2 | 0,27 | 4 | 0,60 |
| Total | 548 | 100 | 555 | 100 | 621 | 100 | 657 | 100 | 729 | 100 | 671 | 100 |
Table 3: Behavior of deaths in Parkinson’s disease as a direct cause of death according to provinces, Cuba, 2015-2020.
Source: Database, National Directorate of Health Statistics, Cuba, 2015-2020. Table 2: Behavior of deaths in Parkinson’s disease as a direct cause of death according to provinces, Cuba, 2015-2020.
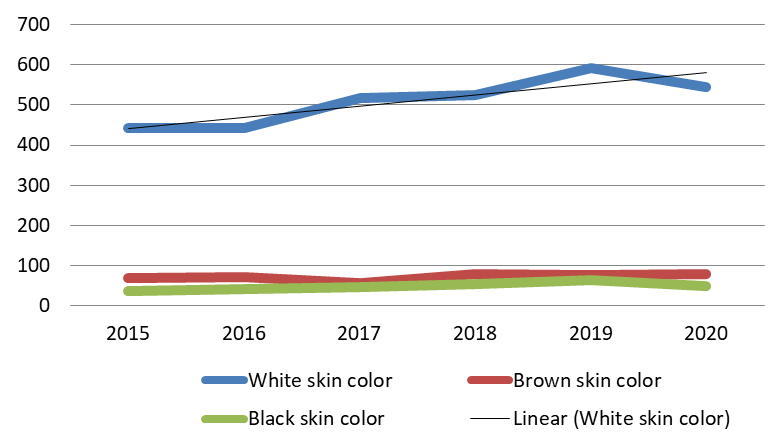
Source: Database. National Directorate of Health Statistics. Cuba. 2015-2020 Graph 2: Behavior of deaths in Parkinson’s disease as a direct cause of death according to skin color. Cuba. 2015-2020.
| Age Group | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | % | No | % | No | % | No | % | No | % | No | % | |
| <1 | 1 | 0,93 | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0 |
| 01-abr | 0 | 0,00 | 0 | 0,00 | 1 | 1,10 | 0 | 0,00 | 1 | 1,08 | 0 | 0 |
| 15 - 19 | 0 | 0,00 | 1 | 1,08 | 2 | 2,20 | 0 | 0,00 | 0 | 0,00 | 0 | 0 |
| 20 - 24 | 0 | 0,00 | 3 | 3,23 | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0 |
| 25 - 29 | 1 | 0,93 | 1 | 1,08 | 1 | 1,10 | 0 | 0,00 | 0 | 0,00 | 0 | 0 |
| 30 - 34 | 1 | 0,93 | 0 | 0,00 | 1 | 1,10 | 1 | 1,11 | 0 | 0,00 | 0 | 0 |
| 35 - 39 | 2 | 1,85 | 0 | 0,00 | 0 | 0,00 | 3 | 3,33 | 1 | 1,08 | 0 | 0 |
| 40 - 44 | 5 | 4,63 | 4 | 4,30 | 1 | 1,10 | 1 | 1,11 | 1 | 1,08 | 0 | 0 |
| 45 - 49 | 5 | 4,63 | 4 | 4,30 | 8 | 8,79 | 6 | 6,67 | 4 | 4,30 | 0 | 0 |
| 50 - 54 | 10 | 9,26 | 14 | 15,05 | 7 | 7,69 | 13 | 14,44 | 8 | 8,60 | 0 | 0 |
| 55 - 59 | 9 | 8,33 | 10 | 10,75 | 9 | 9,89 | 10 | 11,11 | 17 | 18,28 | 0 | 0 |
| 60 - 64 | 11 | 10,19 | 5 | 5,38 | 12 | 13,19 | 13 | 14,44 | 18 | 19,35 | 0 | 0 |
| 65 - 69 | 24 | 22,22 | 15 | 16,13 | 12 | 13,19 | 14 | 15,56 | 15 | 16,13 | 0 | 0 |
| 70 - 74 | 15 | 13,89 | 20 | 21,51 | 15 | 16,48 | 14 | 15,56 | 12 | 12,90 | 0 | 0 |
| 75 - 79 | 14 | 12,96 | 7 | 7,53 | 9 | 9,89 | 9 | 10,00 | 7 | 7,53 | 0 | 0 |
| 80 - 84 | 4 | 3,70 | 7 | 7,53 | 9 | 9,89 | 4 | 4,44 | 9 | 9,68 | 0 | 0 |
| 85 - 89 | 4 | 3,70 | 2 | 2,15 | 3 | 3,30 | 2 | 2,22 | 0 | 0,00 | 0 | 0 |
| 90 - 94 | 2 | 1,85 | 0 | 0,00 | 1 | 1,10 | 0 | 0,00 | 0 | 0,00 | 0 | 0 |
| 95 - 99 | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0 |
| 100 y + | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0,00 | 0 | 0 |
| Total | 108 | 100,00 | 93 | 100,00 | 91 | 100,00 | 90 | 100,00 | 93 | 100,00 | 0 | 0 |
Table 4: Deaths in amyotrophic lateral sclerosis as a direct cause of death according to age group. Cuba. 2015-2020.
Source: Database. National Directorate of Health Statistics, Cuba, 2015-2020. Table 3: Deaths in amyotrophic lateral sclerosis as a direct cause of death according to age group. Cuba. 2015-2020.
| Province | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | % | No | % | No | % | No | % | No | % | No | % | |
| Pinar del Rio | 2 | 1,85 | 7 | 7,53 | 5 | 5,49 | 7 | 7,78 | 4 | 4,30 | 2 | 2,15 |
| Artemisa | 7 | 6,48 | 6 | 6,45 | 3 | 3,30 | 5 | 5,56 | 6 | 6,45 | 2 | 2,15 |
| Havana | 20 | 18,52 | 16 | 17,20 | 26 | 28,57 | 18 | 20,00 | 20 | 21,51 | 23 | 24,73 |
| Mayabeque | 8 | 7,41 | 3 | 3,23 | 2 | 2,20 | 2 | 2,22 | 1 | 1,08 | 1 | 1,08 |
| Matanzas | 11 | 10,19 | 4 | 4,30 | 4 | 4,40 | 5 | 5,56 | 6 | 6,45 | 4 | 4,30 |
| Villa Clara | 12 | 11,11 | 11 | 11,83 | 12 | 13,19 | 6 | 6,67 | 9 | 9,68 | 9 | 9,68 |
| Cienfuegos | 2 | 1,85 | 3 | 3,23 | 1 | 1,10 | 9 | 10,00 | 2 | 2,15 | 3 | 3,23 |
| Santi Spíritus | 6 | 5,56 | 8 | 8,60 | 7 | 7,69 | 7 | 7,78 | 5 | 5,38 | 6 | 6,45 |
| Ciego de Ávila | 6 | 5,56 | 3 | 3,23 | 1 | 1,10 | 2 | 2,22 | 4 | 4,30 | 2 | 2,15 |
| Camagüey | 1 | 0,93 | 6 | 6,45 | 5 | 5,49 | 4 | 4,44 | 7 | 7,53 | 7 | 7,53 |
| Las Tunas | 13 | 12,04 | 5 | 5,38 | 8 | 8,79 | 5 | 5,56 | 3 | 3,23 | 2 | 2,15 |
| Holguín | 9 | 8,33 | 9 | 9,68 | 13 | 14,29 | 5 | 5,56 | 11 | 11,83 | 19 | 20,43 |
| Granma | 3 | 2,78 | 2 | 2,15 | 0,00 | 3 | 3,33 | 4 | 4,30 | 3 | 3,23 | |
| Santiago de Cuba | 5 | 4,63 | 5 | 5,38 | 1 | 1,10 | 7 | 7,78 | 5 | 5,38 | 9 | 9,68 |
| Guantánamo | 2 | 1,85 | 4 | 4,30 | 3 | 3,30 | 3 | 3,33 | 5 | 5,38 | 1 | 1,08 |
| Isla de la Juventud | 1 | 0,93 | 1 | 1,08 | 0,00 | 2 | 2,22 | 1 | 1,08 | 0 | 0,00 | |
| Total | 108 | 100,00 | 93 | 100,00 | 91 | 100,00 | 90 | 100,00 | 93 | 100,00 | 93 | 100,00 |
Table 5: Amyotrophic lateral sclerosis as a direct cause of death according to provinces. Cuba. 2015-2020.
Source: Database. National Directorate of Health Statistics, Cuba, 2015-2020. Table 4: Amyotrophic lateral sclerosis as a direct cause of death according to provinces. Cuba. 2015-2020.
Discussion
In Cuba, the aging process has had an increase in the proportion of people aged 60 and over in recent years, in relation to the total population, with a history of 11.3% of people over 60 years of age (1985) to 20.4% in 2018, indicating its location in the aging group III (GE-III), having more than 15% of its total population aged 60 and over. Thus, at the end of 33 years, aging has increased by 9.1 percentage points [5].
Alzheimer’s Ddisease (AD)
It is the most frequent of dementias and contributes in 60 - 70% of cases. It is an anatomical-clinical entity of a degenerative nature and progressive course [6]. In 2018, 50 million people suffered from dementia worldwide and, of these, about 60 to 80% have Alzheimer’s disease. The prevalence of this pathology increases markedly with age, with an increase of more than 15 times between the ages of 65 and 85 [7]. Mortality from Alzheimer’s disease between 2000 and 2019 has doubled, increasing by 145%, that is, 1 in 3 older people dies from this pathology [8].
WHO mentions that women are disproportionately affected, globally, 65% of deaths are due to Alzheimer’s [9, 10, 11]. All of the above could be justified according to the years of survival, where women survive more than men about 9 years. In the provinces classified as the oldest, the proportional values of their population aged 60 and over exceed 20%, such as Villa Clara, Sancti Spiritus and Havana, where deaths from Alzheimer’s disease presented irregular behavior during the period of time contemplated by this research Table 1 & Graph 1.
According to a meta-analysis of 157 epidemiological studies carried out around the world, the prevalence of dementia is, depending on the geographical area, between 58% for people over 60 years of age, showing an exponential growth pattern with age, doubling approximately every five years, and a predominance of the female sex [12, 13]. Another meta-analysis shows similar results, with a point prevalence of 4.8% and a prevalence of 6.9% in the community population aged 60 years and over [14]. This work also analyzed the causes of heterogeneity between studies such as age, diagnostic criteria and geographical scope.
In Latin America, a recent collaborative study based on population studies carried out in urban areas of six countries (Brazil, Chile, Cuba, Peru, Uruguay and Venezuela) indicates an overall prevalence of dementia of 7.1% in those over 65 years of age. However, there is a significant variability in the estimates, since, among the three studies carried out in Brazil, the prevalence was 2%, 7.1% and 8.8%, respectively, while in Uruguay it was 3.1%, and in Venezuela it was 13.1% (14.5). Another study, based on the 10/66 Dementia Research Group protocol, obtained estimates of the prevalence of dementia in the population aged 65 and over in different more homogeneous Latin American countries, with values ranging from 6.2% to 7.3% for an urban area of Venezuela and a rural area of Mexico, respectively, and between 9.8% and 12.6% for urban areas of the Dominican Republic and Cuba [15].
Parkinson’s Disease (PE)
Is the second most common neurodegenerative disease after Alzheimer’s disease. When analyzing the yearbooks of Cuba, it was observed that the greatest involvement by Parkinson’s disease occurred in the 75-79 age groups, followed by the ages between 80 and 84 years, data that coincide with the study by Condor et al. where the average age was 72.93 [16]; with that of Solís who found that PE occurs at 71 years [17, 18]. Rong S, et al. [19] states that The data obtained in the present study show that there is currently a tendency in both men and women to increase PE, with a predominance of deaths in male patients as well as the work of Condor in which the male sex predominated 58.3%. [16, 17, 18, 19, 20] Table 2 &Graph 2.
Moreira-Díaz LR, et al. [21] says that the Cuban population has an aging trend, so it is predicted that the prevalence of PE will increase. Hence, the number of patients with this pathology can be increased to 29,000 in two decades, indicating that in 2018 there were 665 deaths from this condition, with a crude rate for men of 7.4% and for women of 4.4%. All of the above could be explained by the hormonal protective factor against nerve-like conditions that women have, because it decreases the loss of dopaminergic neurons, which shows the male sex to be more likely to suffer.
In 2016, it was estimated that 6.1 million people in the world suffered from the disease, which more than doubled compared to the 1990 figure (2.5 million). In 2040 it is estimated that there will be about 17 million people affected. This makes Parkinson’s disease one of all neurological diseases, the fastest growing worldwide according to the global burden study of the disease [17]. This increase can be explained by several factors, including the aging of the population, exposure to environmental risk factors (such as certain toxins and the global decrease in smoking) and improvements in the diagnosis and reporting of cases of the disease, in addition to increased survival of patients due to the availability of effective treatments [18].
The risk of the disease seems to be determined by complex interactions between individual factors (such as age and the presence of certain genetic polymorphisms or mutations) and environmental factors. As for genetic risk factors, the one with the most robust evidence is the presence of mutations in the GBA gene (which codes for the lysosomal enzyme beta- glucocerebroxidase). Other genes identified are related to monogenic forms of the disease (such as LRRK-2 and SNCA) [20]. Age is the risk factor most consistently associated with Parkinson’s disease. There is a peak prevalence between 85 and 89 years of age (1.7% in men and 1.2% in women) and a decrease from this age. It is more common in men, with a male-female ratio of 1:4, with a prevalence that has doubled in the last 26 years [21, 22]. The age-standardized prevalence rate in Colombia was recently estimated at between 60 and 70 per 100,000 inhabitants (which in 2016 would represent 25,930 patients) [23]. However, in the Epineuro population study, carried out through two-phase, door-to-door surveys between 1995 and 1996, a prevalence of 470 per 100,000 inhabitants was found [24].
Amyotrophic Lateral Sclerosis (ALS) or Charcot Disease
It represents the third neurodegenerative disease in frequency, surpassed by AD and PE. In the present study, the incidence rates of Amyotrophic Lateral Sclerosis increased steadily by 3% per year for 22 years, from 1.6 to 3.3 X 100,000 per year. Older age, bulbar symptoms and men negatively affected survival. The median survival since diagnosis was 17.6 months and from the onset of symptoms it was 27.6 months [25]. The incidence rates of ALS in Europe and North America range from 1.5 to 2.7 X 100,000 person-years, while prevalence rates range from 2.7 to 7.4 X 100,000 person- years. The incidence of ALS increased with each decade, especially after the age of 40 [26, 27].
The incidence rates of Amyotrophic Lateral Sclerosis (ALS) in Europe and North America range from 1.5 to 2.7 per 100,000 person-years, while prevalence rates range from 2.7 to 7.4 per 100,000 person-years [28]. According to Castro and Colbs, in their study, it obtained a prevalence of 6.1 million inhabitants in 2017. Annual incidence between 1.2 cases/100,000 inhabitants/year in 2012 and 3.5 cases/100,000 inhabitants/year in 2016 [29, 30].
The highest number of patients who died from this pathology ranged from 65 to 74 years old, similar to studies by Maragakis who demonstrates an abrupt increase in ALS in the seventh decade, but the incidence in the elderly is uncertain [25, 31] Tables 3&4.
Lara et al. in their study of this entity, carried out in 2 stages (2005 - 2011) and (2012-2017), showed that this pathology predominated in patients with white skin color 63.9% and 66.7% respectively, followed by the mestizo race [32]. In relation to the distribution by sex, men predominated in both groups, with 54.14% in the first stage and 53.3% in the second [32, 33].
The male-female ratio is approximately 1.3 to 1.5 for sporadic ALS, although the ratio is close to unity in the age group over 70 years [25]. Studies carried out in Italy and Latin America bring differences. Thus, in Italy the male-to-female ratio is practically 1:1, in the population of Latin America the disease predominates in women [34]. The incidence of ALS increases with each decade, especially after the age of 40, and peaks at 74 years, then gradually decreases [35, 36].
It is estimated that half a million people are affected in the world. Due to its low prevalence due to its high and rapid mortality, ALS is considered a rare or “invisible” disease. Every year, 120,000 new cases of ALS are diagnosed worldwide, 17 every hour, and a 69% increase in the number of cases is expected by 2040 [25].
Conclusion
The prevalence and incidence of dementia and Alzheimer’s disease increases exponentially from the age of 65. As a result of the progressive aging of the population and the increase in life expectancy, the number of cases of dementia will increase over the coming decades. Recent studies indicate a slight decrease in the cumulative risk of age- and sex-adjusted dementia over the last few decades in some countries.
The prevalence and incidence of Parkinson’s disease vary widely throughout the world. In general, in Europe and the United States, the prevalence is higher than in other countries and is relatively uniform. In Asian countries, Latin America and Africa is inferior, especially in the latter continent. The most significant risk factors are aging and men.
The prevalence of Amyatrophic Lateral Sclerosis remains low (between 2 and 5 cases/100000 inhabitants), due to high mortality, due to the lack of effective treatment at present. Although there are differential criteria and a multitude of tests with which to make a definitive diagnosis, it is still difficult to reach the goal in the early stages of the disease, which translates into an average delay in diagnosis of one year.
Recommendations
- Develop diagnostic strategies and early intervention in this type of patient.
- Design research evaluating survival, years of life potentially lost and years of work for each of these diseases.center.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
References
-
Cubiles Troya S (2021) Biotechnology and neurodegenerative diseases. (Trabajo Fin de Grado Inédito). Universidad de Sevilla, Sevilla.
-
Hechavarría Ávila MM, Ramírez Romaguera M, García Hechavarria H, García Hechavarria A, Hechavarría Ávila MM, et al. (2018) The aging. Social and individual repercussion. Rev Inf Científica. diciembre de 97(6): 1173-1188.
-
Guerra JJL, Marante JPD, Salgado AMR, Peñalver AI, Guerrero EPG, et al. (2018) Determinants of the health status of the population and its influence on the development of cognitive disorders. Rev Cuba Salud Pública 44(1): 141-152.
-
Noa P, Coll Costa JL (2021) La actividad física en el adulto mayor con enfermedades crónicas no transmisibles. Rev Podium 16(1): 308-322.
-
Lara SC, Lara LC (2021) Vivir en/entre sonrisas? Envejecimiento y Alzheimer. CEDEM 33(1): 150-177.
-
World Health Organization (2021) Global status report on the public health response to dementia.
-
Castillo Reyes HE, López Contreras JR, Soto Maravilla MC, Vega Romero CG (2021) Apolipoprotein epsilon four and Alzheimer’s disease in patients of the Salvadoran Institute of Social Security. Crea Cienc Rev Científica 13(2): 33-46.
-
(2021) News_Alzheimer’s Association Report Examines Racial and Ethnic Attitudes on Alzheimer and Dementia Care.
-
Barragán Martínez D, García Soldevilla MA, Parra Santiago A, Tejeiro Martínez J (2019) Alzheimer disease. Med - Programa Form Médica Contin Acreditado. 1 de marzo de 12(74): 4338-4346.
-
Niu H, Álvarez-Álvarez I, Guillén-Grima F, Aguinaga- Ontoso I (2017) Prevalence and incidence of Alzheimer’s disease in Europe: A meta-analysis. octubre de 32(8): 523-532.
-
Ahmadi-Abhari S, Guzman-Castillo M, Bandosz P, Shipley MJ, Muniz-Terrera G, et al. (2017) Temporal trend in dementia incidence since 2002 and projections for prevalence in England and Wales to 2040: modelling study. BMJ 358: j2856.
-
Ziniti B, Stommel E, Linder E, torbick N (2018) Assessing Cyanobacterial Harmful Algal Blooms as Risk Factors for Amyotrophic Lateral Sclerosis. Neurotoxiciti Research 33(1): 1-14.
-
World Alzheimer Report 2019. Attitudes to dementia pp: 1-160.
-
Garre-Olmo J (2018) Epidemiología de la enfermedad de Alzheimer y otras demencias : Neurología.com. Rev Neurol 66(11): 377-386.
-
Cuba Antezana A, Anicama Hernández Á (2018) Prevalencia de síntomas no motores en pacientes con enfermedad de parkinson: una revision 7(3): 101-106.
-
Cóndor I, Atencio-Paulino J, Contreras -Cordova C (2019) Clinical epidemiological characteristics of parkinson’s disease in a national hospital of the peruvian highlands. Rev Fac Med Humana. 15 de octubre de 19(4): 14-21.
-
Solís M, Araneda J (2017) Parkinson’s disease (PD) has been associated with different environmental factors that increase its prevalence. diciembre de 55(4): 239- 246.
-
Valent F, Devigili G, Rinaldo S, Del Zotto S, Tullio A, (2018) The epidemiology of Parkinson’s disease in the Italian region Friuli Venezia Giulia: a population-based study with administrative data. Cienc Neurol 39(4): 669-704.
-
Rong S, Xu G, Liu B (2021) Trends in Mortality From Parkinson Disease in the United States, 1999-2019. Neurology 97(20): e1986-1993.
-
(2022) Etiology and pathogenesis of Parkinson disease. UpToDate.
-
Moreira Díaz LR, Palenzuela Ramos Y, Maciñeira Lara IE, Díaz González L, Torres Martinz Y (2019) Clinical and epidemiological variables in patients diagnosed with Parkinson’s disease. Rev Médica Sinerg 15(3): 7.
-
Leiva AM, Martínez Sanguinetti MA, Troncoso Pantoja C, Nazar G, Petermann Rocha F, et al. (2019) Chile lidera el ranking latinoamericano de prevalencia de enfermedad de Parkinson. Rev Méd Chile 147(4): 535-536.
-
Saavedra Moreno JS, Millán PA, Buriticá Henao OF (2019 Introduction, epidemiology and diagnosis of Parkinson’s disease. Acta Neurológica Colomb 35(3S1): 2-10.
-
Montalvo Herdoíza JP, Montalvo Perero PS, Alvear Toala LE, Intriago Mercado ER, Moreira Vera DV (2017) Prevalence of Parkinson’s Disease: Door-to-door Study in Manabi-Ecuador. RevEcuat.neurol 26(1): 23-25.
-
Maragakis N, Galvéz N (2022) Epidemiology and pathogenesis of amyotrophic lateral sclerosis – UpToDate.
-
Scull-Torres M (2018) Palliative care in amyotrophic lateral sclerosis. Medimay 25(1): 9.
-
Larson TC, Kaye W, Mehta P, Horton DK (2018) Amyotrophic Lateral Sclerosis Mortality in the United States, 2011–2014. Neuroepidemiology 51(1-2): 96- 103.
-
Aktekin MR, Uysal H (2020) Epidemiology of Amyotrophic Lateral Sclerosis. Turk J Neurol 26(3):187- 96.
-
Batty GD, Gale C (2021) Pre-Morbid Risk Factors for Amyotrophic Lateral Sclerosis: Prospective Cohort Study. Clin Epidemiol 13: 941-947.
-
Montano Peguero Y, Wong Guerra M, Fonseca Fonseca LA, Ramírez Sánchez J, Nuñez Figueredo Y (2018) Actualización de los avances en la investigación de la esclerosis lateral amiotrófica. Rev Cienc Farm Aliment 4(1): 38-52.
-
Palese F, Sartori A, Verriello L, Rosa S, Passador P, et al. (2018) Epidemiology of amyotrophic lateral sclerosis in Friuli-Venezia Giulia, North-Eastern Italy, 2002–2014_ a retrospective population-based study. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration 20(1-2): 1-10.
-
Lara G, Zaldivar V, Vaillant TZ, Morales AA, GiLl JG (2020) Amyotrophic Lateral Sclerosis, efficacy of its multidisciplinary management Institute of Neurology and Neurosurgery. 2005-2017. Panorama. Cuba y Salud 15 (3): 12-18.
-
Serra M, Valdes M (2019) Survival in patients with Amyotrophic Lateral Sclerosis. Rev Habanera Cienc Médicas 18(4): 607-623.
-
Longinetti E, Fang F (2019) Epidemiology of amyotrophic lateral sclerosis: an update of recent literature. Curr Opin Neurol 32(5): 771-776.
-
Logroscino G, Piccininni M (2019) Amyotrophic Lateral Sclerosis Descriptive Epidemiology: The Origin of Geographic Difference - PubMed. Rev Neuroepidemiology 52(2): 93-103.
-
Beard JD, Steege AL, Ju J, Lu J, Luckhaupt SE (2017) Schubauer-Berigan MK. Mortality from Amyotrophic Lateral Sclerosis and Parkinson’s Disease Among Different Occupation Groups-United States, 1985–2011. MMWR Morb Mortal Wkly Rep 66(27): 718-722.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda