Psychosocial Risk Factors Associated with Gestational Diabetes Mellitus a Scoping Review
Introduction: The prevalence of gestational diabetes mellitus (GDM) has increased worldwide and, of course, adverse outcomes for the health of the mother, fetus and neonate, and the resulting healthcare costs have increased. The World Health Organization affirms that healthy lifestyle habits that go with physical, mental, and psychosocial health and range from preconception to postpartum are essential to achieve successful pregnancies. Objective: Conducting a scoping review of the psychosocial risk factors associated with GDM. Materials and Methods: The databases consulted were PubMed / Medline and Cochrane. Studies on psychosocial risk factors in pregnant women older than 18 years, with a diagnosis of GDM, from 2010 to 2020, in English and Spanish, published in peer-reviewed journals, were selected. A standardized data extraction form was developed. Results: 1188 articles on this topic were found, 93 of which were selected according to the inclusion criteria. The findings yielded several main issues such as conflicts with cultural practices, social stigma, influence of ethnicity / race, low educational level, sleep quality, physical limitations, problems with breastfeeding, concern for the health of the mother and baby, low perception of risk of GDM and DM2 in the future, stress, anxiety and depression, limited knowledge about GDM, lack of partner / family / social support, low levels of self-care and self-efficacy in glycemic control, lack of support from health professionals and difficulties with changes in lifestyle. Discussion and Conclusion: All the identified psychosocial risk factors must be taken into account either by adapting existing prevention and promotion programs or by developing new programs. Interventions should not end with pregnancy and the psychological impact and risk of developing T2D after delivery should be considered, as well as multiethnic populations and the most demographically and socioeconomically vulnerable groups. In addition, they should be included in the Clinical Practice Guidelines and in prevention, promotion and intervention programs for the health and quality of life of women with GDM.
Introduction
Diabetes mellitus is a chronic disease with deadly, disabling, and costly consequences for individuals, families, communities, and countries. The incidence of diabetes risk factors is related to overweight, and obesity caused by the spread of unhealthy diets and sedentary lifestyles [1, 2, 3].
The prevalence of gestational diabetes mellitus (GDM) has also increased worldwide, yielding figures between 1 and 14% and, of course, adverse outcomes for the health of the mother, fetus and neonate and the resulting healthcare costs to cope with this condition have increased in the short and long-term [1, 3, 4, 5].
GDM refers to elevated blood glucose levels during pregnancy among women without previous diabetes and is characterized by complications in delivery and postpartum, fetus and early childhood.
Healthy lifestyle habits from preconception to postpartum are considered an important safeguard to counteract GDM and achieve successful pregnancies. Among the priorities established by the WHO are healthy diet and nutrition, weight control, physical activity, planned pregnancy and physical, mental and psychosocial health. It is important to intervene in modifiable risk factors such as diet and physical activity, but the psychosocial well-being of the mother and child is also important [1, 6].
Although it seems contradictory, the diagnosis of GDM represents a timely warning to make changes in one’s diet, physical activity, and psychosocial aspects because the sole diagnosis psychologically impacts the mother and as a consequence also the child [7].
The Spanish Diabetes Society (2019: 6) affirms that “The education of the pregnant diabetic patient constitutes a fundamental therapeutic aspect, since motivating these people to be protagonists of their own treatment means that it is possible to modify, to a great extent, their future clinical evolution through better metabolic control, reducing risk factors and their social cost and, what is more important, achieving a successful pregnancy”.
The psychosocial factors associated with gestational diabetes have been little studied in low and middle-income countries [8] such as those in Latin America, the data is scarce and in general dedicated to depression, anxiety, and stress, and, although these are an important part of the psychosocial risks for developing GDM they are not the only ones.
Likewise, these psychosocial risk factors have been studied more in relation to types 1 and 2 diabetes and are defined by the ADA [9] as those complex, environmental, social, behavioral, and emotional elements that influence living with diabetes and achieving satisfactory medical results and also psychological well-being. Depression is the psychosocial factor most commonly investigated in studies on diabetes [10], followed by studies on anxiety and psychological stress. Depression has been found to be associated with a 37-60% increased risk of developing diabetes [10, 11, 12]. These studies do not propose causality, but association or correlation, and they are longitudinal studies on type 1 and 2 diabetics and not women with GDM.
Moreover, personality factors are not well investigated in relation to diabetes, but it seems that hostility has been associated prospectively with an increase in fasting glucose and transversely with insulin resistance [13]. The precise mechanisms that link psychosocial risk factors and diabetes have not yet been defined and several explanations have been suggested: for example, this adverse relationship would be mediated by behavioral pathways such as poor diet, physical inactivity, excessive alcohol consumption, smoking [14] and lower adherence to self-care behaviors such as the consumption of medications to control diabetes [10, 15].
Therefore, it is necessary to evaluate the psychosocial risk factors associated with GDM and the health beliefs and behaviors of women with this condition that lead them to perceive a low risk of developing type 2 diabetes mellitus in the future, and present low fruit and vegetable consumption and a low level of physical activity. This reveals a clear knowledge-behavior gap about the necessary lifestyle modifications that can affect the adherence to treatment of women with GDM [16]. Due to the above, it is important that a multidisciplinary team (including psychology and psychiatry professionals) carries out a biopsychosocial risk assessment of pregnant women with GDM to establish if they need additional care [17].
According to Kalra B, et al. [18], it is necessary to address the psychosocial problems faced by women with GDM because pregnancy is itself a stressful condition, and a diabetic pregnancy leads to even greater stress, which requires a better psychological care, making it necessary to sensitize health professionals who treat this disease on this aspect.
The psychological discomfort suffered by women with complications such as GDM is a process that occurs on a continuum from the combination of different psychosocial risk factors associated with daily life to the context in which the pregnancy occurs, with moments of crisis and their previous obstetric experiences [19].
The emotional experience of women in the face of a high-risk pregnancy is a topic little studied by the Latin American scientific literature and the biomedical approach has prevailed as a solution [19, 20, 21]: it explains the disease depending on physical symptoms and leaves aside its social, psychological and behavioral dimensions, so it is important to develop a more critical approach focused on the study of the mental health of pregnant women within the setting of their daily life.
On the other hand, while studying some worldwide clinical practice guidelines on GDM, including that of NICE [22], that of Mexico and that of Colombia [23], it was found that psychosocial risk factors were not included (apart from stress, anxiety, and depression) as aspects that may influence the emotional impact of the diagnosis, the knowledge of this condition and its possible consequences.
In summary, psychosocial risk factors are multiple and diverse and can have an impact both on the development of GDM and on its course and prognosis. Due to their role, these factors can influence the effectiveness of prevention programs and interventions and, consequently, adherence to GDM treatment.
Considering the strong links between psychosocial risk factors and GDM and the WHO recommendations to include these factors in the treatment and health care of women with GDM from preconception to postpartum, the interest to carry out a scoping review on the psychosocial risk factors associated with GDM arose, which management will make it possible to propose or improve interventions for the health and quality of life of these women.
Materials and Methods
Study design: The study design consists of a scoping review due to the need to synthesize the available scientific evidence in a rigorous, transparent, reliable, and effective manner [24, 25, 26]. This scoping review is the precursor to a systematic review on psychosocial risk factors associated with GDM, which have been little studied in Latin America and for which a more precise definition is also lacking. The study is aimed at the identification and description of characteristics, key concepts, knowledge gaps and evidence of practice in the field, and at making a map of evidence, characteristics, concepts, and the available knowledge that provides a general and broad vision of the theme. The protocol and checklist were established and defined the inclusion and exclusion criteria in accordance with the JBI and the PRISMA ScR [24, 25, 26, 27, 28].
Inclusion criteria: Studies on pregnant women over 18 years of age diagnosed with GDM according to different criteria, with previous or ongoing GDM diagnosis, without pre- existing diabetes, from 2010 to 2020, in English and Spanish. All types of published primary studies with full text available were included.
Exclusion criteria: Studies on pregnant women under 18 years of age, diagnosed with diabetes before pregnancy. Studies published before 2010.
Information sources: A search was carried out with PubMed / Medline and Cochrane databases to identify scientific articles on this topic, after an analysis of the words contained in the titles and abstracts and the index terms used to describe these articles (MesH and DesC). This supported the development of a search strategy, including identified keywords and index terms. The descriptors and keywords used with the AND and OR boolean connectors are described in Table 1.
Study selection and data extraction: Search results were uploaded and processed using Microsoft Excel version 2016. Two review authors independently screened the titles and abstracts of the search results and then assessed the eligibility of the selected full-text reports. Disagreements were resolved by discussion, consensus, or consultation with a third reviewer when necessary. A standardized extraction form was developed and tested on a sample of 5 articles to assess its completeness and applicability and modified as necessary to ensure that all data was collected to address the research question. The form included first author, type of study, country, participants, main measurements and instruments, results, and findings.
Data analysis: An analysis of the scope, nature and distribution of the studies included in the review and a content analysis of the collected data were made; the literature was summarized according to the psychosocial risk factors found, and the results of the studies were classified into categories and subcategories, when necessary, with the aim of mapping the research landscape in this area. Qualitative results were reported, and we sought to explore similarities and differences between studies, to identify patterns and themes, and postulate explanations for the findings.
Assessment of the quality and risk of bias of the studies: As this was a scoping review, an assessment of the methodological quality of the included studies was not required and there was no evaluation of the risk of bias in accordance with the methodology used [24, 25, 26, 29].
Ethical considerations: As this was a scoping review, there were no people involved in the study: therefore, informed consent was not necessary.
| Item | Descriptor (DeCS) | No. Of studies |
|---|---|---|
| 1 | Psychosocial factors | |
| 2 | Psychosocial risk factors | |
| 3 | Depression | |
| 4 | Anxiety | |
| 5 | Psychological stress | |
| 6 | Gestational Diabetes OR GDM | |
| 7 | 1 AND 6 | 700 |
| 8 | 2 AND 6 | 60 |
| 9 | 3 AND 6 | 200 |
| 10 | 4 AND 6 | 88 |
| 11 | 5 AND 6 | 36 |
| 12 | Lifestyle | |
| 13 | 1 AND 6 AND 12 | 104 |
| TOTAL | 1188 | |
| Complete electronic search strategy for PubMed / Medline Limiters and filters: January 2010 to October 2020, in academic journals (peer-reviewed), English and Spanish languages. |
Table 1: Database search strategy.
Source: Own elaboration, 2021. Table 1: Database search strategy.
Results
The database search yielded 1,188 articles and 52 additional references were found by manual gray literature search and reference list verification, yielding 1,240 scientific evidence. After eliminating duplicates and excluding articles by title, a total of 985 of them were reached, and titles and abstracts were read to verify compliance with the inclusion criteria, after which 699 articles were excluded.
Of these, a total of 286 articles were selected with the option of reading the full text, and 196 that did not meet the inclusion requirements and did not meet the objectives were excluded. The systematic reviews included (n = 11) were taken into account to verify the reference lists and for the conceptualization and operationalization of the psychosocial risk factors associated with GDM. Definitive studies (n = 90) underwent data extraction, processing, and analysis. The document selection process is presented in the PRISMA flow diagram (2009), as shown in Figure 1.
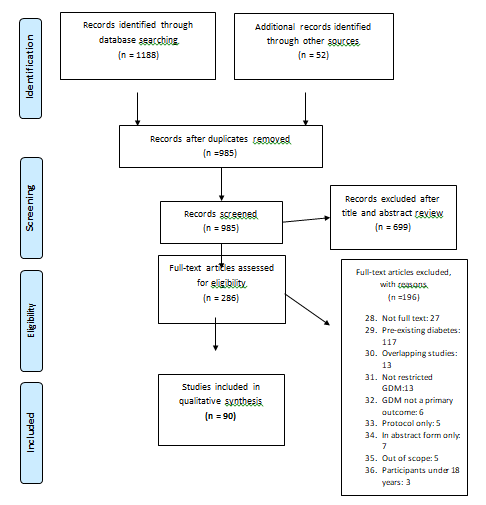
Source: Flow diagram PRISMA (2009). Figure 1: Flow Diagram - PRISMA 2009.
Characteristics of the Included Studies
Of the 90 included studies, 29 had a cross-sectional design, 25 a qualitative design, 19 were cohort studies (16 prospective and 3 retrospective), 11 were systematic reviews and 5 meta-analyses, 4 were case-control studies, 3 were mixed studies (qualitative and quantitative) and 1 was Controlled Clinical Trial (Table 2).
| Item | First author, Year | Type of study | Country | Population/sample | Measurements/Instruments |
|---|---|---|---|---|---|
| 1 | Abraham K, et al. [30] | qualitative study | New York, United States | 10 women with GDM in the last 5 years. | Short semi-structured interviews |
| 2 | Arafa A, et al. [31] | systematic review and meta-analysis | 10 studies | Search in databases of cohort studies on GDM and risk of postpartum depressive symptoms | |
| 3 | Arafa A, et al. [32] | meta-analysis of cohort studies | United States / Australia | 5 studies | Search in databases of cohort studies on depression and risk of gestational diabetes |
systematic review and meta-analysis
4 Azami M, et al. [33]
18 studies
5 Berggren EK, et al. [34] retrospective cohort study North Carolina, United States 1018 women with GDM
6 Bouthoorn SH, et al. [35] cohort study Rotterdam, the Netherlands 7511 pregnant women
7 Burgut FT, et al. [36] cross-sectional study Qatar 1379 postpartum women
8 Carolan M, et al. [37] cross-sectional study Melbourne, Australia 143 women with GDM Attitude towards diabetes scale
9 Carolan M, [38] qualitative study Melbourne, Australia 15 women with GDM Semi-structured interviews and focus group
10 Carolan M, et al. [39] qualitative study United States / Australia 18 women with GDM Interviews
11 Carolan M, et al. [40] cohort study Melbourne, Australia 140 women with GDM Diabetes Knowledge Scale [DKN] questionnaire, with additional questions about pregnancy and GDM
12 Chávez- Courtois M, [41]
13 Clark CE, et al. [42] Cases and controls study California, United States 384 with DMG; 382 without DMG
14 Clevesy MA, et al. [43] study of case United States 1 woman with GDM
15 Colicchia LC, et al. [44] cross-sectional study United States 111 women with GDM
16 Cosson E, et al. [45] cross-sectional study París, France 994 women with GDM
17 Dahlen HG, et al. [46] retrospective cohort study Sidney, Australia 3092 pregnant women Edinburgh Depression Scale, EPDS; risk factor screening tool Search for studies in Scopus, PubMed, Science Direct, Embase, Web of Science, CINAHL, Cochrane Library, EBSCO, and Google databases Perinatal results comparing Hispanic and African American women with Caucasian women.
Education was classified into four levels. The diagnosis of GDM was retrieved from the birth records.
Edinburgh Postpartum Depression Scale (EPDS) and structured questionnaire qualitative study Ciudad de México, México 30 women with GDM Michigan Diabetes Research and Training Center questionnaire and in-depth interviews.
Fasting serum glucose, 75 g oral glucose tolerance test (OGTT) or 100 g OGTT during pregnancy; Diagnosis of depression in the 6 months after delivery Edinburgh EDPS Depression Scale. Diagnosis GDM at 28 weeks of gestation, with oral glucose tolerance 2 hours later.
Diabetes Social Support Scale, Confusion, Fuss and Order Scale, Survey on Access to Healthy Food and Physical and Emotional Responses to Food Precariousness and Inequality Scale in Health Centers (EPICES). Main complications of GDM (large- for-gestational age infant (LGA), shoulder dystocia, caesarean section, pre-eclampsia).
18 Damé P, et al. [47] cross-sectional study Brasil 820 women with GDM Edinburgh EPDS Depression Scale and Structured Interviews risk factor screening tool
19 Devsam BU, et al. [48] systematic review 19 studies Analysis of the beliefs, values, perceptions, and experiences of women after the diagnosis of GDM.
20 Doughty KN, et al. [49] prospective cohort study
21 Draffin CR, et al. [50] qualitative study United Kingdom 19 women with previous or current GDM Focus groups
22 Eades CE, et al. [51] qualitative study Scotland 16 women with GDM Semi-structured interviews
23 Egan AM, et al. [52] prospective cohort study
24 Engberg E, et al. [53] cross-sectional study
25 Figueroa-Gray M, et al. [54] qualitative study Seattle, United States 16 women with GDM Focus groups
26 Garcia-Soidan FJ, et al. [55] qualitative study Valencia, Venezuela 39 women with previous GDM Beck’s Depression and Hamilton Anxiety Interview and Test.
27 Ge L, et al. [56] qualitative study Southeast China
28 Gilbert L, et al. [6] systematic review 16 studies Search in article databases between 1980 and 2018
29 Goldstein R, et al. [57] cross-sectional study Melbourne, Australia 46 women with GDM Satisfaction questionnaire with the diagnosis, risk perceptions and health beliefs
30 Hayase M, et al. [58] cross-sectional study Japan 56 women with GDM Pittsburgh Sleep Quality Questionnaire (PSQI) and Perceived Stress Scale (PSS).
31 Hjelm K, et al. [59] qualitative study Sweden 14 women with GDM Semi-structured interviews
32 Hjelm K, et al. [60] qualitative study Sweden 9 women with GDM Semi-structured interviews during pregnancy (weeks 34-38), and 3 and 14 months after delivery
195 pregnant women with GDM and 2815 without GDM
Multivariate logistics and regression to estimate associations between GDM and dependent variables.
Pregnancy Experience Scale (PES), Stress, Anxiety and Depression Scale (DASS), Perceived Social Support Scale (PSSS), Health Survey (SF) -822, Brief Disease Perception Questionnaire (IPQ), Questionnaire areas Problem Diabetes (PAID-5), Diabetes Self-Efficacy Scale (DSES)
218 pregnant women with GDM and 108 without GDM
482 pregnant women with GDM, BMI ≥ 30 kg / m2 and 358 pregnant women without GDM
Edinburgh Depression Scale EPDS
62 women with GDM without other pregnancy complications In-depth interviews
33 Horsch A, et al. [61] cross-sectional study Switzerland 203 women with GDM
34 Hui AL, et al. [62] qualitative study Pittsburgh, United States 30 women with GDM
35 Hussain Z, et al. [63] cross-sectional study Pulau Pinang, Malaysia 166 women with GDM
36 Ilias I, et al. [64] cross-sectional study Athens, Greece 56 women with GDM
37 Jarvie R, et al. [65] qualitative study Southwest England
38 Jelsma JG, et al. [66] mixed study 7 European countries 92 overweight pregnant women Interviews and questionnaire, (BMI ≥ 25 kg / m2)
39 Kaiser B, et al. [67] prospective cohort study Geneva, Switzerland 173 pregnant women with GDM
40 Kaptein S, et al. [68] qualitative study Toronto, United States 19 women with GDM Semi-structured interviews
41 Keskin FE, et al. [69] cross-sectional study Istanbul, Turkey 44 women with GDM and 45 without GDM
42 Kim Y, et al. [70] cross-sectional study Bangladesh 358 pregnant women
43 Knippen KL, et al. [71] cross-sectional study United States 205 women with previous GDM
44 Kopec JA, et al. [72] cohort study Szczecin, Poland 205 women with GDM Examen físico, Cuestionario a las 27 semanas de gestación y a las 36 semanas de seguimiento.
Questionnaire events related and unrelated to pregnancy, perceived stress, psychological distress, anxiety, depression and amount of sleep. Cortisol was measured using fasting and bedtime saliva samples, and copeptin using fasting plasma.
Semi-structured interview Food Choice, Perceived Stress Scale, Anxiety Scale during Pregnancy, Demographic Questionnaire.
DMG Knowledge Questionnaire (GDMKQ). Mean of 3 Most Recent Fasting Plasma Glucose (FPG) Values (mmol / L) Diagnosis of GDM with HAPO criteria and treated with at least one insulin injection per day and Lay’s procrastination questionnaire
27 women with coexisting BMI ≥ 30 and with GDM
In-depth interviews during pregnancy and postpartum and field notes Quantitative data at the end of pregnancy (T1) and at 6 months postpartum (T3).
Beck’s Depression Inventory (BDI), Montreal Cognitive Assessment (MOCA), Stimulated Auditory Serial Addition Test (PASAT), Spatial Memory Test (SRT), Symbol Digit Modalities (SDMT), and Word List Generation (WLG).
Knowledge about GDM. Health beliefs about GDM. Intention to breastfeed yes or no. Demographic and pregnancy-related characteristics Análisis secundario de los datos de la Encuesta Nacional de Examen de Salud y Nutrición (NHANES) 2007- 2014
45 Kordi M, et al. [73] cross-sectional study Mashhad, Iran 400 women with GDM
46 Kragelund- Nielsen K, et al. [74]
47 Krige SM, et al. [75] cross-sectional study Ciudad del Cabo, South África 239 pregnant women with GDM Questionnaire of frequency and beliefs related to food choices
48 Kubo A, et al. [76] cross-sectional study California, United States 1353 women with GDM
49 Larrabure- Torrealva GT, et al. [77]
cross-sectional study Lima, Perú 1300 pregnant women
50 Lee K, et al. [78] cross-sectional study Malaysia 526 women with GDM Depression, anxiety, and stress questionnaire (DASS-21)
51 Lydon K, et al. [79] cross-sectional study Ireland 25 women with GDM and 25 women without GDM
52 Mak JKL, et al. [80] prospective cohort study Sichuan, China 1449 pregnant women
53 Marchetti D, et al. [81] systematic review 15 studies
54 Martinez- Paredes JF, et al. [82] topic review 55 studies Searching databases of studies on depression in pregnancy
55 McMillan B, et al. [83] qualitative study United Kingdom 27 women with GDM Semi-structured interviews
56 McParlin C, et al. [84] qualitative study United Kingdom 12 pregnant women with GDM
57 Miazgowski T, et al. [85] prospective cohort study Szczecin, Poland 165 women with GDM Secondary analysis of data from the National Health and Nutrition Examination Survey (NHANES) 2007-2014 qualitative study South India 19 pregnant women with GDM Semi-structured interviews Perceived Stress Scale (PSS10) and gestational weight gain according to the 2009 Institute of Medicine Diagnosis of GDM with IADPSG criteria and Patient Health Questionnaire-9 to evaluate depression Pregnancy Experiences Scale (PES), Depression Anxiety and Stress Scale (DASS), Diabetes Problem Areas Scale (PAID-5) and Perceived Social Support Scale (PSSS).
Diagnosis of GDM with oral glucose tolerance tests. Edinburgh Postnatal Depression Scale (EPDS) at 32-37 weeks’ gestation, one month and three months postpartum Search in databases of studies to evaluate and / or improve quality of life levels in women diagnosed with GDM.
1200 kcal / day diet for moderate weight loss (WELLBABE study) and semi-structured interviews after completing the 4-week diet State-Trait Anxiety Inventory (27 and 37 weeks of gestation), Multidimensional HLC scale, Glycemic control by self-monitoring fasting and postprandial blood glucose levels.
| 58 | Molyneaux E, et al. [86] | RCT Randomized Clinical Trial | United Kingdom | 797 obese pregnant women [BMI] ≥30 kg / m2 | Edinburgh depression scale and glucose tolerance test at the beginning of pregnancy and at 28 weeks of gestation. Adherence to at least 5 out of 8 intervention sessions. Gestational weight gain. |
|---|---|---|---|---|---|
| 59 | Momeni JF, et al. [87] | cross-sectional study | Shahid Beheshti, Iran | 100 pregnant women with GDM and 100 without GDM | Lifestyle questionnaire during pregnancy |
| 60 | Morrison C, et al. [88] | cross-sectional study | North Carolina, United States | 1021 pregnant women without pre- existing diabetes | Depression questionnaire and medical records to identify a positive history of diabetes after the first trimester of pregnancy. |
| 61 | Morrison MK, et al. [89] | cross-sectional study | Australia | 393 diagnosed with GDM ≤3 years earlier | Postal Survey |
| 62 | Muche AA, et al. [90] | cohort study | Northwest Ethiopia | 1027 pregnant women | Diagnostico DMG con criterios ADA/ OMS 2013/IADPSG; Cuestionario internacional de actividad física (IPAQ); Medición diversidad dietética; Entrevista. |
| 63 | Muhwava LS, et al. [91] | qualitative study | Ciudad del Cabo, South África | 35 women with GDM | Focus groups and in-depth interviews |
| 64 | Mukerji G, et al. [92] | cross-sectional study | Ontario, Canada | 614 women with GDM | Diabetes risk perception survey |
| 65 | Orbay E, et al. [93] | cross-sectional study | Turkey | 281 pregnant women with or without GDM | DMG diagnosis with glucose tolerance test; Survey and Hospital Anxiety and Depression Scale (HAD) |
| 66 | Pantzartzis KA, et al. [94] | Cases and controls study | Salonica, Greece | 31 pregnant women with GDM and 31 without GDM | Quality of life questionnaires EQ-5D- 5L, WHOQOL-BREF and ADDQoL |
| 67 | Párraga- Moreira GJ, et al. [95] | cross-sectional study | Manabí, Ecuador | 95 pregnant women | Survey, interview and Self-care perception test |
| 68 | Parsons J, et al. [96] | qualitative study | London, United Kingdom | 35 women with GDM | In-depth interviews and focus groups |
| 69 | Parsons J, et al. [97] | qualitative study | United Kingdom | 50 women with GDM in the previous five years | In-depth interviews and focus groups |
| 70 | Persson M, et al. [98] | qualitative study | Sweden | 10 women with GDM | In-depth interviews |
| 71 | Ricardo- Ramírez C, et al. [99] | cross-sectional study | Medellín, Colombia | 189 pregnant women with high obstetric risk | Beck’s Depression Inventories version II (BDI-II) and Beck’s Anxiety and Demographic and Clinical History Questionnaire |
| 72 | Ruiz-González I, et al. [100] | Cases and controls study | Granada, Spain | 46 women with GDM and 84 controls | GDM diagnosis with O ‘Sullivan test, Anthropometric assessment, Sociodemographic questionnaire, gynecological study. Measurement of sleep quality and daytime sleepiness. |
73 Ruohomaki A, et al. [101] cohort study Finland 1066 women with GDM
74 Saadati F, et al. [102] cross-sectional study Tabriz, Iran 364 women with GDM Sociodemographic questionnaire, Pittsburg sleep quality and quality of life during pregnancy QOL-ORAV
75 Sandsaeter HL, et al. [103]
76 Schmidt CB, et al. [104] prospective cohort study Amsterdam, Netherlands 100 women with GDM
77 Siad FM, et al. [105] qualitative study Calgary, Alberta, Canada 10 women with GDM In-depth semi-structured interviews
78 Singh H, et al. [106] mixed study California, United States 564 women with GDM In-depth semi-structured interviews
79 Surucu HA, et al. [107] cross-sectional study Turkey 109 pregnant women with GDM and 109 without GDM
80 Surucu HA, et al. [107] cross-sectional study Turkey 126 women with GDM Demographic and Clinical Data Questionnaire and Stress Coping Scale
81 Sutherland L, et al. [108] cross-sectional study 79 women with GDM Surveys and abstraction of medical records after delivery and 3 months postpartum.
82 Tang Y, et al. [109] prospective cohort study Sichuan, China 1426 pregnant women
83 Trutnovsky G, et al. [110] cohort study Germany
systematic review and metanalysis Africa 17.938 pregnant women
84 Tsakiridis I, et al. [111]
85 Twedt R, et al. [112] prospective cohort study Pittsburgh, United States 37 women with GDM
86 Varela P, et al. [113] cross-sectional study Greece 117 pregnant women Sociodemographic and Obstetric Questionnaire, Edinburgh Postnatal Depression Scale (EPDS)
87 Walmer R, et al. [114] prospective cohort study Massachusetts, United States
Edinburgh Postnatal Depression Scale (EPDS). DMG diagnosis with Finnish guidelines qualitative study Norway 17 women with GDM Interviews and focus group Diabetes scale 5 (PAID-5), Diabetes distress scale (T0-T1), Patient health questionnaire 9 (PHQ-9), self-report and medical records.
GDM diagnosis according to ADA criteria and introductory information form Sociodemographic survey; Anxiety Self-Assessment Scale (SAS); Depression Self-Rating Scale (SDS) WHOQOL-BREF Quality of Life Questionnaire, Mood Questionnaire (MDBF), Diabetes Treatment Satisfaction Questionnaire (DTSQ) and Semi-structured Interview
45 women with GDM, 27 treated with diet and 18 treated with insulin Searches in databases of observational studies between 2007 and 2018.
Sleep record for 7 consecutive days with actigraphy. Association of sleep duration in morning fasting and one-hour postprandial blood glucose concentrations.
659 women with GDM and 14461 without GDM
GDM diagnosis with Carpenter- Coustan criteria and Mental health diagnosis
88 Wilson BL, et al. [115] retrospective cohort study Utah, United States 4682 women with GDM systematic review and metanalysis
89 Wilson CA, et al. [116]
62 studies
90 Xiaoyu W, et al. [117] systematic review 9 studies Search in databases of qualitative studies Bivariate analysis to identify associations between variables and hierarchical stepwise logistic regression to identify the best predictors of GDM and BW.
Search databases for studies measuring GDM and perinatal mental disorder during the same pregnancy
- Source Own elaboration, 2021.
Table 4: Included studies on psychosocial risk factors associated with gestational diabetes.
Most of the investigations were conducted in the United States (n = 16) and the United Kingdom (n = 8); others in Australia (n = 6); n = 4 studies in Turkey, China, and Iran; 3 studies in Sweden, Greece, South Africa and Canada; n = 2 in Switzerland, Malaysia and Poland and 1 study in Qatar, Netherlands, India, Germany, Bangladesh, Netherlands, Norway, Northwest Ethiopia, Spain, Finland, New Zealand, Japan, and France. A multicenter study was conducted in 7 European countries. The Latin American studies were distributed as follows: 4 were carried out in Brazil and 1 in Venezuela, Mexico, Ecuador, Peru, and Colombia.
Of the remaining studies, 11 were systematic reviews and 1 was a meta-analysis. As can be seen, the studies have been carried out in a variety of countries around the world, but most of them exclusively in first world countries. In Latin America there are still very few publications on the subject.
It is important to bear in mind that most of the studies from developed countries focused on the psychosocial risk factors associated with GDM in vulnerable groups, immigrant populations or specific ethnic groups, which could be related to the fact that these types of groups present characteristics such as obesity, low level of education and financial difficulties that act as risk factors for developing GDM [118] (Table 2).
Categories and Subcategories Found of Psychosocial Risk Factors Associated with GDM
Several categories of psychosocial risk factors that influence prevention, health promotion, quality of life, and adherence to treatment of women with GDM were identified. Some of the categories found overlapped within the same study and others resulted in subcategories. The categories were 10 in total, are described in Table 3 with their subcategories and are explained in detail later.
| Item | Categories and subcategories | Total number of studies in the category | Percentage |
|---|---|---|---|
| 1 | Sociodemographic factors: such as socioeconomic factors, conflicts with cultural practices, social stigma, ethnic and racial factors, coordination of treatment with working life, low educational level. | 49/90 | 54,44% |
| 2 | Clinical and obstetric history: such as loss of previous pregnancies, not wanting pregnancy, quality of sleep, physical limitations such as fatigue and exhaustion, problems with breastfeeding, impaired cognitive functions, low quality of life. | 42/90 | 46,66% |
| 3 | Impact of diagnosis: causing shock or shock, burden of facing a diagnosis of GDM, diagnosis that threatens pregnancy, concern for maternal or baby health | 40/90 | 44,44% |
| 4 | Risk perception: as a low perception of the risk of GDM or of developing DM2 in the future after pregnancy | 26/90 | 28,88% |
| 5 | Stress, anxiety, and depression, in addition to a feeling of abandonment | 87/90 | 96,67% |
Table 5: Description of the psychosocial factors associated with GDM.
| 6 | Knowledge about GDM: such as low literacy and limited knowledge about health, GDM or developing DM2 in the future | 25/90 | 27,77% |
|---|---|---|---|
| 7 | Partner / family / social support | 35/90 | 38,88% |
| 8 | Self-care and self-efficacy for glycemic control: such as difficulties for gly- cemic control, deficiencies in self-care and self-efficacy, little motivation to change one’s own lifestyle, high costs for the mother’s autonomy, and time limitations | 43/90 | 47,77% |
| 9 | Support from health professionals: such as the lack of support from health professionals and understanding GDM through living with other women diagnosed with GDM | 29/90 | 32,22% |
| 10 | Lifestyle changes: there are difficulties in changing lifestyle, not considering biopsychosocial well-being and practical and flexible solutions for pregnant women with GDM | 28/90 | 31,11% |
Table 6: Description of the psychosocial factors associated with GDM.
GDM: gestational diabetes mellitus; DM2: type 2 diabetes mellitus. The total number of psychosocial risk factors is associated with the number of studies identified that mention these factors. Source: Own elaboration, 2021. Table 3: Description of the psychosocial factors associated with GDM.
The results indicate that sociodemographic factors such as financial limitations [39, 105, 111, 115] result in difficulty paying treatment costs, buying expensive meals, paying medical bills, and obtaining resources for the development of healthy eating habits [67, 74]. Some women with GDM do not have the means and resources in the postpartum period to apply in a lasting way the advice received in the prenatal period.
Cultural norms can act as risk factors for developing GDM. For example, the lack of information on traditional and alternative food, appetite regulation, cultural roles and beliefs, social stigmas, and the almost total absence of social and professional support about diet and physical activity, can become cultural barriers that work against adherence to treatment [48, 68, 97].
Women with GDM are socially stigmatized due to the lack of information and health literacy of the general population [65]; they experience stress due to social and economic causes as they are stigmatized for being obese during pregnancy and for not promoting changes in their lifestyle. They feel socially punished if they do not comply with the necessary behaviors to achieve a healthy lifestyle.
Regarding ethnic and racial factors, in some studies it was found that not having a European origin, being migrants, being non-white (non-Caucasian) women are conditions that influence the relationship between GDM and symptoms of anxiety and depression. Hispanic women had fewer adverse outcomes overall compared to Caucasian or African American women.
Treatment to achieve glycemic control and reduce adverse GDM outcomes may differ by race / ethnicity women of non-Caucasian ethnicities may be at risk of poorer gestational diabetes self-management due to less education, lower health literacy and lower valuation of GDM as a serious disease. In the United States, during a study of 205 women with a history of GDM, it was found that Hispanic women and non-Hispanic black women were less likely to have had glucose tests than non-Hispanic white women, which could increase the risk of developing DM2 after delivery.
Some of the challenges faced by women with GDM who work are coordinating treatment with working life, having to resolve schedule difficulties and other burdens such as childcare and other home tasks while the work demands and the treatment to control GDM is necessary.
Low educational level is the sociodemographic element that was most associated with a psychosocial risk factor because it generates a poorer appreciation of GDM and low glucose control. In the cohort study of 7511 women with GDM by Bouthoorn SH, et al. [35] it was found that women with the lowest level of education were 3 times more likely to develop GDM than women with the highest level of education. Other sociodemographic factors are type of work occupation, consanguinity, lack of access to transport, women with age ranges up to 25 years, unemployment status, sexual abuse and domestic violence.
Clinical and obstetric antecedents such as unplanned pregnancies, threatened abortions, cesarean section, diagnosis of GDM in a previous pregnancy and weight gain, can act as factors of psychosocial risk associated with GDM. In a study carried out in Lima, Peru, with 1,300 women with GDM, it was found that a family with history of diabetes is 1.5
times more likely to develop GDM
Multiparity, interrupted pregnancies, overweight and obesity, pregnancy at an early age, pregnancy at an advanced age, history of mental health problems and excessive gestational weight gain, were found to be some of the psychosocial risk factors associated with GDM.
The deterioration of sleep quality and sleeping difficulties also act as psychosocial risk factors associated with GDM. In different studies it was observed that diabetic pregnant women have a daytime sleepiness higher than the average population. Short durations of sleep at night were associated with very poor glucose control in women with GDM. Duration of sleep was negatively associated with postprandial fasting blood glucose concentrations, and an increase of one hour in sleep time was associated with statistically significant reductions in fasting glucose and postprandial glucose concentrations.
Certain physical limitations such as tiredness, physical discomfort, hunger, thirst, diuresis, and fatigue were associated with psychosocial risk factors because these variables act against the desire to change diet or be physically active. Therefore, they affect adherence to treatment of women with GDM.
After a diagnosis of GDM, the probability of breastfeeding decreases (ORa = 0.62, 95% CI 0.46, 0.85) and there is a preference for feeding the baby with formula (ORa = 1.74, 95% CI 1.02, 2.97) or mixed feeding (ORa = 1.78, 95% CI 1.21, 2.61). Breastfeeding initiation rates are lower and there is a higher risk of early interruption of breastfeeding in women with obesity compared to women with a healthy weight. Perceived susceptibility, benefit and self-efficacy were identified as significant factors in increasing the intention to breastfeed in women with GDM.
Some women diagnosed with GDM have a decreased quality of life, which can affect adherence to treatment. Several emotional alterations originated by the impact of the GDM diagnosis were found, such as the feeling of shock, disappointment [106], helplessness, worry [117] and struggle to accept treatment, in addition to feelings of “loss of control”.
Another group of women experienced that it is temporary but that they cannot face the diagnosis alone [30] because they experience strong emotions, negative thoughts and uncertainty at the time of diagnosis [48, 50]. On the other hand, it was found that some women do not consider GDM an important or real diagnosis and believe that its impact is minimal [51].
After the diagnosis of GDM, women’s concerns revolve around its acceptance and their energies are focused on how to solve it and face it with new strategies such as changes in lifestyle, and a struggle ensues to know how to handle GDM, many times feeling a great burden. Authors such as Persson M, et al. [98] and Jarvie R, et al. [68] reported that the main concern of women diagnosed with GDM is the perception that this complication threatens their pregnancy, their health and that of the baby: factors that can also be protective and not only risky because they induce to improve one’s health and reduce any future risk of diabetes.
Women prioritize the health of the baby, but in many cases this could lead them to adopt extreme behaviors such as starvation, and this could also put the health of the fetus at risk. Concern about the health of the child constitutes a favorable factor (and not only a risk factor) since for these women the greatest motivation for long-term changes in their lifestyle is the future health of the.
In general, there is an awareness that GDM is a low risk disease and not a serious one. Many times, women do not even believe in the diagnosis. Therefore, it is necessary to create greater awareness about the risks of GDM, as some women may not comply with the advice of professionals regarding lifestyle changes and necessary glycemic control and pay urgent attention to the serious consequences of the lack of adherence to treatment.
Women expressed concern about the risk of developing DM2 in the future, that is, after delivery: a perception that can be reinforced by the lack of post-pregnancy care, considering GDM a transitory condition. The absence of a history of prior GDM, a family history of diabetes, and insulin use were associated with a low perception of the risk of diabetes in the future [92].
Perception of stress, negative thoughts after diagnosis and doubts about how to deal effectively with stress are psychosocial risk factors for GDM, so it is necessary to develop effective stress coping strategies, such as optimistic coping because it is related to adequate glycemic control. Women with increased stress from early to mid-pregnancy were 2.6 times more likely to having developed GDM.
Likewise, it was found that women who received insulin experienced significantly higher levels of stress and anxiety, which may lead to the emergence of unhealthy dietary coping strategies. Unemployment and a second pregnancy were important factors in women with GDM who coped ineffectively with stress. In Jarvie’s R, et al. [65] qualitative study, women experienced a number of social and economic stressors that compromised their ability to manage pregnancies complicated by maternal obesity and GDM and to make changes in lifestyle.
In several studies it was found that women experience feelings of fear, skepticism, uncertainty, suffering, disappointment, sadness, and miserableness when receiving and living with a diagnosis of GDM. In addition, they feel distressed about changes in their identity, thus increasing the risk of developing GDM. At the beginning of pregnancy, severe anxiety was more prevalent in hyperglycemic women than in those with a normal glycemic status and, in addition, some women presented a possible intention to injure themselves [93].
Tan’s prospective cohort study with 1426 women showed that the risk of GDM in anxious pregnant women was higher than that of non-anxious pregnant women (OR = 1.556, 95% CI 1.014- 2. 387). In this study, it was also recorded that there is an association between diabetes distress, parity, and adverse pregnancy outcomes: the prevalence of anxiety and depression was higher in the group of nulliparous women (8.8% and 11.9%) than in the one of multiparous women (5.4% and 6.4%) and the difference was statistically significant (P <0.05).
On the other hand, insulin treatment causes fear and a feeling of “shock” and was associated with anxiety caused by a lack of knowledge about GDM and family encouragement and a feeling of not receiving enough support from health care providers. The levels of anxiety, impotence and worry increase in these women due to the apprehension they feel about the health of the baby and the possibility of developing maternal and infant complications. Furthermore, distress negatively affects quality of life and there may be a complex interaction between psychosocial anxiety and gestational weight gain among women with GDM [76].
Similarly, several studies have confirmed an association between depression and GDM. In fact, women with GDM had higher EDPS (Edinburgh Depression Scale) scores compared to women without GDM. It was found that the disease of women with GDM who had completed the EDPS, was associated with a higher probability of depression (OR 2.23, 95% CI 1.23-4.05, Ruohomaki, 2018), (pooled OR = 1, 20; 95% CI: 1.09, 1.33, [31]), confirming that women with a history of depression compared to those without it have a significantly higher risk of developing GDM.
In addition, it was found that there is a higher risk of depressive symptoms in the prenatal period and around the time of the GDM diagnosis, and there seems to be an association between a result in the EPDS ≥ 13 and other psychosocial problems, such as thoughts of self-harm, domestic violence, and child abuse.
In contrast, elevated symptoms of prenatal depression did not predict GDM (adjusted OR 0.80, 95% CI 0.52 to 1.22, P = 0.30), adherence to treatment (adjusted OR 1.16; 95% CI: 0.63 to 2.15; p = 0.63) or increase in gestational weight OR adjusted 0.52, 95% CI: -0.26 to 1.29, p = 0.19), in the Molyneaux Randomized Clinical Trial RCT with 797 obese pregnant women with GDM.
Family history of depression and anxiety, age up to 25 years, psychological abuse, having a dysfunctional partner, having children under five years of age, having been a victim of adverse social situations or having lived through a natural disaster are factors that are associated with depression, and having depression was associated with an increased chance of developing GDM.
It was found that the feeling of abandonment may be present especially in the postpartum period, as women felt abandoned after delivery and were not sure what to expect from their GP in terms of monitoring and support. Likewise, a clear gap between the knowledge and behavior of women with GDM and a lack of knowledge about the necessary lifestyle modifications became present.
Educational level seems to be the most significant indicator of the level of knowledge of GDM: the lower the educational level, the more limited the knowledge about GDM. But women are convinced that together with their partner they can have a joint and more adequate understanding of the need for changes in their lifestyle.
Women present a serious lack of literacy in health, GDM, possible DM2 in the future, the values of beneficial foods and an adequate physical activity routine. When women have GDM, a supportive family and social environment is necessary to manage this condition, which requires changes in one’s own lifestyle.
The partner, friends and family are a source of social support [37, 44, 66, 84, 89, 111] and it was found that the greater the social support, the greater the adherence to treatment. In addition, women with GDM have the perception that they are victims of social stigma due to obesity and GDM, suffering from social problems and feeling interference with their family life. Research shows that the partner is seen as a motivator, that is, it becomes a long-term contributor to changes in lifestyle.
For women with GDM, it is essential to recognize the necessary changes and learn to manage GDM. When they fail to carry out these changes, they present feelings of “loss of control” [62] which leads to poor glycemic control and perinatal complications. It is important to keep in mind that not having a blood glucose test in the last three years is a risk factor if one has or has had GDM.
There are barriers to achieving an effective self-care of GDM that have to do with diet, physical activity, sleep, rest, and social interaction, consequences of procrastination and disobedience: two-character traits that have already been shown to be linked to non-compliance with diabetes treatments. Those women who perceived their risk as higher or felt supported by family or friends were more likely to report a high level of agreement (glycemic control) with GDM treatment associated with an internal locus of control.
The main motivation of women to change their lifestyle is the concern for the health of the baby during pregnancy and after birth, but the multiple demands of time and activities of a GDM treatment give women the impression that the costs of their personal autonomy are high, facing competitive demands of time and a great pressure to fulfill multiple activities.
Women with GDM need the support of health professionals, who should be attentive to their own beliefs about this condition, since these influence the beliefs and behaviors of patients. Likewise, women feel a need for more individualized and culturally appropriate advice, particularly on diet.
Frequent references to weight change by health professionals were considered stigmatizing and counterproductive, making them feel judged for being obese or having GDM and perceive their recommendations as unrealistic given their limited social / material circumstances. Findings indicate that the health care personnel did not convey to them the future implications of DM2 and the need for follow-up glucose testing after delivery. Health care would be aimed at only recording information and the consultation time is not enough to develop knowledge about GDM and adequately cover their needs.
Women perceive lifestyle changes as problematic, there are suboptimal levels of fruit and vegetable consumption and physical activity and they experience that abstaining from eating a snack becomes a challenge due to their beliefs.
Controlling cravings for sugary foods and beverages is an important topic to target for lifestyle change messages, because bad eating habits (more sugar and less fiber) can contribute to poor adherence to nutritional guidelines among pregnant women with GDM, worsening their quality of life both in the short and long term.
Last but not least, it was found that many of the interventions for women with GDM include programs on diet and physical activity, but do not integrate biopsychosocial well-being, which would help to reduce the perception of stress. With the multiple activities and commitments to home and work, women prefer practical and flexible solutions that are perceived as a motivator and a favorable factor for changes in lifestyle.
Discussion
The objective of this study was to conduct a comprehensive review of the psychosocial risk factors associated with gestational diabetes mellitus in order to improve intervention and prevention programs for this condition.
Ten psychosocial risk factors associated with GDM were identified, categorized, and described in the 90 studies included in this review. The most common psychosocial risk factors are stress, anxiety, and depression (87/90, 96.77%), which are treated directly or indirectly. These factors must be considered throughout the cycle of comprehensive health care for pregnant women with GDM, if the desire is to improve short and long-term results for mothers and their children.
Depression is presented as a risk factor for developing GDM, so it is necessary to take preventive measures and ensure early detection. There appears to be an association between an EPDS> or = 13 and developing GDM for which further investigation is warranted. The application of the Edinburgh Depression Scale EPDS is recommended as a tool (validated worldwide), especially after the diagnosis of GDM and during the perinatal period. Early diagnosis favors a decrease in risk behaviors, fetal neurodevelopmental disorders, and obstetric outcomes, since the consequences associated with depression include interference with the mother-child bond.
Many of the psychosocial risk factors found in this review coincide with those proposed by Gómez López ME, et al. [119] among which there are socioeconomic factors such as employment, poverty, domestic work, education, and income; psychological factors such as life events, social isolation, stress due to conflicts with partner, negative life events, dissatisfaction with regard to pregnancy, social support from the partner, friends, and family.
Gómez López ME, et al. [19] states that psychosocial risk factors can range from having living children or not to having had gestational losses or not, to having family and / or partner support or not, to planning pregnancy or not and to having had obstetric complications or not. In the study carried out at the “Isidro Espinosa de los Reyes” National Institute of Perinatology, it was detected that the main emotional risk factors included being an obstetric patient, having one or more living children, not having a partner, dedicating oneself to the home, being a merchant or unemployed, being over 35 years old and having a scholarship of zero to nine years.
On his part, Pimentel D, et al. [120] states that the factors associated with emotional alterations that cause psychological distress during pregnancy with endocrinopathy include the experience of the disease, an unhealthy lifestyle, social stressors, depressed mood, unplanned pregnancy, and personal beliefs about the disease. Therefore, the emotional problems of women with high-risk pregnancies include ambivalence or rejection towards pregnancy, guilt for being responsible for pregnancy complications, social inadequacy, heightened anxiety levels and depression resulting from a complex interaction of physical variables, genetic and psychological, which may precede GDM or result from it, as found in this review.
For these women to implement changes in their lifestyle, early, adequate, appropriate, reliable and high-quality information is necessary, in an easy-to-use and consult format and with flexible intervention proposals that offer practical solutions and include motivational and supportive factors such as the baby’s health and partner and family participation.
Knowledge of the experiences of women diagnosed with GDM can be useful to health professionals to provide greater and better support and preventive measures for glycemic control. According to different authors, this could delay the development of DM2 in the future. In other words, greater knowledge about GDM is related to better glycemic control and consequent adherence to treatment.
Successively, it is advisable to be attentive to the stigmatizing beliefs and attitudes of health professionals, since these can influence the beliefs of patients and make them suffer emotionally. It is necessary to give personalized attention to the necessary modifications in lifestyle and guidelines on how to help control weight, considering the barriers experienced by some overweight or obese mothers. Therefore, more awareness and training programs aimed at health personnel are recommended.
On the other hand, it is necessary to evaluate the capacity for self-care and self-efficacy of women with GDM and develop group and participatory activities considering that living with women in similar conditions helps to motivate them to generate changes in lifestyle and to increase the internal locus of control that helps to promote greater responsibility and a higher level of commitment among them. Psychosocial well-being is as important in interventions as recommendations on diet and physical activity It is recommended that interventions include addressing the stress and anxiety of pregnancy and the diagnosis of GDM with effective coping strategies, transmitting risk proactively and motivating women with GDM to change their lifestyles, with an approach focused on the couple, the family, the woman’s environment and her health, since if the pregnant woman has quality of life this will be reflected in the fetus and the newborn.
Knowledge about GDM has an impact on quality of life that goes beyond pregnancy. The lack of information about GDM (such as information about insulin and its impact on daily life and causes and risks of GDM), diet and follow-ups lead to a lower perception of risk and poor self-care behavior, in addition to increased A1C and weight gain. Therefore, interventions should not end with pregnancy considering the risk of developing DM2 after delivery.
It is important to consider multi-ethnic populations and the most demographically and socioeconomically vulnerable groups while developing educational programs that address their needs. Among the findings of this review are significant ethnic differences that make some women culturally sensitive to dietary recommendations. Sociocultural determinants should be the basis for designing and implementing the different nutritional treatment and physical activity strategies.
In rural communities where there are fewer resources available, context-specific support strategies should be developed. People with a low level of education are more likely to develop GDM because among them there are higher rates of overweight and obesity and intervention strategies should focus on reducing overweight and obesity before pregnancy.
The findings show that the quality of sleep is low among women with high-risk pregnancy, so it is necessary to educate them about healthy sleep, which is associated with adequate control of blood glucose.
There seems to be a relationship between risk perception and social support, and, in turn, these factors seem to be closely related to compliance with recommendations and adherence to GDM treatment. There is also a significant relationship between quality of life and attendance at a diabetes education program.
At the Latin American level, we found a single person that can be considered a reference point in this topic and has proposed several guidelines on psychosocial risk factors associated with obstetric complications and in high-risk pregnancies. The other Latin American go-to researcher comes from Argentina with an article on the importance of considering psychosocial risk factors in DM2.
Conclusion and Recommendations
Community interventions are recommended to raise awareness about healthy lifestyles and include training for pregnant women on the complications that can be developed during pregnancy due to modifiable factors such as overweight and obesity, sedentary lifestyle, consumption of psychoactive substances and not modifiable factors such as personal and family pathological antecedents. For example, technology can be seen as an alternative or complement to intervention, providing information, allowing flexible and personalized self-management, and facilitating social support. The need for future research was identified to test the efficacy of using technology as an adjunct to current care.
Important aspects such as partner, family, social support, and health professionals need to be taken into account for women with GDM to be able to finally act the necessary changes in lifestyle to improve their quality of life and combat many of the adverse outcomes of GDM. These are sufficient grounds for including psychosocial risk factors in future guidelines, so we conclude this article by strongly recommending that psychosocial risk factors be included in clinical practice guidelines and that research on this topic be promoted.
Limitations and strengths: The main strength of this review is that it is an initiative to ensure that care in health services is comprehensive and interdisciplinary. Recommendations emerged for clinical practice in the psychosocial area of GDM that, if not cared for, could be the cause of the failure of prevention, promotion, and intervention programs for women with GDM and lack of adherence to treatment. The publication date of the included studies was limited to the last decade considering that scientific production on this topic has been generated only in recent years. The diversity and richness of the data collected would justify some analysis by complementary topics that it is suggested to carry out in the near future, in order to include and develop this area in the production of future Clinical Practice Guidelines for GDM.
Implications for practice: Several psychosocial risk factors were identified and categorized that should be taken into account in the future development of CPG and in prevention, promotion and intervention programs for the health and quality of life of women with GDM.
- Authors’ Contribution: Conceptualización y diseño, S.C.M.M., J.C.M.E, A.M., H.M.C., C.R.R .; Methodology, S.C.M.M., J.C.M.E, A.M., M.E.G.L .; Data acquisition and Software, L.M.A.P., V.P .; Analysis and interpretation of data, S.C.M.M., J.C.M.E, A.M., L.M.A.P., V.P .; ; Investigador Principal, S.C.M.M., Investigación, S.C.M.M., J.C.M.E, A.M., L.M.A.P., V.P., M.E.G.L., J.C.M.R. Drafting of the manuscript— Preparation of the original draft, S.C.M.M., J.C.M.E, M.E.G.L .; Drafting, revision and editing of the manuscript, S.C.M.M., J.C.M.E, A.M., C.R.R., H.M.C., L.M.A.P., V.P., M.E.G.L., J.C.M.R. Visualización, S.C.M.M., J.C.M.E .; Supervisión, S.C.M.M., J.C.M.E .; Acquisition of funds, M., J.C.M.E, A.M., L.M.A.P., V.P., M.E.G.L., J.C.M.R. Visualización, S.C.M.M., J.C.M.E .; Supervisión, S.C.M.M., J.C.M.E.
- Acknowledgments: We present our thanks to the GDM Project, Vida Nueva WDF10-572: Improving detection and treatment of GDM and reducing the future risk of diabetes in the mother and offspring in Barranquilla City.
- Conflict of Interest: The authors have no conflict of interest.
References
-
(2016) Organización Mundial de la Salud OMS. Informe Mundial sobre la Diabetes.
-
Diabetes. Organización Panamericana de la Salud OPS.
-
American Diabetes Association ADA (2020) Standards of medical care in diabetes. Diabetes Care 43(S1): S1-S2.
-
International Diabetes Federation (2015) Atlas de la Diabetes de la FID. In: 7th (Edn.), pp: 1-144.
-
Coustan DR, Lowe LP, Metzger BE, Dyer AR (2010) The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study: paving the way for new diagnostic criteria for gestational diabetes mellitus. Am J Obstet Gynecol 202(6): 654.e1-654.e6546.
-
Gilbert L, Gross J, Lanzi S (2019) How diet, physical activity and psychosocial well-being interact in women with gestational diabetes mellitus: an integrative review. BMC Pregnancy Childbirth 19: 60.
-
Craig L, Sims R, Glasziou P (2020) Women’s experiences of a diagnosis of gestational diabetes mellitus: a systematic review. BMC Pregnancy Childbirth 20: 76.
-
Ali MK, Siegel KR, Chandrasekar E (2017) Diabetes: An Update on the Pandemic and Potential Solutions. In: Prabhakaran D, Anand S, Gaziano TA, et al. (Eds.), Cardiovascular, Respiratory, and Related Disorders. 3rd (Edn.), Chapter 12.
-
Young Hyman D, Hill Briggs F, Gonzalez JS, Peyrot M (2016) Psychosocial Care for People with Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 39(12): 2126-2140.
-
Hackett RA, Steptoe A (2016) Psychosocial Factors in Diabetes and Cardiovascular Risk. Current cardiology reports 18(10): 95.
-
Demakakos P, Zaninotto P, Nouwen A (2014) Is the association between depressive symptoms and glucose metabolism bidirectional? Evidence from the English Longitudinal Study of Ageing. Psychosom Med 76: 555- 561.
-
Pan A, Lucas M, Sun Q, Van Dam RM, Franco OH, Manson JE, et al. (2010) Bidirectional association between depression and type 2 diabetes mellitus in women. Arch Intern Med 170: 1884-1891.
-
American Diabetes Association (2009) Diagnosis and classification of Diabetes Mellitus. Diabetes Care 32(S1): s62-s67.
-
Ng R, Sutradhar R, Yao Z, Wodchis WP, Rosella LC (2020) Smoking, drinking, diet and physical activity-modifiable lifestyle risk factors and their associations with age to first chronic disease. Int J Epidemiol 49(1): 113-130.
-
Katon JG, Russo J, Gavin AR, Melville JL, Katon WJ (2011) Diabetes and depression in pregnancy: is there an association?. J Womens Health (Larchmt) 20(7): 983- 989.
-
Jones EJ, Roche CC, Appel SJ (2009) A review of the health beliefs and lifestyle behaviors of women with previous gestational diabetes. J Obstet Gynecol Neonatal Nurs 38(5): 516-26.
-
Ministerio de Salud y Protección Social de Colombia (2015) Clinical practice guideline for the diagnosis, treatment and follow-up of gestational diabetes. Sistema General de Seguridad Social en Salud, Colombia. Guía No GPC-2015-49.
-
Kalra B, Sridhar GR, Madhu K, Balhara YP, Sahay RK, et al. (2013) Psychosocial management of diabetes in pregnancy. Indian journal of endocrinology and metabolism 17(5): 815-818.
-
Gómez López ME (2018) Guide to psychological care for women with obstetric complications. Perinatología y Reproducción Humana 32(2): 85-92.
-
Gómez López ME (2007) Guide to psychological intervention for patients with high-risk pregnancy. Perinatología y Reproducción Humana 21: 111-121.
-
Ofman SD, Taverna MJ, Stefani D (2019) Importance of considering psychosocial factors in DM2. Revista Cubana de Endocrinología 30(2): e144.
-
National Institute for Health and Care Excellence NICE (2015) Diabetes in pregnancy: management from preconception to the postnatal period. NICE guideline Published.
-
(2015) Prevalence of positive screening for depression and anxiety in high-risk obstetric pregnants in a medellín clinic (colombia), between january and august 2013. Associated risk factors. Revista Colombiana de Obstetricia y Ginecología 66(2): 94-102.
-
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, et al. (2018) PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 169(7): 467-473.
-
Peters MDJ, Godfrey CM, McInerney, Khalil H, Parker D, et al. (2015) Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc 13(3): 141-146.
-
Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, et al. (2020) Chapter 11: Scoping Reviews. In: Aromataris E, Munn Z, et al. (Eds.), JBI Manual for Evidence Synthesis, JBI.
-
Joanna Briggs Institute (2014) Levels of Evidence and Grades of Recommendation Working, Party. Supporting Document for the Joanna Briggs Institute Levels of Evidence and Grades of Recommendation: The Joanna Briggs Institute.
-
Joanna Briggs Institute JBI (2015) Reviewers’ Manual: Methodology for JBI Scoping Reviews.
-
Peters MDJ, Casey M, Tricco A (2021) Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Implementation 19(1): 3-10.
-
Abraham K, Wilk N (2014) Living with gestational diabetes in a rural community. MCN Am J Matern Child Nurs 39(4): 239-245.
-
Arafa A, Dong JY (2019a) Gestational diabetes and risk of postpartum depressive symptoms: A meta-analysis of cohort studies. Journal of Affective Disorders 253: 312- 316.
-
Arafa A, Dong JY (2019b) Depression and risk of gestational diabetes: A meta-analysis of cohort studies. Diabetes Res Clin Pract 156: 107826.
-
Azami M, Badfar G, Soleymani A, Rahmati S (2019) The association between gestational diabetes and postpartum depression: A systematic review and meta- analysis. Diabetes Res Clin Pract 149: 147-155.
-
Berggren EK, Boggess KA, Funk MJ, Stuebe AM (2012) Racial disparities in perinatal outcomes among women with gestational diabetes. Journal of women’s health 21(5): 521-527.
-
Bouthoorn SH, Silva LM, Murray SE (2015) Low-educated women have an increased risk of gestational diabetes mellitus: The Generation R Study. Acta Diabetol 52(3): 445-452.
-
Burgut FT, Bener A, Ghuloum S, Sheikh J (2015) A study of postpartum depression and maternal risk factors in Qatar [published correction appears in J Psychosom Obstet Gynaecol 34(2): 90-97.
-
Carolan M, Steele C, Margetts H (2010a) Attitudes towards gestational diabetes among a multiethnic cohort in Australia. J Clin Nurs19 (17-18): 2446-2453.
-
Carolan M, Steele C, Margetts H (2010b) Knowledge of gestational diabetes among a multi-ethnic cohort in Australia. Midwifery 26(6): 579-588.
-
Carolan M, Gill GK, Steele C (2012) Women’s experiences of factors that facilitate or inhibit gestational diabetes self-management. BMC Pregnancy Childbirth 12: 99.
-
Carolan M, Duarte Gardea M, Lechuga J, Salinas-López S (2017) The experience of gestational diabetes mellitus (GDM) among Hispanic women in a U.S. border region. Sexual & Reproductive Healthcare. 12: 16-23.
-
Chavez-Courtois, Mayra (2014) Experience and perceptions of gestational diabetes and its self- management in a group of overweight multiparous women. Science. saúde coletiva 19(6): 1643-1652.
-
Clark CE, Rasgon NL, Reed DE, Robakis TK (2018) Depression precedes, but does not follow, gestational diabetes. Acta Psychiatrica Scandinavica 139(4): 311- 321.
-
Clevesy MA, Gatlin TK, Strebel KT (2018) Is There a Relationship Between Gestational Diabetes and Perinatal Depression?. MCN Am J Matern Child Nurs 43(4): 206- 212.
-
Colicchia LC, Parviainen K, Chang JC (2016) Social Contributors to Glycemic Control in Gestational Diabetes Mellitus. Obstet Gynecol 128(6): 1333-1339.
-
Cosson E, Bihan H, Reach G, Vittaz L, Carbillon L, et al. (2015) Psychosocial deprivation in women with gestational diabetes mellitus is associated with poor fetomaternal prognoses: an observational study. BMJ open 5(3): e007120.
-
Dahlen HG, Barnett B, Kohlhoff J (2015) Obstetric and psychosocial risk factors for Australian-born and non- Australian born women and associated pregnancy and birth outcomes: a population-based cohort study. BMC Pregnancy Childbirth 15: 292.
-
Damé P, Cherubini K, Goveia P, Pena G, Galliano L, et al. (2017) Depressive Symptoms in Women with Gestational Diabetes Mellitus: The LINDA-Brazil Study. Journal of diabetes research 7341893.
-
Devsam BU, Bogossian FE, Peacock AS (2013) An interpretive review of women’s experiences of gestational diabetes mellitus: proposing a framework to enhance midwifery assessment. Women Birth 26(2): e69-e76.
-
Doughty KN, Ronnenberg AG, Reeves KW, Qian J, Sibeko L (2018) Barriers to Exclusive Breastfeeding Among Women with Gestational Diabetes Mellitus in the United States. J Obstet Gynecol Neonatal Nurs 47(3): 301-315.
-
Draffin CR, Alderdice FA, McCance DR (2016) Exploring the needs, concerns and knowledge of women diagnosed with gestational diabetes: A qualitative study. Midwifery 40: 141-147.
-
Eades CE, France EF, Evans JMM (2018) Postnatal experiences, knowledge, and perceptions of women with gestational diabetes. Diabet Med 35(4):519-529.
-
Egan AM, Dunne FP, Lydon K, Conneely S, Sarma K, McGuire BE (2017) Diabetes in pregnancy: worse medical outcomes in type 1 diabetes but worse psychological outcomes in gestational diabetes. QJM 110(11): 721-727.
-
Engberg E, Stach-Lempinen B, Sahrakorpi N (2015) A cross-sectional study of antenatal depressive symptoms in women at high risk for gestational diabetes mellitus. J Psychosom Res 79(6): 646-650.
-
Figueroa-Gray M, Hsu C, Kiel L, Dublin S (2017) “It’s a Very Big Burden on Me”: Women’s Experiences Using Insulin for Gestational Diabetes. Matern Child Health J 21(8): 1678-1685.
-
García-Soidán FJ, Villoro R, Merino M, Hidalgo-Vega Á, Hernando-Martín TD (2017) Health status, quality of life and use of healthcare resources of patients with diabetes mellitus in Spain. Semergen 43(6): 416-424.
-
Ge L, Wikby K, Rask M (2016) ‘Is gestational diabetes a severe illness?’ exploring beliefs and self-care behavior among women with gestational diabetes living in a rural area of the southeast of China. Aust J Rural Health 24(6): 378-384.
-
Goldstein R, Gibson-Helm ME, Boyle JA, Teede HJ (2015) Satisfaction with diagnosis process for gestational diabetes mellitus and risk perception among Australian women. International Journal of Gynecology & Obstetrics 129(1): 46-49.
-
Hayase M, Shimada M, Seki H (2014) Sleep quality and stress in women with pregnancy-induced hypertension and gestational diabetes mellitus. Women Birth 27(3): 190-195.
-
Hjelm K, Bard K, Apelqvist J (2012) Gestational diabetes: prospective interview-study of the developing beliefs about health, illness, and health care in migrant women. J Clin Nurs 21(21-22): 3244-3256.
-
Hjelm K, Bard K, Apelqvist J (2018) A qualitative study of developing beliefs about health, illness, and healthcare in migrant African women with gestational diabetes living in Sweden. BMC Womens Health 18(1): 34.
-
Horsch A, Seon Kang J, Vial Y, Ehiert U (2016) Stress exposure and psychological stress responses are related to glucose concentrations during pregnancy. Br J Health Psychol 21(3): 712-729.
-
Hui AL, Sevenhuysen G, Harvey D, Salamon E (2014) Stress and anxiety in women with gestational diabetes during dietary management. Diabetes Educ 40(5): 668- 677.
-
Hussain Z, Yusoff ZM, Sulaiman SA (2015) Evaluation of knowledge regarding gestational diabetes mellitus and its association with glycemic level: A Malaysian study. Prim Care Diabetes 9(3):184-190.
-
Ilias I, Linardi A, Milionis C, Tselebis A, Koukkou E (2018) La procrastination dans l’autogestion du diabète gestationnel [Procrastination in the self-management of gestational diabetes]. Presse Med. 47(2): 180-181.
-
Jarvie R (2017) Lived experiences of women with co- existing BMI≥30 and Gestational Diabetes Mellitus. Midwifery 49: 79-86.
-
Jelsma JG, Van Leeuwen KM, Oostdam N (2016) Beliefs, Barriers, and Preferences of European Overweight Women to Adopt a Healthier Lifestyle in Pregnancy to Minimize Risk of Developing Gestational Diabetes Mellitus: An Explorative Study. J Pregnancy 2016: 3435791.
-
Kaiser B, Jeannot E, Razurel C (2016) Determinants of Health Behaviors After Gestational Diabetes Mellitus: A Prospective Cohort Study in Geneva. J Midwifery Womens Health 61(5): 571-577.
-
Kaptein S, Evans M, McTavish S (2015) The subjective impact of a diagnosis of gestational diabetes among ethnically diverse pregnant women: a qualitative study. Can J Diabetes 39(2): 117-122.
-
Keskin FE, Ozyazar M, Pala AS, Elmali AD, Yilmaz B, et al. (2015) Evaluation of cognitive functions in gestational diabetes mellitus. Exp Clin Endocrinol Diabetes 123(4): 246-251.
-
Kim Y, Lee JL, Jang IS, Park S (2020) Knowledge and Health Beliefs of Gestational Diabetes Mellitus Associated with Breastfeeding Intention Among Pregnant Women in Bangladesh. Asian Nurs Res (Korean Soc Nurs Sci) 14(3): 144-149.
-
Knippen KL, Sheu JJ, Oza-Frank R, McBride K, Dake J (2019) Predictors of Health-Protective Behavior and Glycemia after Gestational Diabetes, NHANES 2007- 2014. Diabetes Educ 45(4): 408-419.
-
Kopec JA, Ogonowski J, Rahman MM, Miazgowski T (2015) Patient-reported outcomes in women with gestational diabetes: a longitudinal study. Int J Behav Med 22(2): 206-213.
-
Kordi M, Heravan MB, Asgharipour N, Akhlaghi F, Mazloum SR (2017) Does maternal and fetal health locus of control predict self-care behaviors among women with gestational diabetes?. J Educ Health Promot 6: 73.
-
Kragelund-Nielsen K, Vildekilde T, Kapur A, Damm P, Seshiah V, et al. (2020) If I Don’t Eat Enough, I Won’t Be Healthy”. Women’s Experiences with Gestational Diabetes Mellitus Treatment in Rural and Urban South India. Int J Environ Res Public Health 17(9): 3062.
-
Krige SM, Booley S, Levitt NS, Chivese T, Murphy K, et al. (2018) Dietary Intake and Beliefs of Pregnant Women with Gestational Diabetes in Cape Town, South Africa. Nutrients 10(9): 1183.
-
Kubo A, Ferrara A, Brown SD (2017) Perceived psychosocial stress and gestational weight gain among women with gestational diabetes. PLoS One 12(3): e0174290.
-
Larrabure-Torrealva GT, Martinez S, Luque-Fernandez MA, Sanchez SE, Mascaro PA, et al. (2018). Prevalence and risk factors of gestational diabetes mellitus: findings from a universal screening feasibility program in Lima, Peru. BMC Pregnancy Childbirth 18(1): 303.
-
Lee K, Ching S, Hoo F (2019) Prevalence and factors associated with depressive, anxiety and stress symptoms among women with gestational diabetes mellitus in tertiary care centers in Malaysia: a cross-sectional study. BMC Pregnancy Childbirth 19: 367.
-
Lydon K, Dunne FP, Owens L, Avalos G, Sarma KM, et al. (2012) Psycho stress associated with diabetes during pregnancy: A pilot study. Irish Med J 105(S5): 26-28.
-
Mak JKL, Lee AH, Ngoc MP, Li T, Xiong Fei P, et al. (2019) Gestational diabetes and postnatal depressive symptoms: A prospective cohort study in Western China. Women and Birth 32(3): e427-e431.
-
Marchetti D, Carrozzino D, Fraticelli F, Fulcheri M, Vitacolonna E (2017) Quality of Life in Women with Gestational Diabetes Mellitus: A Systematic Review. Journal of diabetes research 7058082.
-
Martínez-Paredes JF, Jácome Pérez N (2019) Depression in pregnancy. Revista Colombiana de Psiquiatría 48(1): 58-65.
-
McMillan B, Easton K, Goyder E, Delaney B, Madhuvrata P, et al. (2018) Reducing risk of type 2 diabetes after gestational diabetes: a qualitative study to explore the potential of technology in primary care. Br J Gen Pract 68(669): e260-e267.
-
McParlin C, Hodson K, Barnes AC, Taylor R, Robson SC, et al. (2019) Views, experience, and adherence among pregnant women with gestational diabetes participating in a weight loss study (WELLBABE). Diabet Med 36(2): 195-202.
-
Miazgowski T, Bikowska M, Ogonowski J, Taszarek A (2018) The Impact of Health Locus of Control and Anxiety on Self-Monitored Blood Glucose Concentration in Women with Gestational Diabetes Mellitus. J Womens Health (Larchmt) 27(2): 209-215.
-
Molyneaux E, Begum S, Briley AL (2018) Do elevated symptoms of depression predict adherence and outcomes in the UPBEAT randomized controlled trial of a lifestyle intervention for obese pregnant women?. BMC Pregnancy Childbirth 18(1): 378.
-
Momeni JF, Simbar M, Dolatian M, Alavi Majd H (2014) Comparison of lifestyles of women with gestational diabetes and healthy pregnant women. Glob J Health Sci 7(2): 162-169.
-
Morrison C, McCook JG, Bailey BA (2016) First trimester depression scores predict development of gestational diabetes mellitus in pregnant rural Appalachian women. J Psychosom Obstet Gynaecol 37(1): 21-25.
-
Morrison MK, Lowe JM, Collins CE (2014) Australian women’s experiences of living with gestational diabetes. Women Birth 27(1): 52-57.
-
Muche AA, Olayemi OO, Gete YK (2019) Prevalence of gestational diabetes mellitus and associated factors among women attending antenatal care at Gondar town public health facilities, Northwest Ethiopia. BMC Pregnancy Childbirth 19(1): 334.
-
Muhwava LS, Murphy K, Zarowsky C, Levitt N (2019) Experiences of lifestyle change among women with gestational diabetes mellitus (GDM): A behavioral diagnosis using the COM-B model in a low-income setting. PLoS One 14(11): e0225431.
-
Mukerji G, Kainth S, Pendrith C (2016) Predictors of low diabetes risk perception in a multi-ethnic cohort of women with gestational diabetes mellitus. Diabet Med 33(10): 1437-1444.
-
Ekrem O, Sabah T, Berfu C, Burak O, Sinem T, et al. (2017) Antenatal Anxiety in Pregnant Women with Gestational Diabetes Mellitus. Ankara Med J 17: 111-118.
-
Pantzartzis KA, Manolopoulos PP, Paschou SA, Kazakos K, Kotsa K, et al. (2019) Gestational diabetes mellitus and quality of life during the third trimester of pregnancy. Qual Life Res 28(5): 1349-1354.
-
Párraga Moreira GJ (2020) Pedagogy of care in women at risk of gestational diabetes. Jipijapa. UNESUM. Facultad de Ciencias de la Salud Tesis pp: 104.
-
Parsons J, Sparrow K, Ismail K, Hunt K, Rogers H, et al. (2018) Experiences of gestational diabetes and gestational diabetes care: a focus group and interview study. BMC Pregnancy Childbirth 18(1): 25.
-
Parsons J, Sparrow K, Ismail K, Hunt K, Rogers H, et al. (2019) A qualitative study exploring women’s health behaviors after a pregnancy with gestational diabetes to inform the development of a diabetes prevention strategy. Diabet Med 36(2): 203-213.
-
Persson M, Winkvist A, Mogren I (2010) ‘From stun to gradual balance’--women’s experiences of living with gestational diabetes mellitus. Scand J Caring Sci 24(3): 454-462.
-
Ricardo Ramírez C, Álvarez Gómez M, Ocampo Saldarriaga MV, Tirado Otalvaro AF (2015) Prevalence of positive screening for depression and anxiety in high- risk obstetric pregnants in a medellín clinic (colombia), between january and august 2013. Associated risk factors. Revista Colombiana de Obstetricia y Ginecología 66(2): 94-102.
-
Ruiz-González I (2015) Prevalence of sleep disturbances and gestational diabetes in the last trimester of pregnancy. Nutr Hosp 32(3): 1139-1144.
-
Ruohomäki A, Toffol E, Upadhyaya S (2018) The association between gestational diabetes mellitus and postpartum depressive symptomatology: A prospective cohort study. J Affect Disord 241: 263-268.
-
Saadati F, Sehhatiei Shafaei F, Mirghafourvand M (2018) Sleep quality and its relationship with quality of life among high-risk pregnant women (gestational diabetes and hypertension). J Matern Fetal Neonatal Med 31(2): 150-157.
-
Sandsæter HL, Horn J, Rich-Edwards JW (2019) Preeclampsia, gestational diabetes, and later risk of cardiovascular disease: Women’s experiences and motivation for lifestyle changes explored in focus group interviews. BMC Pregnancy Childbirth 19: 448.
-
Schmidt CB, Voorhorst I, Van de Gaar VHW (2019) Diabetes distress is associated with adverse pregnancy outcomes in women with gestational diabetes: a prospective cohort study. BMC Pregnancy Childbirth 19: 223.
-
Siad FM, Fang XY, Santana MJ, Bualia S, Hebert MA, et al. (2018) Understanding the Experiences of East African Immigrant Women with Gestational Diabetes Mellitus. Canadian Journal of Diabetes 42(6): 632-638.
-
Singh H, Soyoltulga K, Fong T, Billimek J (2018) Delivery Outcomes, Emergency Room Visits, and Psychological Aspects of Gestational Diabetes: Results from a Community Hospital Multiethnic Cohort. Diabetes Educ 44(5): 465-474.
-
Sürücü HA, Besen DB, Duman M, Yeter EY (2018) Coping with Stress among Pregnant Women with Gestational Diabetes Mellitus. J Caring Sci 7(1): 9-15.
-
Sutherland L, Neale D, Henderson J, Clark J, Levine D, et al. (2020) Provider Counseling About and Risk Perception for Future Chronic Disease Among Women with Gestational Diabetes and Preeclampsia. J Womens Health (Larchmt) 29(9): 1168-1175.
-
Tang Y, Lan X, Zhang Y, Zhou F, Cai C, Zhang J, et al. (2020) Anxiety and depression on gestational diabetes mellitus in early pregnancy. Wei Sheng Yan Jiu 49(2): 179-184.
-
Trutnovsky G, Panzitt T, Magnet E, Stern C, Lang U, et al. (2012) Gestational diabetes: women’s concerns, mood state, quality of life and treatment satisfaction. The Journal of Maternal-fetal & Neonatal Medicine 25(11): 2464-2466.
-
Tsakiridis I, Bousi V, Dagklis T, Sardeli C, Nikolopoulou V, et al. (2019) Epidemiology of antenatal depression among women with high-risk pregnancies due to obstetric complications: a scoping review. Arch Gynecol Obstet 300(4): 849-859.
-
Twedt R, Bradley M, Deiseroth D, Althouse A, Facco F (2015) Sleep Duration and Blood Glucose Control in Women with Gestational Diabetes Mellitus. Obstetrics and gynecology 126(2): 326-331.
-
Varela P, Spyropoulou AC, Kalogerakis Z, Vousoura E, Moraitou M, et al. (2017) Association between gestational diabetes and perinatal depressive symptoms: evidence from a Greek cohort study. Prim Health Care Res Dev 18(5): 441-447.
-
Walmer R, Huynh J, Wenger J (2015) Mental Health Disorders Subsequent To Gestational Diabetes Mellitus Differ By Race/Ethnicity. Depress Anxiety 32(10): 774- 782.
-
Wilson BL, Dyer JM, Latendresse G, Wong B, Baksh L (2015) Exploring the Psychosocial Predictors of Gestational Diabetes and Birth Weight. J Obstet Gynecol Neonatal Nurs 44(6): 760-771.
-
Wilson CA, Newham J, Rankin J (2020) Is there an increased risk of perinatal mental disorder in women with gestational diabetes? A systematic review and meta-analysis. Diabet Med 37(4): 602-622.
-
Xiaoyu W (2019) Women’s experiences of gestational diabetes mellitus. A descriptive review. University of Gavle Lishui University, China. Student thesis, bachelor’s degree in nursing sciences.
-
Breuing J, Pieper D, Neuhaus AL (2018) Barriers and facilitating factors in the prevention of diabetes type II and gestational diabetes in vulnerable groups: protocol for a scoping review. Syst Rev 7: 245.
-
Gómez López ME, Berenzon Gorn S, Lara Cantú MA, Ito Sugiyama ME (2016) Psychological discomfort in women with high-risk pregnancy. Summa Psicológica UST 13(1): 89-100.
-
Pimentel-Nieto D (2007) Clinical guide for the psychological intervention of pregnant women with endocrinopathies. Perinatol Reprod Hum 21: 54-68.
-
Centro Nacional de Excelencia Tecnológica en Salud CENETEC-Salu (2014) Guía de Práctica Clínica Prevención, Diagnóstico y Manejo de la DEPRESIÓN PRENATAL Y POSPARTO en el Primero y Segundo Niveles de Atención. México.
-
Craig L, Sims R, Glasziou P (2020) Women’s experiences of a diagnosis of gestational diabetes mellitus: a systematic review. BMC Pregnancy Childbirth 20: 76.
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses PRISMA (2009). Transparent Reporting of Systematic Reviews and Meta-analyses. PRISMA Flow diagram.
-
Ross GP, Falhammar H, Chen R, Barraclough H, Kleivenes O, et al. (2016) Relationship between depression and diabetes in pregnancy: A systematic review. World Journal of Diabetes 7(19): 554-571.
-
Silveira ML, Whitcomb BW, Pekow P (2014) Perceived psychosocial stress and glucose intolerance among pregnant Hispanic women. Diabetes Metab 40(6): 466-475.
-
Sociedad Española de Diabetes SED (2019) Programa de Educación Terapéutica para mujeres con diabetes gestacional y/o familiares y/o cuidadores. Nivel Básico pp: 1-29.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda