New Experimental Model of Heterotopic Spleen Auto Transplantation
The aim of the study was to develop a new experimental model of heterotopic autotransplantation of the spleen by implanting splenic fragments into subcutaneous fat. Research Material: Experimental studies were conducted on 8 white mongrel rats weighing 300-400 grams at the age of 3 to 4 months. Research Results: Splenectomy is accompanied by significant violations of hemostasis and the immune system of the body, which justifies the feasibility of performing heterotopic autotransplantation of the spleen (GATS). In cases of infection or necrosis of the implant when performing traditional GATS methods, repeated surgical intervention under general anesthesia by laparotomy is required. The developed new method of GATS, which consists in implanting fragments of the spleen into subcutaneous adipose tissue, enveloped by an omentum "on the leg", in cases of necrosis or infection of the allograft, allows you to limit yourself to minimal surgical intervention under local anesthesia.
Khakimov MSh*, Matrizaev TZh, Zhumanazarov AU and Lyubentsova OV
Tashkent Medical Academy, Uzbekistan *Corresponding author: Khakimov M, Tashkent Medical Academy, Uzbekistan, Email: murad_72@mail.ru
Introduction
The urgency of the problem in the structure of abdominal injuries, spleen injuries occupies one of the leading places, the frequency of which is 20-25% of victims with abdominal trauma [1].
Most often, splenectomy is performed for injuries of the spleen. In the human body, the spleen performs many functions: it takes part in hematopoiesis; it plays a leading role in the hemostasis system and the body’s immune system. All these facts can contribute to the development of postoperative complications after splenectomy, which sometimes lead to fatal outcomes. In recent years, the tactics of preserving the spleen in case of its injuries has gained more and more supporters. Evidence of this is the growing number of scientific papers that substantiate the expediency of preserving the spleen, and if it is technically impossible to save it, performing heterotopic spleen autotransplantation (HSAT) [2].
Various methods of HSAT are known, which differ in the formation of autografts and the location in the patient’s body. The most common method is HSAT, which involves placing fragments of the spleen into the formed pouch of the greater omentum or retroperitoneum. Due to the existing shortcomings of these methods, HSAT methods were proposed in the liver parenchyma, in the left subdiaphragmatic space by fixing to the dome of the diaphragm, the mesentery of the small intestine [3].
Despite the existence of many methods of spleen autotransplantation, the views of their authors are contradictory, there is no unanimity in choosing the most optimal method of intervention, which could ensure the regeneration of spleen tissues with the restoration of its functions earlier after surgery, and would also be highly safe in terms of prevention. Possible complications in cases of autograft necrosis and its infection in conditions of massive post-traumatic infection of the abdominal cavity. One of the frequent postoperative complications of HSAT is the infection of the graft, less often there is lysis of the implant. These cases require repeated surgical treatment by performing a laparotomy, which can cause negative results of the interventions. The unresolved many issues in the problem of HSAT in traumatic injuries of the organ, the search for alternative options for preserving the splenic tissue in the body and protecting it from infection in patients after splenectomy, was the subject of this research work.
The aim of the study was to develop a new experimental model of heterotopic spleen autotransplantation by implanting spleen fragments into the subcutaneous fat.
Research Material
Experimental studies were carried out in the TMA vivarium on 8 outbred rats weighing 300-400 grams, aged
3 to 4 months, in compliance with the requirements of the European Convention for the Protection of Vertebrate Animals Used for Experimental and Other Scientific Purposes (Strasburg, 1986). At the first stage, on 4 rats, we evaluated the experimental model of HSAT into the subcutaneous tissue that we proposed. However, by the 15th day, lysis of the autograft is noted. In this connection, on 4 more rats, HSAT was made into the subcutaneous tissue, wrapped in an omentum on the leg. The evaluation of the results of implantation of the spleen into the subcutaneous tissue was made on the basis of morphological studies.
Results
Nami proposed the method of HSAT by implanting fragments of the spleen into the subcutaneous fat. The advantage of our proposed technique is the possibility of performing repeated interventions in case of infection or autograft lysis with minimal aggression without repeated laparotomy.
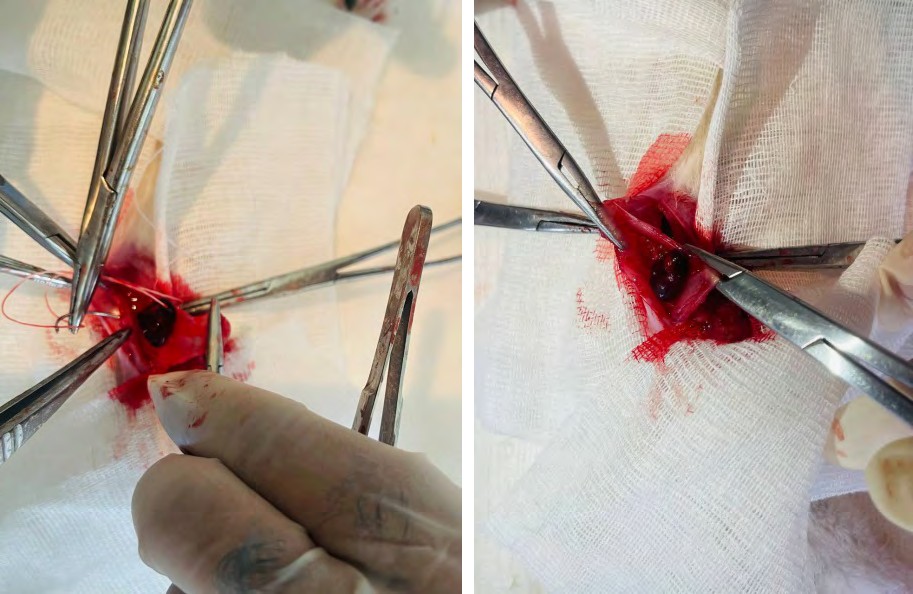
We have carried out experimental studies on the implantation of spleen fragments into the subcutaneous fat in 4 animals. Implantation was carried out in the incision area along the midline of the abdomen. Splenectomy was performed under standard conditions. A pocket was cut out in the supraponeurotic space, where a fragment of the spleen was implanted into the subcutaneous fat with suturing of the surgical wound (Figure 1).
Morphological studies were carried out on the 15th day. There is a thinning of the subcutaneous adipose tissue, in which there are foci of myxomatosis, fibrosis and a pronounced lymphoplasmacytic inflammatory reaction.
The muscle layer is thickened, with swollen, homogenized or necrotic fibers, between which there is a dense mixed inflammatory reaction (Figure 2). Aponeurotic layer with signs of proliferation of connective tissue. Morphological
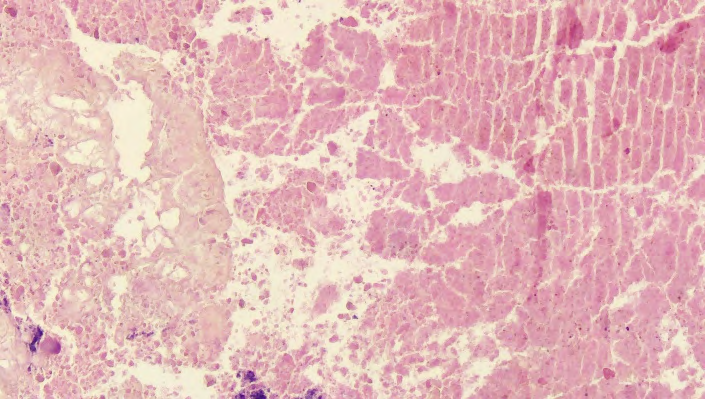
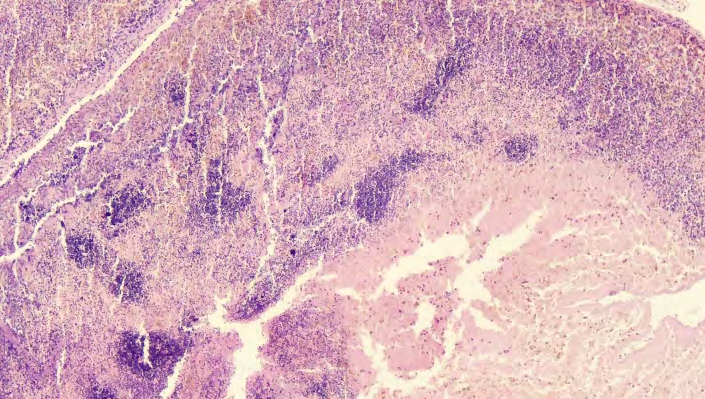
examination of the subcutaneous tissue in the area of the implanted fragment of the spleen showed chags of the spleen tissue with extensive fields of necrosis and small focal accumulations of tissue detritus. Adjacent fatty tissue in a state of necrosis and necrobiosis (Figure 3).
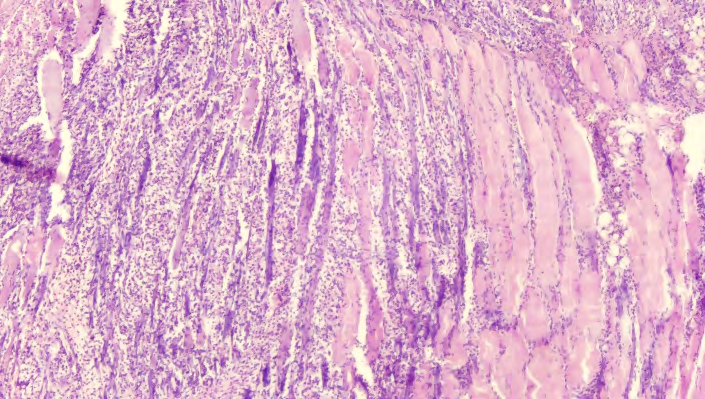

Figure 3: Necrosis of the spleen tissue and adjacent fatty tissue. Stained with hematoxylin and eosin. Ok.10. Ob.4 The conducted morphological studies have shown that with subcutaneous localization of the spleen autograft, pronounced alterative changes with necrosis of the spleen are noted. Pronounced inflammatory changes were revealed in the surrounding tissues. Given this fact, we decided to refrain from further continuation of experimental studies with the localization of spleen fragments in the subcutaneous tissue.
In order to distinguish spleen fragments from subcutaneous fat tissues and the impact of its fatty acids, we conducted studies on 4 more rats with autotransplantation of spleen fragments into the subcutaneous tissue, shrouded in a part of the greater pedunculated omentum.
The experiment was carried out as follows: after performing a traditional splenectomy and preparing a fragment of the spleen, the autograft was wrapped with a part of the greater omentum. The aponeurosis was sutured, while the greater omentum was removed between the sutures, a fragment of the spleen was wrapped around, a pocket was cut out in the subcutaneous tissue, where the implant was located (Figure 4). The skin was sutured. On the 15th and 30th days, material was taken for morphological study.

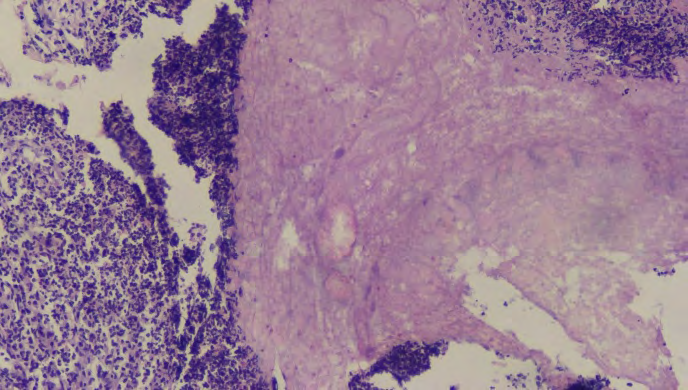
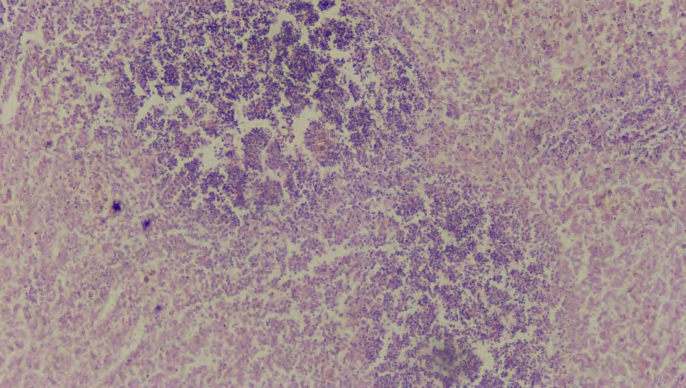
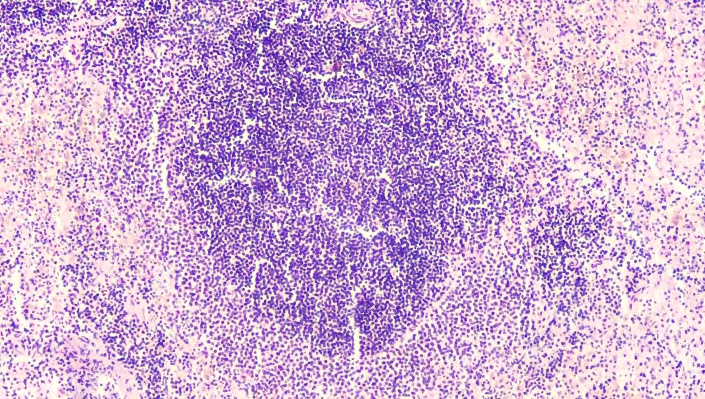
On the 15th day, with subcutaneous localization of a fragment of the spleen, shrouded in a greater omentum, the integumentary stratified squamous epithelium of the skin of uniform thickness, with moderate keratosis, the skin appendages are small, located in small groups. In the upper layers of the dermis around the vessels there are moderate accumulations of lymphocytes. The collagen fibers of the dermis are swollen. Subcutaneous adipose tissue is developed satisfactorily, with plethoric vessels, scattered lymphoplasmacytic infiltration. Muscle fibers with interstitial edema, myocyte dystrophy. Greater omentum with moderate leukocyte infiltration. At the same time, in the omentum, areas of acute inflammation alternate with zones of proliferative activity of cells of the fibroblast series a. The spleen capsule is thin, in some places on its surface there are slight accumulations of leukocytes. The red pulp of the spleen is sparse, with small foci of necrosis, mainly in the subcapsular zone, focal accumulations of hemosiderophages and segmented leukocytes (Figure 5). The follicles of the white pulp are small, located separately, mostly of the same size, with poorly expressed or absent germinal centers. The marginal zone is evenly developed (Figure 6).
On the 30th day of the experiment, the epidermis was slightly thinned in places, and slight hyperkeratosis was noted. The sebaceous glands are enlarged. Collagen fibers are thinned, discomplexed, isolated lymphocytes are found around the vessels. There are single suture foci with a perifocal reaction. There is a thickening of the subcutaneous adipose tissue, a moderate lymphoplasmacytic inflammatory reaction, and in some places foci of fibrosis. The muscle layer is moderately thickened, with swollen fibers, between which there is a slight inflammatory reaction. The greater omentum delimits the spleen tissues from the surrounding tissues, forming infiltrative adhesive processes (Figure 7) Spleen tissues in places with rare fields of necrosis, small focal accumulations of tissue detritus (Figure 8). Elements of red and white pulp are isolated.
Thus, the conducted studies have shown that with isolated localization of the spleen autograft, necrosis and tissue lysis are noted. As you know, the greater omentum, being a barrier, helps to limit the intraperitoneal focus of inflammation, forming infiltrative adhesive processes, which can prevent the spread of infection to other parts of the abdominal cavity; it is able to encapsulate foreign bodies. Questions concerning the influence of biologically active substances produced in the structures of the omentum on the activation or inhibition of the process of adhesion formation are very important. It should be emphasized that the structures of the greater omentum are actively involved not only in limiting the inflammatory process in the abdominal cavity, but also in protecting the abdominal organs, and in their various (traumatic, postoperative) injuries, which is also realized as an adhesive process. Given
this fact, we decided to use a greater omentum to isolate the autograft from the subcutaneous tissue by enveloping the implant with a pedunculated omentum. The conducted morphological studies showed good engraftment of spleen fragments, which made it possible to conclude that it is possible to perform HSAT into the subcutaneous tissue.
In functional terms, the implementation of HSAT testified to the restored lost functions of the spleen after splenectomy.
Splenectomy, in the general blood test, an increase in the indices of leukocytes, platelets and lymphocytes is noted, followed by their decrease. Moreover, after HSAT, the normalization of these criteria is noted already by the 15th day, while after splenectomy, even on the 30th day, their high level remains (Table 1).
In the coagulation system after splenectomy, fibrinogen and PTI increased, and APTT decreased. Carrying out HSAT contributed to the achievement of these analyzes of the preoperative level at different times. The fibrinogen index at the initial value of 2,8±0,3 g/l increased to 3,0±0,2 g/l by the 5th day and returned to the initial level by the 15th day. The PTI indicator reached the level of 82,1±3,4% on the 5th day, reached the initial level by the 30th day of the experiment (72,0±2,1%). APTT decreased on the first day after HSAT to 17,9±2,0 sec. With the normalization of this criterion by the 15th day (19,4±1,4 sec.) (Table 1).
| Index | Exodus | 5 days | 15 day | 30 days | |
|---|---|---|---|---|---|
| Leukocytes, *109 /l | After splenectomy | 11,6±1,0 | 11,3±0,7 | 10,8±0,7 | |
| After HSAT | 6,9±0,8 | 9,7±3,2 | 7,7±1,9 | 7,0±1,0 | |
| Student’s t-test | 0,567 | 1,778 | 3,113 | ||
| Thrombocytes, *109 /l | After splenectomy | 453,1±24,6 | 483,1±26,1 | 458,3±23,8 | |
| After HSAT | 355,8±19,1 | 403,3±19,1 | 371,4±16,2 | 358,9±14,9 | |
| Student’s t-test | 1,599 | 3,636 | 3,540 | ||
| Lymphocytes, % | After splenectomy | 63,3±2,1 | 60,6±1,6 | 61,5±1,0 | |
| After HSAT | 58,6±3,3 | 60,6±3,0 | 58,6±2,4 | 58,4±2,0 | |
| Student’s t-test | 0,737 | 0,693 | 1,386 | ||
| Fibrinogen, g/l | After splenectomy | 3,8±0,4 | 3,8±0,3 | 3,8±0,3 | |
| After HSAT | 2,8±0,3 | 3,0±0,2 | 2,8±0,2 | 2,8±0,3 | |
| Student’s t-test | 1,789 _ | 2,774 | 2,357 | ||
| PTI, % | After splenectomy | 86,1±2,9 | 86,5±3,6 | 86,5±1,5 | |
| After HSAT | 71,4±4,1 | 82,1±3,4 | 74,1±2,7 | 72,0±2,1 | |
| Student’s t-test | 0,895 | 2,756 | 5,619 | ||
| APTT, sec | After splenectomy | 15,9±1,2 | 14,8±0,8 | 14,5±0,5 | |
| After HSAT | 19,7±1,4 | 17,9±2,0 | 19,4±1,4 | 20,0±1,5 | |
| Student’s t-test | 0,857 | 2,853 | 3,479 | ||
| CD 3+ (T-lymphocytes), % | After splenectomy | 32,7±1,2 | 32,5±2,6 | 32,8±0,8 | |
| After HSAT | 41,8±2,0 | 35,9±2,0 | 41,8±1,8 | 42,3±1,4 | |
| Student’s t-test | 1,372 | 2,941 | 5,892 | ||
| CD 4+ (T-helpers), % | After splenectomy | 22,3±1,2 | 21,6±1,9 | 22,0±1,0 | |
| After HSAT | 31,4±1,4 | 26,8±1,7 | 29,9±1,8 | 31,7±1,6 | |
| Student’s t-test | 2,163 | 3,171 | 5,141 | ||
| CD 20+ (B-lymphocytes), % | After splenectomy | 12,1±0,8 | 13,8±1,6 | 13,3±1,3 | |
| After HSAT | 8,4±1,1 | 9,8±0,9 | 8,9±1,2 | 8,2±1,1 | |
| Student’s t-test | 1,910 | 2,450 | 2,995 | ||
| After splenectomy | 1,3±0,2 | 1,3±0,1 | 1,5±0,1 | ||
| IgA, g/l | After HSAT | 1,1±0,1 | 1,0±0,1 | 1,1±0,1 | 1,1±0,2 |
| Student’s t-test | 1,342 | 1,414 | 1,789 | ||
| After splenectomy | 1,3±0,1 | 1,1±0,1 | 1,1±0,1 | ||
| IgM, g/l | After HSAT | 1,6±0,2 | 1,2±0,2 | 1,4±0,2 | 1,6±0,3 |
| Student’s t-test | 0,447 | 1,342 | 1,581 | ||
| After splenectomy | 4,3±0,7 | 4,3±0,3 | 4,2±0,4 | ||
| Ig G, g/l | After HSAT | 7,3±0,5 | 6,4±0,8 | 7,0±0,7 | 7,4±0,5 |
| Student’s t-test | 1,976 | 3,545 | 4,998 |
Table 1: Comparative indicators of the general blood test.
After splenectomy, there was a decrease in cellular and humoral immunity. After the implementation of the HSAT, these indicators returned to their original values at various times. The CD 3+ index (T-lymphocytes) at the initial level of 41,8±2,0% decreased to 35,9±2,0% by the 5th day and again reached the initial level by the 15th day (41,8±1,8%). A similar trend was noted with CD 4+ (T-helpers) and CD 16+ (T-suppressors), but the dynamics was slower. So, with an initial value of 31,4±1,4% and 14,4±2,0%, respectively, and having decreased by the 5th day to 26,8±1,7% and 12,3±1,4%, only by the 30th day did they reach the initial level (31,7±1,6% and 14,2±1,8%). Among the indicators of humoral immunity, a particular change in Ig A is not marked. Ig values M , Ig G decreased after splenectomy. From the 5th day on the background of HSAT their increase was noted. With an Ig value M in the indicated terms was 1,6±0,2%, by the 30th day it reached the initial level of 1,6±0,3%; Ig index G increased from 6,4±0,8% to 7,4±0,5% (Table 1).
Discussion of the Results
The issues of HSAT, despite a rather long history of implementation and application in clinical practice, do not lose their relevance in the scientific world at the present time. Various approaches have been proposed for the implementation of this intervention and attempts to improve the results of traditional approaches to HSAT.
To improve the engraftment of the autograft, Afendulov S.A. proposed He-Ne laser treatment of the implant, which was used on 11 patients. The method of autotransplantation proposed by the authors makes it possible to achieve engraftment of the autograft and reduce the frequency of postoperative complications, restore the function of the lost spleen [4].
The clinical effect of HSAT depends on the dimensions of the implant. Small grafts can be resorbed, while too large grafts can undergo necrosis with the development of abscesses, which causes HSAT to be ineffective [5, 6]. Kirpatovsky ID [7] recommends performing HSAT by implanting 4-5 slices of the removed spleen 5 mm thick into the greater omentum. At the same time, the author does not exclude the possibility of lysis or fragmentation of spleen tissues.
In the work of Tveritneva LF [8] showed that the rate of implant recovery depends on the reticular framework and the presence of the spleen capsule. This fact indicates the expediency of transplantation of spleen fragments with a capsule, which serve as a scaffold for lymphoid tissue. In our studies, a large omentum was used as a frame.
Thus, we carried out experimental studies to develop a new approach to HSAT, which consisted in implanting a fragment of the spleen into the subcutaneous tissue. The choice of this localization was due to the fact that in situations with HSAT in the abdominal cavity or retroperitoneal space, there is a possibility of performing a second laparotomy in cases of infection or lysis of the autograft. However, during experimental studies on the implantation of an autograft into the subcutaneous tissue, organ lysis occurred in the early stages. This fact prompted us to the idea of conducting HSAT of a fragment of the spleen, wrapped in a greater omentum “on the leg”. The conducted morphological studies have shown a good implant survival. However, the analysis of the literature data showed that it is necessary to conduct additional studies to determine the optimal volume of the autograft, which would allow adequate restoration of the lost functions of the spleen, which was the subject of our subsequent studies.
Conclusions
Splenectomy is accompanied by significant disorders of hemostasis and the immune system of the body of the experimental animal, which justifies the expediency of performing heterotopic spleen autotransplantation. However, in cases of infection or necrosis of the implant when performing traditional methods of heterotopic spleen autotransplantation, a second surgical intervention under general anesthesia by laparotomy is required, which has a certain frequency of postoperative complications, which leads to the search for less traumatic implantation methods [1].
The developed new method of heterotopic autotransplantation of the spleen, which consists in implanting fragments of the spleen into the subcutaneous fat, shrouded in a pedunculated omentum, in cases of necrosis or infection of the allograft, allows us to limit ourselves to minimal surgical intervention under local anesthesia.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda