Exploring the Role of Leadership in Shaping Organizational Wellness and Employee Health
Objective: This qualitative case study aims to determine the state of workplace wellness activities in organizations in Midwestern and Southern states. Specifically, this study looks at the roles of top-down leadership and organizational goals as determinants of a healthy workforce. Design/Methodology/Approach: Participants were asked about workplace wellness programs using the Centers for Disease Control (CDC) Health Scorecard (HSC). Additionally, qualitative interviews asked participants questions about their workplace wellness programs. The results of the qualitative interviews were transcribed and compared to the literature for patterns, themes, and outliers. Participants: Participants were college-educated employees. They were asked to share information on their organizations’ workplace wellness practices. Main outcome measures: The CDC HSC consists of 125 questions totaling 265 points. Organizations were measured based on their scores falling in the top, middle, and lower third of scores. Their qualitative answers were used to add depth and meaning to the scores. Results/conclusions: Workplace wellness programs are successful when they are supported from top-down leadership, multiple marketing methods are utilized, and a focused person is responsible for corporate initiatives. Originality: This article provides the unique perspective of professionals in the field of workplace wellness.
Abbreviations
CMS: Centers for Medicare and Medicaid Services; GDP: Gross Domestic Product; HERO: Health Enhancement Research Organization; ROI: Return on Investment; APA: American Psychological Association; EAPs: Employee Assistance Programs; HRAs: Health Risk Assessments; HSC: Health Scorecard.
Introduction
Employee health is a crucial aspect of organizational efficiency and productivity. In the United States, the financial burden of employee health on employers has been steadily increasing, driven by rising healthcare costs, the prevalence of chronic diseases, and the growing demand for comprehensive wellness programs. This essay explores the various dimensions of these costs, examining their implications for employers and the potential strategies to mitigate them.
One of the primary drivers of the high cost of employee health is the escalating healthcare expenses. According to the Centers for Medicare and Medicaid Services (CMS), the national health expenditure in the U.S. reached $4.3 trillion in 2021, accounting for 19.7% of the Gross Domestic Product (GDP) [1]. This trend is expected to continue, with healthcare costs projected to grow at an average annual rate of 5.4% from 2022 to 2031 [1]. For employers, this translates into higher premiums for health insurance plans, with the average annual cost of family health insurance coverage exceeding $22,000 in 2023, up 5% from the previous year [2].
U.S. consumer prices rose by 3.7% over the 12 months through August, a decrease from the peak inflation rate of 9.1% in June of the previous year. Medical cost increases typically lag behind general inflation because contracts between insurers and hospitals for procedure prices are often negotiated months or even a year in advance [2, 3]. Benefit consultants are crucial in designing insurance plans for medium and large employers, with about two-thirds of U.S. workers receiving benefits through such plans [4].
Chronic diseases such as diabetes, heart disease, and obesity are significant contributors to the high cost of employee health. The Centers for Disease Control and Prevention (CDC) reports that chronic diseases account for 90% of the nation’s $3.3 trillion in annual healthcare costs [5]. Employers feel the impact through increased medical claims, higher absenteeism, and reduced productivity. A study by the Health Enhancement Research Organization (HERO) found that chronic disease management programs can reduce healthcare costs by up to 20% [6]. However, the initial investment in these programs remains a challenge for many organizations.
Beyond direct medical costs, absenteeism and presenteeism significantly affect organizational productivity and profitability. Absenteeism, or the frequency of employees missing work due to illness, costs U.S. employers approximately $225.8 billion annually, with an average of 8.7 days of work lost per employee each year [7]. Presenteeism, where employees attend work despite being ill, is even more costly, with estimates suggesting it costs employers between $150 billion and $250 billion annually due to reduced productivity and errors [8]. Effective health management programs that address both absenteeism and presenteeism are essential for mitigating these costs.
Investing in workplace wellness programs is a strategic approach to controlling healthcare costs and enhancing employee well-being. The RAND Corporation’s analysis indicates that well-implemented wellness programs can yield a return on investment (ROI) of $1.50 to $3.00 for every dollar spent, primarily through reduced healthcare costs and lower absenteeism [9]. Successful programs often include physical activity incentives, nutritional counseling, and stress management workshops. Additionally, programs that integrate mental health support have shown significant benefits, with the American Psychological Association (APA) noting a 30% reduction in healthcare costs for organizations that support mental health [10].
Despite the benefits, many employers face challenges in implementing effective health programs. Cost concerns, lack of employee engagement, and insufficient data to measure program effectiveness are common barriers. Employers are increasingly turning to data analytics and technology to overcome these challenges. Wearable technology, health apps, and predictive analytics can enhance the personalization and effectiveness of wellness programs, making them more appealing and impactful [11]. Moreover, fostering a culture of health and wellness within the organization is crucial, as it encourages employee participation and long-term commitment to health initiatives.
The CDC HSC provides an example budget organizations can use to begin their wellness initiatives. Centers for Disease Control and Prevention [5] “The following is a sample budget justification form for a company of 300 employees. This form should go hand in hand with the worksite health plan in seeking financial support for the worksite health program” [5].
| Item | Subtotal | Total Cost | |
|---|---|---|---|
| Wages/Benefits | Part-time Wellness Director | $20,000 | $20,000 |
| Materials and Supplies | Lighting and paint for stairwell project | $300 | $950 |
| Materials and Supplies | Printing for posters, fliers, etc. | $500 | $950 |
| Materials and Supplies | Supplies for Healthy Pot-Luck lunch | $150 | $950 |
| Memberships/Affiliations | Wellness Council of Greater Cornville National | $500 | $550 |
| Memberships/Affiliations | Network of Wellness Councils | $50 | $550 |
| Subscriptions and Publications | Electronic newsletter service | $175 | $325 |
| Subscriptions and Publications | Various health publications | $150 | $325 |
| Health Education Materials | Blood pressure log-books | $500 | $800 |
| Health Education Materials | Blood pressure literature and DVD | $300 | $800 |
| Health Assessment & Screenings | Currently planned for Year 2 | $0 | $0 |
| Health Coaching | Currently planned for Year 2 | $0 | $0 |
| Health Plan Changes | Currently planned for Year 2 | $0 | $0 |
| Health Education Programs | Blood pressure educational workshops | $250 | $500 |
| Health Education Programs | Blood pressure literature and DVD | $250 | $500 |
| Equipment | Blood pressure monitoring equipment | $800 | $5,450 |
| Equipment | Bike rack | $450 | $5,450 |
| Equipment | Pedometers | $2,200 | $5,450 |
| Equipment | Bike parking structure | $1,500 | $5,450 |
| Equipment | Bicycles/helmets for sign-out program | $500 | $5,450 |
| Incentives | Gift cards and prizes for contests, raffles, etc. | $1,000 | $7,000 |
| Incentives | Gym reimbursement | $6,000 | $7,000 |
| Miscellaneous | Contract with landscaper to create walking paths on property | $8,000 | $8,820 |
| Miscellaneous | Gym reimbursement | $820 | $8,820 |
| Total | $44,395 | ||
Table 1: Sample Worksite Health Budget.
The cost of employee health in the United States presents a substantial challenge to employers, influenced by rising healthcare costs, the prevalence of chronic diseases, and productivity losses due to absenteeism and presenteeism. However, employers can significantly mitigate these costs by investing in comprehensive wellness programs and leveraging technology, enhancing employee health and organizational performance. Future strategies should focus on integrating health management with broader organizational goals, fostering a culture of wellness, and utilizing innovative technologies to track and improve health outcomes.
This article provides a brief review of the relevant literature. Next, a description of the research approach, including the qualitative data in the form of interview transcripts from twenty-five individuals on the topic of top-down leadership, budgets, and organizational goals as determinants of a healthy workforce, is discussed. The article concludes with a discussion and suggestions for future research.
Literature Review
Workplace wellness programs have gained prominence over the past few decades as organizations recognize the benefits of promoting employee health and well-being. These programs aim to improve physical and mental health, reduce healthcare costs, and enhance productivity. This literature review explores the various aspects of workplace wellness programs, including their design, effectiveness, challenges, and future directions.
The concept of workplace wellness programs originated in the mid-20th century with the advent of employee assistance programs (EAPs) that primarily focused on mental health and substance abuse issues [12]. Over time, these programs evolved to include a broader range of health promotion activities, such as physical fitness, nutrition, stress management, and chronic disease management [13].
Effective workplace wellness programs are typically comprehensive, incorporating multiple components to address various health aspects. Key elements often include:
Health Risk Assessments (HRAs): Tools used to evaluate employees’ health status and identify risk factors. These assessments form the foundation for personalized health interventions [14]. Physical Activity Programs: Initiatives such as on-site gyms, fitness challenges, and group exercise classes aimed at increasing physical activity levels among employees [15]. Nutritional Counseling: Programs that guide healthy eating habits, often including workshops, dietary plans, and access to healthy food options at the workplace [16]. Mental Health Support: Services that offer stress management workshops, counseling, and mental health resources to address psychological well-being [17]. Chronic Disease Management: Programs designed to support employees with chronic conditions through regular monitoring, education, and access to medical care [9].
Effectiveness of Workplace Wellness Programs
Numerous studies have demonstrated the positive impact of workplace wellness programs on health outcomes and organizational performance. Key findings include: Health Improvements: Wellness programs have been associated with reductions in risk factors such as obesity, high blood pressure, and high cholesterol [16]. For example, a meta-analysis by Chapman LS [18] found that workplace wellness programs reduced employees’ body mass index (BMI) by an average of 0.5 points. Healthcare Cost Savings: Employers can achieve significant savings on healthcare costs through the implementation of wellness programs. Baicker K, et al. [9] reported that medical costs fell by about $3.27 for every dollar spent on wellness programs. Productivity Gains: Wellness programs can lead to lower absenteeism and presenteeism, resulting in productivity gains. A study by the RAND Corporation Mattke S, et al. [14]
found that employees participating in wellness programs had fewer sick days and higher productivity levels.
Challenges and Barriers
Despite their benefits, workplace wellness programs face several challenges: Engagement and Participation: One of the primary challenges is achieving high levels of employee engagement and sustained participation. Lack of time, perceived relevance, and program accessibility can affect participation rates [16]. Measuring ROI: Quantifying the return on investment (ROI) for wellness programs can be complex due to the difficulty in isolating the program’s effects from other variables and the long timeframes required to see significant health improvements [13]. Privacy Concerns: Employees may be concerned about the confidentiality of their health data, which can hinder participation in health assessments and other program components [17].
The future of workplace wellness programs lies in leveraging technology and data analytics to enhance program effectiveness and engagement. Emerging trends include:
Personalization: Using data from HRAs and wearable devices to provide personalized health interventions tailored to individual needs and preferences [11]. Integration with Corporate Culture: Embedding wellness programs into the organizational culture to ensure that health and well-being are prioritized at all levels [12]. Comprehensive Mental Health Support: Expanding the focus on mental health by integrating mental health services into existing wellness programs and reducing the stigma associated with seeking help [10].
Workplace wellness programs have become an integral part of organizational strategy, offering significant benefits in health improvements, cost savings, and productivity gains. However, engagement, ROI measurement, and privacy challenges must be addressed to maximize their potential. The integration of technology and a holistic approach to employee well-being are likely to shape the future of these programs, making them more effective and sustainable.
Methods
A combination of data collection methods was used to answer the central questions of this study. First, participants were given the CDC Health Scorecard (HSC) to develop a consistent baseline among all participants for measuring how organizations approach health and wellness. The CDC HSC is an assessment tool that helps employers evaluate their health promotion programs, identify gaps, and develop effective strategies to implement interventions addressing physical movement, tobacco control, safety, heart disease, stroke, chronic health conditions, and other workplace wellness issues. The questionnaire consists of 125 questions totaling 265 points, covering various aspects of workplace health and wellness initiatives.
During the completion of the CDC HSC survey, participants were encouraged to elaborate on their wellness programs or lack thereof. This additional commentary provided context and depth to their responses, allowing for a more comprehensive understanding of each organization’s approach to health and wellness.
Following the survey, participants responded to open- ended interview questions to explore how they are, or are not, addressing health and wellness in their workplace. These qualitative questions allowed participants to describe, in their own words, their health and wellness programs and any additional thoughts not included in the survey. The qualitative questions were developed directly from the central research questions and were asked of all participating organizations to ensure repeatability and reliability.
Qualitative Analysis and Manual Coding
The qualitative data collected from the open-ended interviews were subjected to a thorough analysis. All interviews were transcribed into typed text, resulting in approximately 800 pages of text over 1,100 minutes of interview recordings. This extensive transcription process ensured that no valuable information was overlooked.
In this case study, roughly an hour is required on behalf of the participant. This includes forty-five minutes to complete the CDC HSC and another fifteen minutes to ask open-ended interview questions. Participants are interviewed in a quiet and safe setting that does not cause any harm, danger, intimidation, or coercion to the participants. Participants agree to the location before the interview. For instance, the interview will be in a one-on-one context to avoid the altering of answers due to peer pressure or to please an on- looking boss. Participants will not receive any direct benefits from participating in this survey.
The qualitative analysis involved manual coding of the interview transcripts. Researchers use Manual coding to identify patterns, themes, and categories within qualitative data by systematically tagging text segments. This process was conducted in several stages:
Initial Reading and Note-Taking: The transcribed interviews were read and re-read to familiarize the researchers with the content. Initial notes were taken during this stage to capture immediate impressions and potential themes. Open Coding: In this stage, the text was broken down into discrete parts and labeled with codes that described the content. Codes were applied to words, phrases, sentences, or paragraphs representing key ideas or concepts relevant to the study’s research questions. Axial Coding: The researchers grouped codes into broader categories and subcategories after open coding. This stage involved identifying relationships between codes and organizing them into a coherent structure that reflected the main themes and sub-themes of the data. Selective Coding: The final stage involved refining and integrating the categories to develop a comprehensive understanding of the data. Core themes were identified, and supporting data were organized to illustrate these themes clearly and effectively.
The manual coding process ensured the analysis was grounded in the data, providing a detailed and nuanced understanding of the participants’ perspectives on workplace wellness. This rigorous approach to qualitative analysis allowed the researchers to uncover rich insights into the factors that influence the success of wellness programs and the challenges organizations face in promoting employee health and wellness.
Participants were college-educated employees. They were asked to share information on their organizations’ workplace wellness practices. The next strategy was to ask twenty-five individuals in technology-related organizations that the researcher knew personally. These individuals had a variety of roles in the organizations. Because the researcher knew these individuals personally, there was selection bias in the population that was used for the study. However, the type of technology-related company and the participants’ roles inside the organizations vary such that the selection bias is minimized by including a variety of respondents.
| Description of Organizations by Industry | Number of Employees | |
|---|---|---|
| Category 1: 201-264 HSC Points | ||
| 252 | Manufacturing | 1500 |
| 242 | Educational Services | 350 |
| 237 | Manufacturing | 25 |
| 205 | Manufacturing | 1000 |
| Category 2: 101-200 HSC Points | ||
| 160 | Transportation, Warehousing, Utilities | 25 |
| 154 | Manufacturing | 70 |
| 147 | Professional, Scientific, and Technical Services | 30 |
| 131 | Transportation, Warehousing, Utilities | 48 |
| 123 | Manufacturing | 100 |
| 117 | Transportation, Warehousing, Utilities | 500 |
| 110 | Construction | 500 |
| 103 | Professional, Scientific, and Technical Services | 125 |
| 101 | Retail/Wholesale Trade | 2500 |
| Category 3: 44-100 HSC Points | ||
| 99 | Manufacturing | 450 |
| 72 | Manufacturing | 160 |
| 65 | Manufacturing | 43 |
| 62 | Professional, Scientific, and Technical Services | 7 |
| 56 | Construction | 6 |
| 44 | Professional, Scientific, and Technical Services | 13 |
Table 2: Description of Organizations by Industry, HSC Score, and Number of Employees.
Limitations
One limitation is the reliance on the CDC scorecard, which may not fully capture the wellness programs’ effectiveness despite validation and improvements by Emory University researchers. The scorecard can yield high scores even when employees continue poor health behaviors, such as poor nutrition or tobacco use. Conducting in-person interviews and surveys with organizational leaders is time- consuming, limiting the depth and number of participants. Additionally, the study provides only a snapshot in time, and circumstances for participants can change, affecting the results. The study’s focus on Midwest and Southern states presents several challenges:
- Diverse socioeconomic and demographic profiles affect health behaviors and program outcomes.
- Rural areas often lack healthcare facilities and wellness resources, leading to disparities in program participation and effectiveness. [19, 20, 21, 22, 23, 24].
- Varying cultural norms and health literacy levels influence how wellness programs are perceived and utilized.
- Underdeveloped infrastructure and extreme weather conditions can hinder program implementation and maintenance.
The study’s sample of a college-educated workforce with an average age of 30 may not be representative of the broader regional workforce, which includes many employees with lower educational attainment and older age groups. This discrepancy can skew results, as health behaviors and program engagement vary with education level and age, limiting the study’s generalizability.
Workplace wellness programs may be confidential due to competitive advantage or proprietary information concerns. Employers may also wish to conceal the lack of a wellness program. To ensure authentic feedback, confidentiality is maintained by describing organizations in a non-specific manner, such as “a $100 million per year manufacturer with 500-600 employees.”
Results
The findings of the qualitative questions explain the organizational structure’s features that encourage healthy behaviour. These findings help companies benchmark their score against the workplace wellness programs from the HSC CDC validation study. The purpose of the HSC is to serve as an assessment tool for employers to examine their health promotion programs, to identify gaps, and to develop an effective strategy to implement interventions that address physical movement, tobacco control, safety, heart disease, stroke, chronic health conditions, and other workplace wellness issues addressed in the CDC HSC. The analysis of the data collected examined patterns and trends that emerged.
| Summary of Organizational Supports Scores | ||||||
|---|---|---|---|---|---|---|
| Health Score Card Category | Total Points Possible | CDC | <100 Employees (10 Orgs.) | 100-249 Employees (2 Orgs.) | 250-749 Employees (4 Orgs.) | >749 Employees (3 Orgs.) |
| Validation Study Scores | ||||||
| Organizational Supports | 33 | 24 | 13 | 14 | 12 | 21 |
Table 3: Summary of Organizational Supports Scores
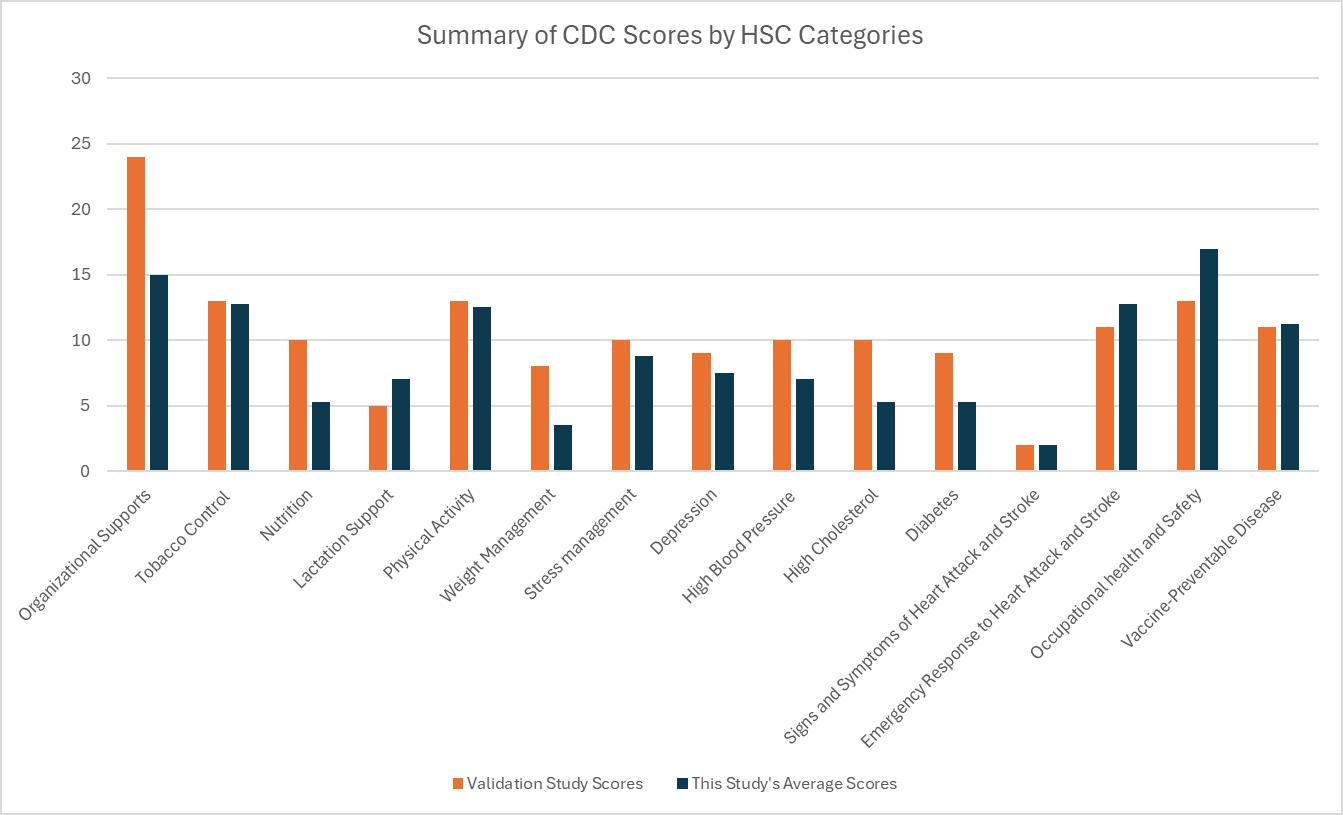
The following table (Table 4: Summary of CDC Scores by HSC Categories) and image (Figure 1: Summary of CDC Scores by HSC Categories) show, the differences between the 93 organizations’ scores from CDC’s validation study by Emory University and those of the organizations in this study. The following categories had more than 40% differences between the Validation Study and this study in the Midwestern and Southern United States: Organizational Supports, Nutrition, Weight Management, High Cholesterol, and Diabetes. Leaders and researchers can examine these categories and differences in their organizations or studies. The categories of Nutrition, Weight Management, High Cholesterol, and Diabetes are differentiated in the CDC Health Scorecard, they are interrelated. Further, they can all be affected by leadership and organizational policy, which might explain why all of these categories show such a difference in both studies.
- Summary of CDC Scores by HSC Categories
- HSC Categories
- Validation Study Scores
- This Study’s Average Scores
- Differences in Scores
- Organizational Supports
- 24
- 15
- 38%
- Tobacco Control
- 13
- 12.8
- 2%
- Nutrition
- 10
- 5.3
- 48%
- Lactation Support
- 5
- 7
- 40%
- Physical Activity
- 13
- 12.5
- 4%
- Weight Management
- 8
- 3.5
- 56%
- Stress management
- 10
- 8.8
- 13%
- Depression
- 9
- 7.5
- 17%
- High Blood Pressure
- 10
- 7
- 30%
- High Cholesterol
- 10
- 5.3
- 48%
- Diabetes
- 9
- 5.3
- 42%
- Signs and Symptoms of Heart Attack and
- Stroke
- 2
- 2
- 0%
- Emergency Response to Heart Attack and
- Stroke
- 11
- 12.8
- 16%
- Occupational health and Safety
- 13
- 17
- 31%
- Vaccine-Preventable Disease
- 11
- 11.3
- 2%
Table 4: Summary of CDC Scores by HSC Categories.
This section examines top-down leadership commitment to wellness and on a high-scoring industrial manufacturer. Other companies have top-down initiatives, but the industrial manufacturing organization emphasized their corporate officers’ and their owners’ role in all their health initiatives. According to their HR Manager, their health initiatives all started with corporate. (Corporate) held the first health fair and then it just went from there. All of our different facilities have a wellness committee. Most of them have a garden. I would want to say, also it’s provided by corporate, it’s promoted by corporate from the top down.
The Health Coordinator and Champion added that “the corporate office started doing the health fair in 2008, and then all the plants started doing health fairs. (Corporate) started the fitness center, and then all the plants had fitness centers.” This organization also has name-brand programs for their gyms, kitchens, gardens, and other programs. For instance, in the interest of confidentiality, if their name were Acme, Co., they’d have Acme-Gym, Acme-Kitchen, and Acme- Garden.
Their HR Manager states that, it’s all promoted from the top down and they provide the resources for the training or information on how to get one of these started, just like US Wellness (and their online program.) Corporate are the ones that are flipping the bill for that third party administrator to provide programs to all the associates.
Their overall company has 2200 employees and because of the close-knit nature of their organization and the corporate support, they leverage all the knowledge enterprise wide.
Other organizations in the study demonstrated top-down leadership and how it leads to their scores. An organization in the educational services industry, the leadership team is very flexible with time off for illness and pursuing school. This interviewee further stated that their organization is committed to keeping health and dental insurance costs incredibly low. She shared that premiums, for the employee, “went up about a dollar (in the last year). We have probably the most reasonable health insurance around.” The interviewee from the educational services industry feels that the leadership’s commitment to health makes up for lower wages. In her words, I think with everything they offer, it makes it worthwhile working there. The paycheck may not always be the best, but the benefits kind of outweigh the (lower wages), with the education and everything. Leadership is also very concerned about safety. Health education classes may not cost a lot for a large organization, but they can show a commitment to the wellness of employees.
An engineer in the manufacturing industry stated that their leadership team plays basketball with the employees to demonstrate their commitment to physical activity. In his words, “we have higher level managers that play basketball with us every week.” This organization has a very active culture, with a sports complex within walking distance of their facility. However, as a display of leadership commitment lacking, this interviewee mentioned that the organization does not have a designated person to solely promote wellness programs. He stated that “we don’t have that person to promote the programs. We do have a training division in HR that makes sure that every year that we repeat programs and information.” This instance demonstrates that it is possible to score high on the HSC without a full-time wellness coordinator when wellness is embedded in the culture.
A very high-scoring automobile manufacturer has a goal of health screenings for 90% or more of employees. In their words, 90% is not easy, and it is a goal that is twice the number that is common in their area. In order to achieve that number, the organization provides multiple incentives and pays them for the time they are away from work and at the clinic. According to their Corporate Care Manager, our goal for health screens are 90% or greater. In the community here locally the average if you go interview a bunch of folks, if you get 45% participation, you’re doing pretty good. We really push it, and we pay them. It’s on company time; they’re on the clock.
This automobile manufacturer, who has been focusing on wellness for over ten years, also shared some cautions to organizations that try to match their results too quickly. Their Corporate Care Manager stated that, if you just walk into a company that doesn’t have that culture that’s been built from the top down all those years and then try to say ‘oh we’re going to get 90% (of health assessments).’ It won’t work. You need foundational principles (and) that’s so important. That wellness culture is so important. It might take ten years to transform a culture to a world class level.
It is also important to discuss the aspects of organizational culture, including budgetary concerns. High- scoring organizations in the study mentioned concepts related to wellness programs that were impacted by their budget. On the positive side, a social services organization stated that implementing a Human Resources Coordinator position allowed the organization the opportunity to offer more wellness programs. Having a partially funded position also allowed them to communicate with their employees about the wellness programs. The HR Coordinator stated that, “my position is very new to the agency. My focus is on wellness, but it’s also on recruitment and training as well. It’s not solely on wellness.” This statement suggests that even a partial financial commitment can be a “big factor” in the wellness programming of the employees.
Interviewees mentioned a budget as a negative constraint more frequently than they mentioned the budget in a positive light regarding wellness. The organization in education services mentioned the distance from their corporate office and wellness programs offered there as a negative situation. According to the leader of that institution, we could technically start a program locally, we could ask for funds, and then we could answer all of these (survey questions) differently. I’m really answering from the location level, and we’re three hours away unfortunately. I think you’re going to find in this region, unfortunately, a high percentage of entities like us that aren’t investing.
This same organization felt that having a part-time employee to manage these resources could be very helpful, but they “do not have the funds to hire a wellness professional. We have not allocated the funds and we have not seen the value of having someone to focus on these areas.” Their employees also travel to their corporate office at least once a year, where many wellness services are available for little or no charge.
The organization in the social services industry felt that their nutrition scores were negatively impacted by budget constraints. The interviewee felt that being small prevents them from having cafeterias and snack bars and creates reliance on vending machines. The HR Coordinator stated that, “I think because we’re small as an agency on this particular site so we don’t have options for having a cafeteria, snack bar, things of that nature. All we have is those vending machines that are out there.” This interviewee in the social services industry stated that they have goals to promote their wellness activities. Their HR Coordinator states that “overall, the measurement is providing ongoing health education to the employees.” The strategic plan includes the actual steps they will take, with the timeline to be completed. The interviewee states that their strategic goal specifically says, “four health and wellness educational sessions and monthly distribution of health education articles.” Further, she suggests that, I’m sure it was written before this position came to be because I can tell you that my goal is to send out weekly information on some these items. Therefore, we’re meeting these goals and actually surpassing some of them.
The industrial manufacturer, who had the second highest score in the study, participates in community round tables where organizations share worksite wellness best practices. Their HR Manager stated that even though they are providing numerous programs, the HR team gets discouraged when they hear what much bigger companies can do in wellness. It’s huge and so they can afford those types of programs. Then we get discouraged because we can’t do all the things that they get to.
This statement suggests that although the roundtables can cause the staff to be discouraged, it is still a worthwhile endeavor because they can benchmark against companies of all sizes and learn new ideas.
Middle-Scoring Organizations
The leaders of organizations in the middle-scoring category had different ways of expressing their commitment to wellness programs. Some organizations use people throughout the company to promote health and wellness, even though it is not specifically their job. For instance, an organization in the 3-D Graphics industry has an office manager who “took care of everything and made sure that everyone was on the same page and everyone was informed” about health and wellness programs. Even though they did not have a specific wellness coordinator, “they make sure to take care of everyone and they always care so much about individual experiences.” The interviewee further explained that the organizational leaders wanted “to ensure that they supported enjoyment level and productivity and efficiency.” An organization in the transportation industry demonstrates similar practices in their culture. They do not have paid employees to run worksite wellness activities, but individuals will voluntarily promote health initiatives. The interviewee stated that, if an employee asks for something, leadership will provide it, even though there is not a lot of promotion. There are various people throughout the company that promote health and wellness on a personal level, but it’s not required for their job. Some of us like to run, we talk about running, encourage others, but I’m not paid to do that.
A separate transportation organization uses a safety person to promote their wellness programs. The transportation supervisor stated that “there is an individual that goes to the different areas and promotes wellness, talks about it, and (listens to) concerns; he’s a safety guy.” Although this sounds promising, an internal wellness volunteer is not necessarily as reliable as a paid position. They can forget, get too busy, or leave the company, and thus, the wellness initiatives live and die with the volunteers.
A middle-scoring organization in the construction industry shared a unique approach to demonstrating top- down leadership commitment to health and wellness. Because all of their employees belong to an employee union, the union takes care of all of the wellness programs for employees. The supervisor explained that “all health programs are union-driven. I don’t think they would provide anything if it wasn’t for the union.” Interestingly, the interviewee stated that employees get to vote on allocating any pay increases they receive. In his words, “The company pays our insurance. We have a package and if we get a raise, it’s up to us to decide where the raise goes; whether to the benefits or on the check.” Further research could solely investigate union companies to see how companies were involved in wellness, in addition to union efforts.
A retail/wholesale trading company demonstrated two CDC HSC line items related to top-down commitment in the interview. Their employee stated that they promote “a monthly group of employees and leaders that meet to discuss topics, including health.” Therefore, if an employee has a complaint or an idea for improvement, they can serve on this monthly, employee committee. This employee shared that the organization’s stated policies are “’to be safe and have fun’ but they were not really adhered to by the company.” They employee also felt that the leadership’s focus on health and wellness is done in the company’s enlightened self-interest. The interviewee said that, almost everything that they do for health and wellness it’s not geared towards helping you personally. The programs are more geared towards keeping you on the shop floor and being able to be functional in your job. Once you left the place they didn’t care if you were smoking two packs a day. At the core it really boils down to two things. One liability, having someone drop on the floor and then two, just your functionality in your position.
From the employees’ point of view, there is a difference between caring for the employees and caring for the company’s bottom-line.
Lowest-Scoring Organizations
The lowest-scoring organizations in the study had four major themes in the sub-category of leadership commitment to health and wellness. An automobile manufacturer is not conducting a lot of wellness activities at the local branch of the company. The local branch is new and the only programs they have are pushed “from corporate” and not necessarily embraced willingly.
Another low-scoring manufacturer does not have formal wellness programs. According to the interviewee, the programs are self-driven by employees. In his words, the company does not really promote programs; walks and exercise are employee driven amongst friends. As a team, my design team, (will say) ‘let’s go out on a walk or let’s all go to the gym together;’ but it’s more as friends. Because we’re all friends there, we just go to the gym, but not as a corporation. A supervisor may encourage it, but it’s more out of his own leadership experience as opposed to the company (promoting it).
In a low-scoring, small organization of seven employees, the owner can clearly see any unhealthy or unsafe practices of the machine and repair shop due to their size. The top- down aspect of their organizational structure is simple, and the owner and manager can be involved in the day-to-day operations. On health issues in the company, the technician shared that, in a small shop like that, with seven people, you can talk to everybody so you may not need a formal survey. He can easily ask questions on “How are you feeling?”, “how’s your health?”, “is your back sore?” He discusses this with everybody, if not daily, once a week to see how everybody is doing.
The leaders of another organization in the lowest- scoring category seem to mostly care about health and safety as it pertains to meeting the letter of the law. Their quality engineer shared that “I think they’re more worried about the bottom line and putting product though the door. Like certain OSHA violations and things like that. They’ll worry about those, but not really about the actual employees’ health.” The interviewee stated that the thinking might change if leadership “could see that it’s an investment, instead of a cost. It’s the same thing with leadership training ... you pay for it today, but you don’t always see the benefit. And you may never be able to put a number on it.” Future research could look at the return on investment of health programs, particularly if employee turnover negates the investments into health when employees leave the company.
An interviewee from the construction industry also elaborated on the viewpoint of the upper management on health expenses being a cost, rather than an investment. The journeyman electrician in this low-scoring category stated that I can easily see how, in the long-term, you can save the company a lot of money, but we’re one of those industries that the turnover rate is so high, that most of these wouldn’t even be able to take effect before we have a whole new line of employees.” He further shared concerns that the views of his colleagues are that everyone is too busy for new health and wellness initiatives. In his words, we don’t have it in the budget or nobody has the time for it simply because it’s such as small company. We are not that far out of a start-up phase where everybody is doing three positions at one time. There is nobody that’s graduated into the, “I don’t have to work that much anymore. Let me focus on those things.” The mentality is that we need “all hands on deck.” The lowest-score organization in the study shared its experience with creating mission statements and organizational goals around health and wellness. The interviewee just crafted a mission statement and goals for an industry certification. He shared that “we’re so young. I just compiled a business statement to get (an industry) certification. It was just a generic statement; it had nothing to do with health. It would be like in your mission statement, you would say, ‘We want to be the healthiest shop.’ ” The interviewee further explained that the organization does not have a strong health culture. He shared that “as far as the company, some people like myself would like to run a 5K around the office. There’s not the top- down support for that type of thing.”
Discussion
The findings from the qualitative questions reveal critical insights into the organizational structures and features that promote healthy behaviors within companies. By benchmarking against the CDC Health Scorecard (HSC) validation study, organizations can identify strengths and areas for improvement in their health promotion programs. This discussion examines the role of leadership, the impact of budgetary constraints, and the cultural aspects that influence the effectiveness of workplace wellness initiatives.
Top-Down Leadership Commitment
The highest-scoring organizations in the study exemplified strong top-down leadership commitment to wellness, which significantly contributed to their success in promoting healthy behaviors. In particular, the industrial manufacturing organization demonstrated how corporate- level support can drive the adoption and integration of wellness programs across various facilities. The consistent emphasis on health initiatives, such as health fairs, fitness centers, and wellness committees, highlights the importance of leadership in fostering a culture of health.
Moreover, the flexibility and support provided by leadership in the educational services industry illustrate how organizational commitment to employee health can offset lower wages, thereby enhancing job satisfaction and retention. These examples underscore that leadership’s active involvement and financial backing are pivotal for the success of wellness programs, as they provide the necessary resources and set the tone for organizational priorities.
Budgetary Constraints and Resource Allocation
Budgetary constraints emerged as a significant challenge, particularly for middle- and low-scoring organizations. While high-scoring companies managed to allocate sufficient resources for wellness initiatives, smaller organizations and those with limited budgets struggled to provide comprehensive programs. For instance, the social services organization highlighted the positive impact of creating a Human Resources Coordinator position, even on a part-time basis, to manage wellness activities. This indicates that even modest investments in dedicated wellness roles can substantially enhance program effectiveness.
Conversely, the educational services organization faced challenges due to its distance from the corporate office, which limited access to centralized wellness resources. This situation exemplifies the difficulties that geographically dispersed organizations might encounter in uniformly implementing wellness programs. Additionally, organizations with limited budgets often rely on voluntary efforts from employees to promote health initiatives, which may not be as reliable or consistent as having dedicated staff.
Organizational Culture and Employee Engagement
The role of organizational culture in supporting wellness programs cannot be overstated. High-scoring organizations often embedded wellness into their corporate values, fostering an environment where health initiatives are seen as integral to the company’s mission. For example, the automobile manufacturer’s goal of achieving high participation rates in health screenings demonstrates a long-term commitment to employee health, reinforced by substantial incentives and paid time for participation. However, cultural challenges were evident in lower-scoring organizations, where health initiatives were either absent or poorly supported. The reliance on self-driven programs among friends, as seen in the small manufacturer, reflects a lack of formal structure and support from management. Additionally, the perception of health expenses as a cost rather than an investment, as noted by the journeyman electrician, highlights a critical barrier to implementing effective wellness programs. Changing this mindset requires demonstrating the long-term benefits and potential cost savings associated with improved employee health.
Implications for Future Research
The findings suggest several implications for future research and practice in workplace wellness programs. Firstly, there is a critical need to explore the long-term return on investment (ROI) of wellness programs, particularly in high-turnover industries, to build a compelling business case for sustained investment in employee health. Additionally, examining the specific elements of organizational culture that most effectively support wellness initiatives could provide valuable insights for companies looking to enhance their programs.
Future research should also investigate the role of union-driven wellness programs, as seen in the construction industry, to understand how these initiatives complement or substitute for employer-led efforts. This could inform strategies for collaborative approaches to workplace health promotion.
Future research should examine health metrics, such as costs, doctor visits, and biometric data, before and after implementing a wellness coordinator. Additionally, investigating industry certifications that include health and wellness components and analyzing participation rates in these certifications could provide valuable insights.
Recommendations for Practice
Based on the findings of this study, several recommendations can be made to enhance the effectiveness of workplace wellness programs through strategic leadership, resource allocation, and cultural support:
- Enhance Top-Down Leadership Commitment: Active Involvement: Leaders should actively participate in wellness initiatives, demonstrating their commitment to employee health. This includes attending health fairs, participating in fitness activities, and engaging with employees about wellness programs. Resource Allocation: Leadership should ensure adequate resources, including financial and human resources, are allocated to support wellness programs. This may involve hiring dedicated wellness coordinators or integrating wellness responsibilities into existing roles.
- Address Budgetary Constraints: Strategic Investment: Organizations should view wellness programs as a strategic investment rather than a cost. Demonstrating wellness initiatives’ long-term return on investment (ROI) can help secure the necessary funding. Leverage External Resources: Smaller organizations can collaborate with local health organizations or participate in community wellness programs to offset costs. Seeking grants or partnerships can also provide additional funding for wellness initiatives.
- Foster a Supportive Organizational Culture: Integration with Corporate Values: Embedding wellness into the corporate culture ensures that health initiatives are seen as integral to the company’s mission.
This includes integrating wellness goals into the company’s core values and strategic objectives.
Promote Employee Engagement: Encourage employee participation through incentives, recognition programs, and creating a supportive environment. Facilitating social interactions and peer support can enhance engagement in wellness activities. 4. Utilize Data and Technology: Data Analytics: Employ data analytics to measure wellness programs’ effectiveness and identify areas for improvement. This includes tracking participation rates, health outcomes, and cost savings. Personalization: Use technology, such as wearable devices and health apps, to provide personalized health interventions tailored to individual needs and preferences. 5. Expand Mental Health Support: Comprehensive Mental Health Programs: Integrate mental health services into existing wellness programs, providing resources such as counseling, stress management workshops, and mental health awareness training. Reduce Stigma: Foster an environment where seeking mental health support is encouraged and stigma is reduced. This can be achieved through leadership support, employee education, and promoting open discussions about mental health [25, 26]. 6. Adapt Programs to Geographic and Demographic Contexts: Regional Considerations: Tailor wellness programs to address the unique challenges and opportunities presented by the geographical and demographic context of the organization. This includes considering access to healthcare facilities, cultural norms, and specific health issues in the region.
- Diverse Workforce: Design wellness programs that cater to the diverse needs of the workforce, including considerations for different educational levels, age groups, and cultural backgrounds.
- By implementing these recommendations, organizations can enhance the effectiveness of their workplace wellness programs’ effectiveness, improving employee health, increased productivity, and reduced healthcare costs. These strategies highlight the critical role of leadership, resource allocation, and organizational culture in fostering a healthy and supportive work environment.
Acknowledgment
The author would like to thank all of the study participants. It could not have been done without their transparency, contribution, and willingness to help.
Funding Details
No funding was received for this project.
Disclosure Statement
There is nothing to disclose.
References
-
(2022) National health expenditures 2021 highlights. Centers for Medicare and Medicaid Services.
-
(2023) Health Care Costs: A Primer. Kaiser Family Foundation.
-
(2023) Consumer Price Index Summary. Bureau of Labor Statistics.
-
(2023) National Survey of Employer-Sponsored Health Plans. Mercer.
-
(2021) Chronic diseases and health promotion. Centers for Disease Control and Prevention.
-
(2019) The business case for wellness: A review of the literature. Health Enhancement Research Organization.
-
(2019) The cost of absenteeism in the U.S. Harvard Business Review.
-
Kessler RC, Barker PR, Colpe LJ, Berglund P, Cleary PD, et al. (2003) The World Health Organization Health and Work Performance Questionnaire (HPQ). Journal of Occupational and Environmental Medicine 45(2): 156- 174.
-
Baicker K, Cutler D, Song Z (2010) Workplace wellness programs can generate savings. Health Affairs 29(2): 304-311.
-
(2021) Workplace mental health: Reducing stress and enhancing well-being. American Psychological Association.
-
(2020) Global health care outlook: Common challenges, common solutions. Deloitte.
-
Goetzel RZ, Ozminkowski RJ (2008) The health and cost benefits of work site health-promotion programs. Annual Review of Public Health 29: 303-323.
-
Berry LL, Mirabito AM, Baun WB (2010) What’s the hard return on employee wellness programs?. Harvard Business Review 88(12): 104-112.
-
Mattke S, Liu H, Caloyeras JP, Huang CY, Van Busum KR, et al. (2013) Workplace wellness programs study: Final report. RAND Corporation.
-
Anderson LM, Quinn TA, Glanz K, Ramirez G, Kahwati LC, et al. (2009) The effectiveness of worksite nutrition and physical activity interventions for controlling employee overweight and obesity: a systematic review. American Journal of Preventive Medicine 37(4): 340-357.
-
Goetzel RZ, Henke RM, Tabrizi M, Pelletier KR, Loeppke R, et al. (2014) Do workplace health promotion (wellness) programs work?. Journal of Occupational and Environmental Medicine 56(9): 927-934.
-
Eisen A, Allen G, Bollash M, Pescatello LS (2008) Stress management in the workplace: A comparison of a computer-based and an in-person stress-management intervention. Computers in Human Behavior 24(2): 486- 496.
-
Chapman LS (2012) Meta-evaluation of worksite health promotion economic return studies: 2012 update. American Journal of Health Promotion 26(4): TAHP1- TAHP12.
-
Anderson GF, Ballreich J, Bleich S, Boyd C, DuGoff E, et al. (2015) Attributes common to programs that successfully treat high-need, high-cost individuals. American Journal of Managed Care 21(11): e597-600.
-
Cutler DM, Lleras-Muney A (2010) Understanding differences in health behaviors by education. Journal of Health Economics 29(1): 1-28.
-
Hartley D (2004) Rural health disparities, population health, and rural culture. American Journal of Public Health 94(10): 1675-1678.
-
(2023) Employer health benefits 2023 annual survey. Kaiser Family Foundation.
-
Liu JJ, Davidson E, Brossart DF, García AM (2020) Health disparities among rural and urban populations in the United States. Journal of Rural Health 36(1): 1-8.
-
Probst JC, Moore CG, Glover SH, Samuels ME (2004) Person and place: the compounding effects of race/ ethnicity and rurality on health. American Journal of Public Health 94(10): 1695-1703.
-
(2023) U.S. employers see biggest healthcare cost jump in decade for 2024. Reuters.
-
(2020) Educational Attainment in the United States: 2020. US Census Bureau.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda