Trends and Causes of Increasing Child Anaemia: Secondary Analysis of NFHS 5 Data- India
National Family Health Survey (NFHS) data of 2019-2020 indicates that prevalence of anaemia among children aged 6-59 months is 67.1%, while among women aged 15-49 years, it is 57%. These figures highlight the significant burden of anaemia in India. This number has increased from 2015-16 to 2019-21. The cause of anaemia can be attributed to two main factors: autonomous factors and induced factors. Furthermore, there are considerable regional disparities in child anaemia within India. The southern part of the country exhibits a lower prevalence of malnutrition in comparison to the northern part. The statistical analysis of 707 districts of India reveals that child malnutrition is influenced by socio-economic, nutritional, and health-related factors. The incidence of anaemia can be passed on to her offspring. While certain socio-economic factors may overlap in both cases, the underlying causes of anaemia differ significantly. This paper provides a comprehensive review of anaemia of children and mothers, covering prevalence, causes, consequences, diagnosis, management, and challenges in prevention. The result suggests for district level policy and targeted interventions to address this critical public health issue.
Sengupta Atanu1, Ghosh Abhijit2* and Mishra Abhijit3
Keywords: Child anaemia; Micronutrient; BMI (Body Mass Index); India; NFHS
Abbreviations
BMI: Body Mass Index; WHO: World Health Organization; CNNS: Comprehensive National Nutrition Survey; GBD: Global Burden of Diseases.
Introduction
Anaemia is a serious health issue affecting children and mothers, having significant implications for their well-being. It may cause irreversible consequences to the affected persons. It is characterized by reduced red blood cells or decreased haemoglobin levels, impairing oxygen transport. Global anaemia prevalence is alarming, affecting an estimated 1.62 billion people or approximately 24.8% of the global population according to the World Health Organization (WHO). This prevalence varies across regions, with higher rates observed in sub-Saharan Africa, South Asia, and parts of Southeast Asia due to limited healthcare access, poor nutrition, and infectious diseases. Disparities exist within populations, with marginalized communities, women, and specific age groups facing higher prevalence. Socioeconomic factors, inadequate nutrition, and gender inequality contribute to these disparities.
Anaemia in children hinders growth, psychomotor development, and cognitive abilities. Iron deficiency anaemia, the most common form, can lead to long-term neurodevelopmental deficits, affecting learning, attention, memory, and behaviour. School-age children with anaemia experience reduced cognitive performance, attendance, and educational achievements, limiting their potential. Anaemia
also impacts psychosocial well-being, motivation, and self-esteem. It increases morbidity and mortality risks by weakening the immune response. Children face higher rates of complications and hospitalizations, while pregnant women have increased risks of adverse outcomes and maternal mortality. The impact anaemia on infections and underlying health conditions contributes to elevated mortality rates, particularly in resource-limited settings.
Addressing anaemia requires targeted strategies considering regional variations and disparities. Interventions should focus on improving healthcare infrastructure, promoting education, ensuring access to nutritious food, and addressing social determinants of health. Early detection, nutritional interventions, and appropriate healthcare access are vital in mitigating the adverse consequences of anaemia and improving overall well-being.
The Comprehensive National Nutrition Survey (CNNS) aims to collect nationally representative data on the nutritional status of pre-schoolers, school-age children, and adolescents through interviews, comprehensive anthropometric measures, and biochemical indicators. It also focuses on identifying the causes of anaemia in children and micronutrient deficiencies in different age groups.
Additionally, the survey examines background characteristics such as the educational attainment of children’s mothers, exposure to mass media, and socioeconomic backgrounds. This wealth of information allows for a greater understanding of the nutritional challenges faced by Indian children. The Global Burden of Diseases (GBD) study revealed that dietary iron deficiency had the most significant impact on disability in India. In 2016, anaemia cost the country approximately Rs. 1.5 lakh crore in GDP losses, as reported by India Spend. According to the CNNS, the prevalence of anaemia among children in India is significant. Approximately 41% of pre-schoolers, 24% of school-age children, and 28% of adolescents were found to be anaemic, with higher rates observed among children under two years of age. In terms of gender disparities, female adolescents had more than double the prevalence of anaemia (40%) compared to male adolescents (18%).
Iron deficiency in infants and young children, especially in developing countries, hinders brain development and has long-term cognitive and motor consequences. Early iron supplementation is crucial to prevent and reverse adverse effects, with prenatal iron deficiency also requiring attention [1].
Anaemia, a significant public health concern, affects approximately two billion individuals globally, particularly women and children [2, 3, 4, 5]. It leads to severe health implications throughout life, including maternal mortality, stunting, impaired cognitive development in children, and reduced work productivity in adults [6, 7, 8].
The rest of the paper is organised as follows. While the first section introduces the paper, the next section depicts the status of anaemia of different states of India. Third section presents the methodology. Findings of the analysis are discussed in the fourth section. Section five concludes the study.
Data Interpretation
In India, anaemia is a major health issue, particularly among children and women. National Family Health Survey (NFHS) data from 2019-2020 indicated that anaemia prevalence among children aged 6-59 months was 67.1%, while among women aged 15-49 years, it was 57%. These figures highlight the significant burden of anaemia in India.
The Comprehensive National Nutrition Survey (CNNS) conducted in India during 2016-2018 is the largest micronutrient survey in the world, focusing on nutritional indicators among children aged 0-4, 5-14, and 15-19 years. It provides crucial context and data on the state of health and nutrition among Indian children.
Radhakrishna R [9], analysing the performance of the states in post-reform period explores the relationship between growth, poverty, and inequality, providing insights for India to expedite poverty reduction initiatives. It indicates huge regional difference among various states of India. Figure 1 clearly shows this disparity.
The data provided shows the prevalence of child anaemia in various states in India. Indeed, the prevalence of anaemia in India is a critical issue that affects a significant portion of the population. The data indicates that out of the 707 districts in India, only 72 districts have a prevalence rate below 50% for anaemia. This highlights the widespread nature of the problem across the country.
Furthermore, it is important to identify the districts that are particularly affected by micronutrient deficiencies such as anaemia. Unfortunately, the specific districts suffering from high levels of anaemia are not mentioned in the provided data. However, it is crucial for policymakers and healthcare authorities to identify these districts and prioritize interventions to address the issue.
The data also indicates that the prevalence of anaemia has increased in some states between the years 2015-16 and 2019-21. This is concerning as it suggests that despite efforts to combat anaemia, certain states are facing challenges in reducing its prevalence. The increasing percentage of anaemia in these states is a cause for concern and indicates the need for renewed efforts and targeted interventions to address the issue effectively.
The subsequent entries show an increasing trend in anaemia prevalence from NFHS-4 to NFHS-5 for various states and union territories. The magnitude of the increase varies across regions, ranging from 2.4% (Arunachal Pradesh) to 32.7% (Assam), while Gujarat experiencing an increase of 17.1%. The states like Rajasthan, Punjab, West Bengal, Maharashtra, and Chhattisgarh registers notable increase in anaemia prevalence, ranging from 11.2% to 25.6%. Mizoram, Manipur, and Jammu & Kashmir have higher increases (18.9%), highlighting the need for targeted interventions in these regions. Nagaland, Odisha, and Tripura also experienced significant increases in anaemia prevalence (16.3% to 19.6%), emphasizing the need for effective strategies to address the issue. Assam had the highest increase of 32.7%, indicating a critical situation and demanding immediate attention to combat anaemia.
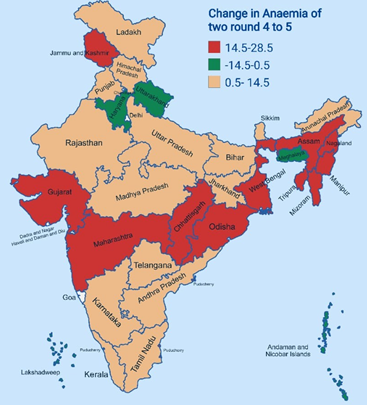
Overall, the data reveals a mixed picture of anaemia prevalence across India. While some regions have shown improvements or slight decreases, several states and union territories have experienced a significant increase in anaemia prevalence. This highlights the urgent need for targeted interventions, improved healthcare infrastructure, and awareness programs to effectively address and reduce anaemia prevalence in these regions. The districts of different states belonging to red colour zone in above India map (Figure 2) implies that percentage of anaemia increases in these districts at an increasing rate than other states (Table 1).
| States | Child anaemia (%) |
|---|---|
| Nagaland | 42.7 |
| Manipur | 42.8 |
| Mizoram | 46.4 |
| Puducherry | 64 |
| Odisha | 64.2 |
| Tripura | 64.3 |
| India | 67.1 |
| Chhattisgarh | 67.2 |
| Assam | 68.4 |
| Maharashtra | 68.9 |
| West Bengal | 69 |
| Jammu & Kashmir | 72.7 |
| Gujarat | 79.7 |
Table 1: Percentage of anaemia increases in the states. Source: NFHS-5
On the other hand, Table 1 shows, all such states Nagaland, Manipur, Mizoram, Puducherry, Odisha, Tripura have lower percentage of Anaemia than that of national level. So, the prevalence of malnutrition is lower in these states.
The states like Chhattisgarh, Assam, Maharashtra, West Bengal, Jammu & Kashmir, Gujarat have experienced increased in the Anaemia from NFHS-4 to 5 with higher percentage than the national level. Let us discuss briefly about these six states.
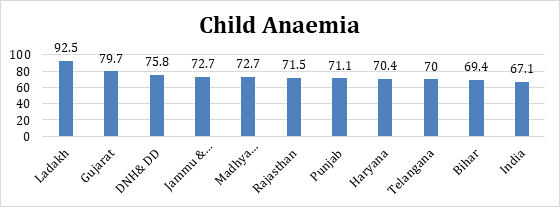
Gujarat records the prevalence of anaemia at 79.7%. This is significantly higher than the national average of 67.1%. Jammu & Kashmir and Madhya Pradesh share the same prevalence rate of 72.7%, indicating a high prevalence of anaemia among children in these states. Rajasthan has a prevalence rate of 71.5%, signifying a significant number of children affected by anaemia in the state. Punjab and Haryana have prevalence rates of 71.1% and 70.4%, respectively, indicating a high burden of anaemia among children in these states. Telangana registers a prevalence rate of 70%, indicating a substantial percentage of children affected by anaemia in the state. Bihar, with a prevalence rate of 69.4%, shows a relatively high burden of anaemia among children in the state.
Among the major states in India, Gujarat has the highest prevalence of anaemia in children aged 6 to 59 months, with approximately 80% of children in that age group being affected by the condition. This indicates a significant burden of anaemia among young children in Gujarat.
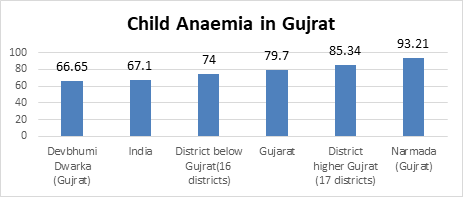
Comparing the NFHS-4 and NFHS-5 data, prevalence of anaemia in Gujarat indicates an increase of 17.1 percentage points. Above figure (Figure 3) shows that, among the districts in Gujarat, sixteen districts have a lower prevalence of child anaemia compared to the state average. However, even in these districts, the prevalence rate of child anaemia remains high at 74%. On the other hand, seventeen districts in Gujarat have an even higher prevalence rate of 85.34% for child anaemia. This prevalence surpasses both the state average and the national average indicating severity of the problem. Among the mentioned districts, Narmada has the highest prevalence rate of child anaemia at 93.21%. Overall, the data highlights the significant challenge of anaemia in Gujarat, with varying prevalence rates among different districts. It underscores the urgent need for targeted interventions, improved healthcare access, and nutrition- focused programs to address and reduce the burden of anaemia among children in the state.
In case of Jammu & Kashmir specifically, the child anaemia rate is higher at 72.7%. However, the average anaemia rate below Jammu & Kashmir is 65.71%, indicating that some regions within the state may have even lower anaemia rates. Higher rates of anaemia in a specific region, particularly in border areas, can indeed be a cause for concern as it suggests a potential health challenges and the need for targeted interventions. Anaemia can have various underlying causes, including nutritional deficiencies, inadequate healthcare infrastructure, limited access to healthcare services, and socioeconomic factors.
| State (Jammu & Kashmir) | Child anaemia |
|---|---|
| Punch (J & K) | 54.27 |
| Shupiyan (J & K) | 57.12 |
| Ramban (J & K) | 62 |
| India | 67.1 |
| Average below J & K | 65.71 |
| Jammu & Kashmir | 72.7 |
| Average above J & K | 80.8 |
| Badgam (J & K) | 85.04 |
| Kishtwar (J & K) | 88.46 |
| Ganderbal (J & K) | 89.76 |
Table 2: The child anaemia rate in Jammu & Kashmir. Source: NFHS-5
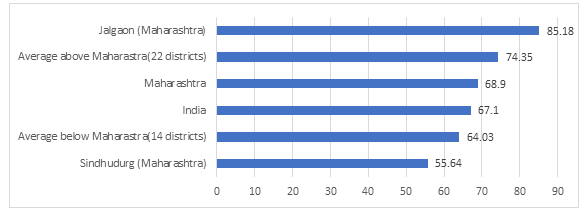
In Maharashtra, anaemia increases from NFHS-4 to NFHS-5. Sindhudurg district in Maharashtra shows a relatively lower prevalence compared to the state average and the national average. This indicates a comparatively better situation in terms of child anaemia in this particular district. There are 14 districts in Maharashtra where the prevalence are below the state average being at 64.03%. This shows that these districts have a higher prevalence of child anaemia compared to Sindhudurg but still below the state average. The prevalence of child anaemia in Maharashtra is slightly higher than the national average, at 68.9%. This suggests that the overall situation in the state is slightly worse than the national average in terms of child anaemia prevalence. There are 22 districts in Maharashtra where the prevalence is above the state average. The prevalence rate is reported at 74.35%, indicating a higher prevalence of child anaemia in these districts compared to both the state and national averages. Jalgaon district in Maharashtra has a significantly higher prevalence (85.18%) in anaemia compared to the state average, the national average, and most other districts in Maharashtra. This indicates a critical situation in terms of child anaemia in this particular district.
The high prevalence of anaemia in West Bengal could be influenced by factors such as inadequate nutrition, limited access to healthcare services, socioeconomic disparities, and cultural practices impacting health and nutrition. The average prevalence of child anaemia in West Bengal is 69%, slightly higher than that of national average. There are ten districts where the average is below the state average, at 65.94%. On the other hand, the average prevalence of child anaemia in 10 districts is above the state average, significantly higher at 73.61%.
| Districts and state of West Bengal | Child anaemia (%) |
|---|---|
| North 24 Pargana (West Bengal) | 57.89 |
| Nadia (West Bengal) | 63.58 |
| Paschim Medinipur (West Bengal) | 65.98 |
| India | 67.1 |
| Average below West Bengal (10 districts) | 65.94 |
| West Bengal | 69 |
| Average above West Bengal (10 districts) | 73.61 |
| Birbhum (West Bengal) | 76.54 |
| Uttar Dinajpur (West Bengal) | 77.21 |
| Purulia (West Bengal) | 77.85 |
Table 4: Child anaemia rate in Districts and state of West Bengal. Source: NFHS-5 In Chhattisgarh, the average is on par with the
This analysis encompasses a comprehensive dataset encompassing 707 districts throughout India. To analyse this vast dataset, three distinct methodologies have been employed: robust regression, tobit regression model, and truncated regression model.
| State Chhattisgarh | Child anaemia (%) |
|---|---|
| Balrampur | 50.08 |
| Surajpur | 51.08 |
| Surguja | 51.35 |
| India | 67.1 |
| Average below Chhattisgarh (11districts) | 57.48 |
| Chhattisgarh | 67.2 |
| Average above Chhattisgarh (16 districts) | 76.91 |
| Narayanpur | 86.82 |
| Dantewada | 89.87 |
| Sukma | 91.4 |
Table 3: Child anaemia rate in Chhattisgarh. Source: NFHS-5
Maternal iron deficiency anaemia poses a significant public health problem in Assam, as highlighted by the study conducted by Goswami BK, et al. [10]. The research emphasizes the adverse outcomes associated with maternal anaemia and its impact on both maternal and child health. There are 12 districts in Assam having anaemia rate below the state average while in 21 districts, the average is above the state level. Comparing with the national average (67.1%), the anaemia rate in Morigaon district is significantly lower. In Kamrup Metropolitan, another district in Assam, the child anaemia rate is reported to be 80.35%, which is significantly higher than both the national and state average. This suggests a serious issue with child anaemia in Kamrup Metropolitan.
| State (Assam) | Child anaemia (%) |
|---|---|
| Morigaon (Assam) | 53.31 |
| Hojai | 56.78 |
| Hailakandi | 59.45 |
| India | 67.1 |
| Average below Assam (12 district) | 62.84 |
| Assam | 68.4 |
| Average above Assam (21 district) | 73.79 |
| West Karbi Anglong | 79.03 |
| Biswanath | 79.84 |
| Kamrup Metropolitan (Assam) | 80.35 |
Table 5: Child anaemia rate in Assam. Source: NFHS-5
Methodology
Regression analysis is employed to examine the relationship between a dependent variable and one or more independent variables. The key objective is to estimate the coefficients of the independent variables, which represent the relationship’s strength and direction. The basic regression model can be expressed as: Y = β0 + β1X1 + β2X2 + ... + βnXn + ε Where:
- Y is the dependent variable (also called the outcome or response variable).
- Β0 is the intercept term, which represents the expected value of Y when all independent variables are zero.
- β1, β2, ..., βn are the coefficients that quantify the relationship between the independent variables (X1, X2, ..., Xn) and the dependent variable (Y).
- X1, X2, ..., Xn are the independent variables (also called predictors or regressors).
- ε is the error term, representing the unexplained variation in Y not accounted for by the independent variables. It captures the random, unpredictable factors affecting Y.
We also use Robustness in the linear regression because robust regression methods provide more reliable estimates when the assumptions of OLS are violated or when there are outliers in the data. However, it’s important to note that robust regression is not a panacea for all regression issues. It is still crucial to carefully interpret the results, evaluate the assumptions, and consider the specific characteristics of the data and research context.
We also use the tobit regression because It is important to note that tobit regression assumes certain assumptions, such as linearity, normality of the error term, and homoscedasticity. Violations of these assumptions can affect the validity of the results. Furthermore, interpretation of tobit regression coefficients can be challenging due to the latent nature of the dependent variable. Careful consideration should be given to the specific characteristics of the data and the research context when using tobit regression analysis. The study examines a tobit regression model with increasing-dimensional covariates, obtaining asymptotic properties of the parameter estimator. Numerical simulations and an application to a dataset demonstrate the strong performance of the proposed estimator [11]. We also regress the observation between low and high anaemia. This will allow us to segregate the effect different variables in a more comprehensive ways.
Findings
A General All India View
Overall Considering child anaemia as dependent variable, we carry out all three regression process, robust regression, tobit regression, and truncated regression. The endeavour is to find out the different aspects of child anaemia. The result is presented in Table 6. The coefficients presented in the regression results indicate the relationship between the independent variables and child anaemia, along with their statistical significance denoted by asterisks (***) and t-values in parentheses.
The R-squared value of 0.53 suggests that the model explains about 53% of the variance in the dependent variable. We can conclude that the model has some predictive power for the dependent variable, and the independent variables included in the model have a significant effect on the dependent variable. All the VIF values are less than 5, which suggests that there is no significant multicollinearity among the independent variables in the model. The mean VIF value of 1.34 (Appendix: Table 1) is also quite low, indicating that the model is relatively stable and the independent variables are not strongly correlated with each other.
| Variables | Regression | Tobit Regression | Truncated Regression |
|---|---|---|---|
| with robust | |||
| Socio-economic variables | |||
| Sex ratio | -0.0468337*** | -.0468337*** | -0.0472174*** |
| (-9.56) | (-9.37) | (-8.98) | |
| Improvement of sanitation | -0.2029361*** | -0.2029361 *** | -0.204621*** |
| (-5.5) | (-5.94) | (-5.9) | |
| Nutritional related Variables | |||
| Adequate diet at birth | -0.1926912** | -0.1926912*** | -0.1932185*** |
| (-3.47) | (-3.71) | (-3.68) | |
| Women BMI less than 18.5 | 0.346648*** | 0.346648 *** | 0.3516071*** |
| -4.37 | -5.2 | -5.2 | |
| Health related Variables | |||
| Severe wasting | 0.4010138*** | 0.4010138*** | 0.4088332*** |
| -4.29 | -4.14 | -4.14 | |
| Diarrhea | 0.2261973* | 0.2261973 * | 0.2314641* |
| -2.24 | -2.31 | -2.31 |
Table 6: Regression analysis (Dependent variable: Child anaemia). Source: NFHS-5, parentheses indicate level of significant.
Three basic variables considered in Table 6 Socio- economic variables, Nutritional related variables and Health related variables are discussed here: Two socio-economic Variables namely sex ratio and the improvement of sanitation is considered: Sex Ratio: The negative coefficient for the sex ratio variable suggests that an increase in the sex ratio (more males relative to females) is associated with a decrease in child anaemia. The coefficient is statistically significant in all three regression models. Improvement of Sanitation: The negative coefficient indicates that an improvement in sanitation is associated with a decrease in child anaemia. The coefficient is statistically significant in both robust and Tobit regression models. Evidence suggests a link between water and sanitation indicators and anaemia. Alongside standard nutrition interventions, promoting policies, practices, and research to enhance access to improved water and sanitation (WASH) should be considered to reduce anaemia prevalence [12, 13].
We also consider two nutritional related variables which are as follows adequate Diet at Birth, Women BMI less than 18.5. Adequate Diet at Birth: The negative coefficient suggests that an adequate diet at birth is associated with a decrease in child anaemia. The coefficient is statistically significant in both Tobit and truncated regression models. Women BMI less than 18.5: The positive coefficient implies that women having a body mass index (BMI) below 18.5 are associated with an increase in child anaemia. The coefficient is statistically significant in all three regression models.
Health-related Variables are: Severe Wasting: The positive coefficient indicates that experiencing severe wasting is associated with an increase in child anaemia. The coefficient is statistically significant in all three regression models. Sustainable socioeconomic improvement and equitable distribution are key to reducing malnutrition, while interventions focusing on enhancing food availability can alleviate hunger, particularly in impoverished communities. [14].
Diarrhoea: The positive coefficient suggests that the variable “diarrhoea” is associated with an increase in child anaemia. The coefficient is statistically significant in both robust and Tobit regression models.
These regression results provide insights into the factors influencing child anaemia. Variables related to socio-economic factors, such as the sex ratio and improvement of sanitation, show a significant association with child anaemia. Nutritional factors, such as an adequate diet at birth and women with a BMI below 18.5, also play a significant role. Additionally, disease-related variables, including severe wasting and Diarrhoea, show significant associations with child anaemia.
But in case of mother’s anaemia Appendix (Table 3), the regression results provide insights into the factors influencing related with it. Socio-economic factors, such as the sex ratio and improvement of sanitation, show a significant association with mother’s anaemia. Additionally, women-related factors, including women getting pregnant at age below 19 and women with a BMI below 18.5, are also significant factors.
Insignificant Variables: The variables “Adequate diet at birth,” “Severe wasting,” and “ Diarrhoea” are reported as insignificant for mother’s anaemia in all three regression models. This means that these variables do not show a statistically significant association with mother’s anaemia in the given analysis. But these are significant for child anaemia, so these variables are called the pure child related variables.
Regional difference in Child Anaemia in India
So far we have considered, India as a whole. However, in order to get a better insights, we will undertake a regional exercise. In this exercise, we choose a few states which have low anaemia and a few states with high anaemia. Regression analysis carried on these two sets will help us to gain more inference about the causes of child anaemia.
First, we consider the differences in child anaemia rates between NFHS-4 and NFHS-5. Then, we rank the states in ascending order based on these differences. From this ranking, we select the states with the lowest child malnutrition rates, which are Lakshadweep, Andaman & Nicobar Islands, Meghalaya, Himachal Pradesh, and Kerala. The second set includes the states with the highest percentage of child anaemia. These states are West Bengal, Maharashtra, Gujarat, and Jammu & Kashmir.
Finally, we analyse district-wise data to compare the regression of child anaemia in high anaemia states with that in low anaemia states. This comparison will help us understand the regional disparities and identify specific areas that require targeted interventions.
| Variables | Regression | Tobit Regression | Truncated Regression |
|---|---|---|---|
| with robust | |||
| Socio-economic variables | |||
| Sex ratio | 0.026085 | 0.0257806 | 0.026304 |
| -1 | (-1.08) | -1.03 | |
| Improvement of sanitation | -0.7911793* | -0.7904791** | -0.7922936*** |
| (-2.21) | (-2.82) | (-3.08) | |
| Nutritional related Variables | |||
| Adequate diet at birth | -0.0851896 | -0.1088479 | -0.0851896 |
| (-0.44) | (-0.61) | (-0.45) | |
| Women BMI less than 18.5 | 10539253** | 1.580013** | 1.539253** |
| -2.84 | -2.74 | -2.49 | |
| Health related Variables | |||
| Severe wasting | 0.9090364 | 0.9025502 | 0.9090364 |
| -0.94 | -0.87 | -0.81 | |
| Diarrhoea | -0.2580223 | -0.2261973 | -0.2580223 |
| (-0.46) | (-0.41) | (-0.34) |
Table 7: Regression Analysis of Low anaemia states. Source: NFHS-5, parentheses indicate level of significant.
| Variables | Regression | Tobit Regression | Truncated Regression | |
|---|---|---|---|---|
| with robust | ||||
| Socio-economic variables | ||||
| Sex ratio | -0.0118673 | -0.0116143 | -0.0118399 | |
| (-1.00) | (-0.63) | (-0.67) | ||
| Improvement of sanitation | -0.1526589* | -0.150162* | -0.1539078* | |
| (-1.97) | (-2.12) | (-2.18) | ||
| Nutritional related Variables | ||||
| Adequate diet at birth | -0.1360176 | -0.13382 | -0.13658 | |
| (-1.56) | (-1.32) | (-1.36) | ||
| Women BMI less than 18.5 | 0.199769* | 0.2035966* | 0.2007447* | |
| -1.87 | -2 | -1.98 | ||
| Health related Variables | ||||
| Severe wasting | 0.2605856 | 0.2653375 | 0.262271 | |
| -1.46 | -1.47 | -1.45 | ||
| Diarrhoea | -0.243492 | -0.022106 | -0.02452 | |
| (-0.13) | (-0.12) | (-0.13) |
Table 8: Regression analysis of high High anaemia states. Source: NFHS-5, parentheses indicate level of significant.
The above two tables 7 and 8 clearly indicates that the most crucial variable affecting child malnutrition is the improvement of sanitation facilities. In both the low and the high anaemia states, improved sanitation facility reduces the preponderance of anaemia. This clearly indicates the need of a strong public action in the field of sanitation. There is a significant disparity among the states, with wealthier regions having better access to improved sanitation facilities compared to the poorer regions. Consequently, the states with better sanitation infrastructure have lower rates of child malnutrition.
Another factor emerged important is the women with low BMI. In both the low and the high anaemia states, the percentage women with low BMI increase the chances of anaemia in that states. In this way, mother health is related to the child health. In a significant way thus, maternal health and child health are closely related. This paper brings out this relation.
Conclusion
This paper highlights the critical issue of anaemia in India, which has increased from the NFHS-4 to NFHS-5 rounds. The states of Nagaland, Manipur, Mizoram, Puducherry, Odisha, and Tripura have witnessed an increase in anaemia rates above 15% in both rounds, but their rates remain below the national level. However, states such as Chhattisgarh, Assam, Maharashtra, West Bengal, Jammu & Kashmir, and Gujarat have experienced an increase in anaemia above 15%, with their rates surpassing the national level. Consequently, these states are facing more severe challenges than others.
Furthermore, findings indicate that the child malnutrition is influenced by various socio-economic, nutritional, and health-related factors. All these factors play a significant role in child anaemia. However, some factors are significant, specifically, the variables, Adequate diet at birth, Severe wasting, and Diarrhoea being insignificant for mother’s anaemia in all three regression models. Nonetheless, they remain significant for child anaemia, making them what we refer to as “pure child-related variables”. Women who become pregnant before the age of 19 have been identified as a significant factor of women’s anaemia, whereas not being a factor in the case of child anaemia. It is a well-known fact that a woman’s anaemia can be transferred to her offspring. While some socio-economic factors may be similar in both cases, the root causes of anaemia differ significantly.
In summary, the paper underscores the alarming prevalence of anaemia in India and highlights the varying factors contributing to anaemia in mothers and children. The study by Kapur D, et al. [15] emphasizes the importance of addressing maternal anaemia as a crucial step in preventing under nutrition in future generations. The researchers highlight that the adverse effects of maternal anaemia on fatal development and growth persist beyond infancy and continue to affect the child throughout childhood, adolescence, and adulthood. Maternal anaemia contributes to intergenerational cycle of poor growth in the offspring. [16].
The findings of the study conducted by Dhaded SM, et al. [17] highlight the need for increased investment and targeted interventions to address micronutrient deficiencies among children, particularly in regions with a higher prevalence of anaemia. The research emphasizes the importance of adopting differential approaches based on regional variations and specific nutritional needs. According to Osorio MM [18] urgent implementation of comprehensive measures, including nutritional education is necessary to address iron-deficiency anaemia. Priority should be given to children under 2 years old and those in rural and deprived areas.
Therefore, this calls for a war footing initiatives to address this problem. In an important study Dreze J, et al. [19] has stated the importance of ICDS institution in mitigating the problem of malnutrition and anaemia. In this work, they have argued that the efficacy of ICDS centre and Anganwadi are very much dependent on the function of local government such as Panchayati Raj Institution, Municipality. People’s participation in development process ensures the proper function of ICDS centre in mitigating the problem of anaemia. The adequate fund needs to be allocated at the ground level. The region-specific policy is required to be framed with a special emphasis on the generation of consciousness. Local level administration such as Panchayati Raj Institution, Municipality with a participatory approached can make a dent in the problem.
References
-
Lozoff B (2007) Iron deficiency and child development. Food and nutrition bulletin 28 (4_suppl4): S560-S571.
-
De Benoist B, Cogswell M, Egli I, McLean E (2008) Worldwide prevalence of anaemia 1993-2005; WHO Global Database of anaemia.
-
Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, et al. (2014) A systematic analysis of global anemia burden from 1990 to 2010. Blood, the Journal of the American Society of Hematology 123(5): 615-624.
-
Mujica-Coopman MF, Brito A, López de Romaña D, Ríos- Castillo I, Cori H, et al. (2015) Prevalence of anemia in Latin America and the Caribbean. Food and nutrition bulletin 36(2): S119-S128.
-
World Health Organization (2015) World health statistics 2015. World Health Organization.
-
Balarajan Y, Ramakrishnan U, Özaltin E, Shankar AH, Subramanian SV (2011) Anaemia in low-income and middle-income countries. The lancet 378(9809): 2123- 2135.
-
Rahman MM, Abe SK, Rahman MS, Kanda M, Narita S, et al. (2016) Maternal anemia and risk of adverse birth and health outcomes in low-and middle-income countries: systematic review and meta-analysis, 2. The American journal of clinical nutrition 103(2): 495-504.
-
Larsen DA, Grisham T, Slawsky E, Narine L (2017) An individual-level meta-analysis assessing the impact of community-level sanitation access on child stunting, anemia, and diarrhea: Evidence from DHS and MICS surveys. PLoS neglected tropical diseases 11(6): e0005591.
-
Radhakrishna R (2015) Well-being, inequality, poverty and pathways out of poverty in India. Economic and Political Weekly 50(41): 59-71.
-
Goswami BK, Hazarika NC, Sarkar A (2018) Maternal iron deficiency anaemia: An important public health problem in Assam. Journal of Obstetrics and Gynecology of India 68(6): 492-498.
-
Ding H, Wang Z, Wu Y (2017) Tobit regression model with parameters of increasing dimensions. Statistics & Probability Letters 120: 1-7.
-
Kothari MT, Coile A, Huestis A, Pullum T, Garrett D, et al. (2019) Exploring associations between water, sanitation, and anemia through 47 nationally representative demographic and health surveys. Annals of the New York Academy of Sciences 1450(1): 249-267.
-
Baldi AJ, Clucas D, Pasricha SR (2020) Anemia and water, sanitation, and hygiene (WASH)—is there really a link?. The American Journal of Clinical Nutrition 112(5): 1145- 1146.
-
Ekholuenetale M, Tudeme G, Onikan A, Ekholuenetale CE (2020) Socioeconomic inequalities in hidden hunger, undernutrition, and overweight among under-five children in 35 sub-Saharan Africa countries. Journal of the Egyptian Public Health Association 95: 09.
-
Kapur D, Agarwal KN (2011) Maternal anaemia contributes to the intergenerational cycle of poor growth in offspring. Indian Journal of Medical Research 133(5): 493-494.
-
Kalaivani K (2009) Prevalence & consequences of anaemia in pregnancy. Indian Journal of Medical Research 130(5): 627-633.
-
Dhaded SM, Somannavar MS (2019) Addressing micronutrient deficiencies among children: Differential approaches for regions with higher prevalence of anaemia. Indian Pediatrics 56(8): 671-676.
-
Osório MM (2002) Determinant factors of anemia in children. J Pediatr (Rio J) 78(4): 269-278.
-
Dreze J, Sen A (2013) An Uncertain Glory: India and Its Contradictions. Economic & Finance. Princeton University Press.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda