The Impact of Caring for People with Spinal Cord Injury (SCI) on Carer’s Subjective Well-Being and Physical Health: A Realist Synthesis Review
<p style="text-align: justify;">Objective: To identify and summarise studies of the psychological well-being of informal carers of people with spinal cord injury. Design: The review included studies if they reported the carers perspective of care giving – studies that focused mostly on the person with spinal cord injury were included only if the carers perspective of the caregiver role could be extracted. Data sources: Electronic searches of MEDLINE, CINAHL, Psych Info, Sociological Abstracts and The Cochrane Library were carried out between December 2013 and February 2015, with update searches undertaken in October 2016. Review methods: A realist synthesis approach was adopted to evaluate studies according to their contribution and drew together evidence from a range of methodologies, including qualitative and quantitative studies. Findings: 28 studies met the inclusion criteria. Nineteen studies focused only on the caregiver (quantitative studies = 13; qualitative studies = 5 and 1 mixed method approach) and four included caregivers and the person with a SCI (quantitative studies=2; qualitative=1 and 1 mixed method approach). Three papers used non care giving age matched comparative approaches. The majority of the studies were conducted in the USA (11), with three from the UK, 2 from Australia and 3 from Brazil. The remainder of studies were international and comprised 1 from China, 1 from Turkey, 1 from the Netherlands, 1 from Canada, 1 from Denmark, 1 from Fiji and 1 from Iran. The total number of SCI carers was 1772; the majority were female (ranging from 88 % to 100% of the samples included) with an age range average (where this has been calculable) of 43.6 Common methodological limitations of studies included in this review were a lack of non-carer age-matched comparison groups, focus on the experience of female caregivers, small sample sizes, and failure to follow up caregivers longitudinally. Several studies provided estimates of the prevalence of subjective well-being and physical health distress among caregivers but no conclusions could be drawn from the current evidence base. The review suggests that many factors are related to caregiver subjective well-being including caregiver attributes, the severity of the spinal cord injury, the relationship dynamics between the carer and the spinal injured individual and objective and subjective assessments of the burden of care. The perceived adequacy of support also emerges as an important aspect with perceived positive and potentially negative impacts on the carer.</p> <p style="text-align: justify;">Conclusion: Further studies are needed to clarify the prevalence of SCI caregivers’ subjective well-being and situation specific factors that predict poorer carer health outcomes. This work will enable appropriate interventions to be developed and evaluated. What is already known about this topic?</p> <p style="text-align: justify;"> Emphasis has been increasingly placed on the delivery of care to patients with SCI in the community and this approach places increased care responsibilities on informal carers.</p> <p style="text-align: justify;"> General carer literature indicates that providing care is associated with poorer psychological health outcomes.</p> <p style="text-align: justify;">What this paper adds</p> <p style="text-align: justify;"> Although from small studies with methodological limitations there is evidence to suggest that providing informal SCI care is stressful.</p> <p style="text-align: justify;"> A number of factors are associated with carer subjective well-being including lack of professional support.</p> <p style="text-align: justify;"> Rigorous, longitudinal studies using age-matched comparative controls are needed to develop and evaluate interventions for this population.</p>
Introduction
Spinal Cord Injury (SCI) often results in physical limitations such that receiving assistance from others is critical to maintaining health and facilitating full societal integration. In the general population, almost 70% of people with SCI receive some form of assistance and support from family members. Similarly, the availability of family care giving is crucial to most individuals with SCI, but there is little research addressing this topic and no appropriate and available method to comprehensively assess the strengths of and burdens on family caregivers. In recent years emphasis has been increasingly placed on delivery of care to patients with SCI in the community. With this approach increased care responsibilities are placed on the families who are required to carry greater care burdens for longer periods of time. Caregiver burden reflects the extent to which a carer perceives their emotional health, physical health, social life and financial status have been affected as a result of caring for a friend or relative [1, 2, 3, 4]. The terminology used to define a ‘carer’ is ambiguous [5]. The term ‘informal caregiver’ is often used to refer to a person who is providing care but is not a health care professional and is unpaid, however, it has been argued that the provision of care by ‘informal’ carers is formal in everything but the receipt of pay [6]. In the UK, the term ‘carer’ has been adopted by the Department of Health (2006) [7] to demarcate the care provided by family or friends from the care provided by health and social professionals. Carers themselves, in particular spouses, do not refer to the notion of being a carer of a caregiver, often describing the experience as an extension of their loving role and commitment to the person requiring support [8, 9]. As such, this article uses the terms synonymously and ‘carer’, ‘caregiver’ are used interchangeably dependent upon how the original authors used the term. Despite the growing numbers of SCI caregivers and potentially high burden, little is known about the effect the SCI has on the care givers psychological well-being. It has been estimated that between 40% and 70% of caregivers have clinically significant symptoms of depression [4]. A meta-analysis of 84 studies indicate that carers had significantly higher levels of depression and stress and lower levels of general subjective well-being than non-carers [10]. In that review, spousal care giving was particularly stressful, as there were large differences in the levels of depression and stress of carers who were spouses compared to non-carers. In addition, caregiver strain is associated with a mortality risk that is 63% higher than no care giving comparisons [11]. Previous reviews have focused on information needs and interventions designed to meet the needs of carers [12, 13, 14] and the general impact of providing care to a person with SCI [15, 16] but there appears to be little evidence of the information and support needs specific to SCI caregivers, and only one study of interventions designed to meet these needs in the form of Brief Problem-Solving Training for family carers immediately post rehabilitation [17] was identified. However, prior to the development of interventions designed to help SCI carers in their care giving role, greater understanding of the psychological impact of the provision of informal care
- Nursing & Healthcare International Journal
- · Refine the purpose of the review by mapping the territory
- · Articulate key theories to be explored and formalise the model
- Step 2: Search for evidence
- · Exploratory search of the literature
- · Progressive focusing to identify key area; refining inclusion criteria in light of emerging data
- · Purposive sampling to test a defined subset of theories with additional snowball sampling to explore new hypotheses as they emerge
- · Final search for additional studies when the review is near completion
- Step 3: Appraise primary studies
- · Use judgement to supplement formal critical appraisal checklist an consider relevance and rigour
- Step 4: Data Extraction
- · Develop data extraction forms and notation devices
- · Extract different data from different studies to populate evaluative framework with evidence
- Step 5: Synthesise evidence and draw conclusions
- · Synthesise data to achievement refinement of theory
- · Allow purpose of review to drive the synthesis process
- · Use ‘contradictory’ evidence to generate insights about the influence of context
- · Present conclusions as a series of contextualised points
- Step 6: Disseminate, Implement and Evaluate
- · Draft and test out recommendations and conclusions with key stakeholders
Table 1: The steps in this realist review were adopted
Steps adopted (Adapted from Pawson& Boaz, 2004)
Step 1: Clarify Scope
· Identify the review question including the nature and content of the intervention and its use
Inclusion Criteria
All study designs were included in the review including qualitative research studies, randomised controlled trials, quasi-experimental designs, observational and descriptive studies. Studies were included if they reported the carers perspective on care giving – studies that focused mainly on the person with SCI were included only if the carers perspective of the caregiver role could be extracted. Studies were included in which participants were identified as the caregiver of a person with SCI and 18 years or older. Studies of all SCI severity levels alongside longevity of the caring relationship were included as were Nursing & Healthcare International Journal
those studies that included participants with different diagnoses providing details specific to the SCI group could be extracted. Studies were excluded if they were not published in English. Further exclusions included papers that presented data collected from caregivers only relating to their views regarding the patient’s condition and care experience and did not reflect the caregivers’ views about providing care.
Search Methods
Search strategies were designed using broad-based terms and no year constraints. Search terms included: carer OR caregiver AND SCI (or tetraplegia, paraplegia). Electronic searches of MEDLINE, CINAHL, Psych info, Sociological Abstracts and the Cochrane Library were carried out between December 2015 and February 2016.A full text copy of an article was obtained if the study appeared to meet the following criteria:
i. Individuals with SCI ii. Carers experiences as expressed by the carer iii. Primary research- including quantitative and qualitative designs Electronic searches were supplemented by citation tracking of reference lists from papers meeting the study’s inclusion criteria. Documents were excluded if they were theses or if their sole focus was patient or health care professionals’ views of carer issues. Gray literature searches of conference proceedings, research reports, book chapters, dissertations and spinal injury organisations web sites were undertaken but yielded no further evidence regarding the research aim.
Search Outcome
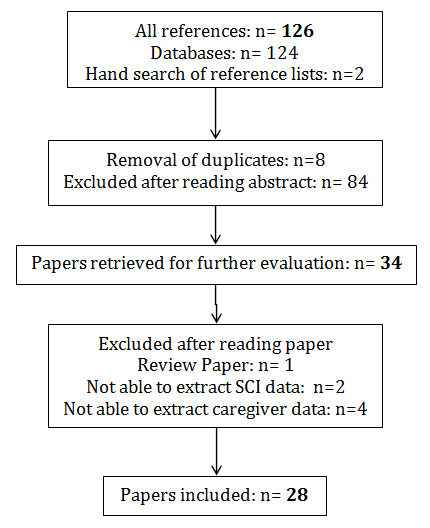
Over 1230 papers were retrieved, with 220 being read in full, and 94 eliminated on second review. The total number of references retrieved by combining the search results was 126 and 28studies met the final inclusion criteria (Figure 1).
Quality assessment and appraisal: Evaluating the quality of the articles and quality appraisal to determine methodological rigour (e.g., sample size, statistical power, presence and strength of the comparison group, use of sound outcome measures, recruitment of the sample) was undertaken using Derish and Annesley’s (2011) [25] criteria. Essentially this comprised critical evaluation of (i) key results, (ii) limitations, (iii) suitability of the methods used to test the initial hypothesis, (iv) quality of the results obtained, (v) interpretation of the results and (vi) impact of the conclusions. As such articles are not graded but thorough appraisal pertaining to the above constructs was adhered to. The Qualitative Research Quality Checklist [26] (Table 2) is a 25 point quality appraisal form designed to evaluate credibility, dependability, confirmability, transferability, authenticity, and relevance of qualitative studies. The QRQC is a guide which facilitates the interpretive curiosity and as such rating scales per se are not implemented. As such, qualitative studies were appraised in terms of their epistemological and theoretical frameworks, study setting, study design, sampling procedures, data collection, ethical issues, reflexivity of the researcher, data analysis, and reporting of the findings. Each item was Nursing & Healthcare International Journal
assigned two ratings: “applicable: and “addressed” each of which consisted of three possible elements (yes, no, unclear). Due to differences in epistemological and ontological stance, not all elements of the QRQC are “applicable” to qualitative studies. Therefore, the QRQC includes three columns for each element. The first column indicates whether the element is relevant to the particular study. Determination of applicability was based on (i) what the author stated they did, and (ii) their epistemological paradigm. For instance, if the author declared they were from a positivist paradigm, it was assumed a reflexive journal would not be part of their process. The appropriateness of the research design was also considered against the author’s epistemological paradigm. The second column indicates whether there is sufficient information in the study for the reviewer to assess whether the specific element has been “addressed”. A third column as also available as a space for the reviewer to comment generally upon the study and/or the qualitative element being addressed. The quality appraisal was conducted on a case-by-case basis during the literature search, extraction, and synthesis process. No papers were excluded in respect of quality because of the dearth of literature meeting the inclusion/exclusion criteria. The quality of the review was maintained by maintaining quality measures in the research process the author adopted.
| Chen | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| De- | |||||||||||||||||||||||||||||
| & | Dickson | Angel & | Dickson | Lucke | |||||||||||||||||||||||||
| Sub- | Lucke et al., | Santo- | Beauregard& | ||||||||||||||||||||||||||
| Question | Boore | et al. | Buus | et al. | et al. | ||||||||||||||||||||||||
| question | -2004 MM | Madeya - | Noreau (2010) | ||||||||||||||||||||||||||
| -2009 | (2010) | (2011) | (2012) | (2013) | |||||||||||||||||||||||||
| 2006 | |||||||||||||||||||||||||||||
| MM | |||||||||||||||||||||||||||||
| Is the purpose and research question clearly stated? | R SI C | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | ||||||||||||||||||||
| Is a qualitative approach appropriate to answer the research question? | R SI C | Y Y Y | Y Y Y | Y Y Y | U U U | Y Y Y | Y Y Y | Y Y Y | Y Y Y | ||||||||||||||||||||
| Is the setting of the study appropriate and specific for exploring the question? | R SI C | Y Y Y | Y Y Y | Y Y Y | Y U U | Y Y Y | Y Y Y | Y Y Y | Y Y Y | ||||||||||||||||||||
| Is there prolonged engagement to render the inquirer open to multiple influences? | R SI C | U U U | U U U | U Y Y | U U U | U U U | U U U | U U U | U U U | ||||||||||||||||||||
| Is there persistent observation in the setting to focus on the issues relevant to the question? | R SI C | U U U | U U U | U U U | U U U | U U U | U U U | U U U | U U U | ||||||||||||||||||||
| Is there compatibility between research question, method chosen, and research design? | R SI C | Y Y Y | Y Y Y | Y Y Y | U U U | Y Y Y | Y Y Y | Y Y Y | Y Y Y | ||||||||||||||||||||
| Is the process of sample selection adequately described and consistent with research design/question? | R SI C | Y Y Y | Y Y Y | Y U U | Y Y Y | Y Y Y | Y Y Y | U U U | Y Y Y | ||||||||||||||||||||
| Is the sample size and composition justified and appropriate for the method/design/question? | R SI C | U U U | Y Y Y | U U U | U U U | Y Y Y | U U U | U U U | U U U | ||||||||||||||||||||
| Are the methods for data collection consistent with the research question? | R SI C | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | ||||||||||||||||||||
| Are the methods of data collection consistent with the methods/design/question? | R SI C | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | Y Y Y | ||||||||||||||||||||
| Is a range of methods used for triangulation? | R SI C | Y Y Y | N N N | Y Y Y | N N N | N N N | N N N | N N N | Y Y Y | ||||||||||||||||||||
| Is there an articulation of who collected the data, when the data was collected, and who analysed the data? | R SI C | U U U | Y Y Y | Y U U | U U U | Y Y Y | Y Y Y | Y Y Y | Y Y Y | ||||||||||||||||||||
| Is there an audit trail regarding data collection, including tapes, | R SI | U U | U N | U U | U U | Y Y | Y Y | Y Y | U U |
| C | U | U | U | U | Y | Y | Y | U | |
|---|---|---|---|---|---|---|---|---|---|
| Is there adequate consideration of ethical issues? | R | U | Y | Y | Y | Y | Y | Y | Y |
| Is there adequate consideration of ethical issues? | SI | U | U | U | Y | Y | Y | Y | Y |
| Is there adequate consideration of ethical issues? | C | U | U | U | Y | Y | Y | Y | Y |
| Has the researcher identified potential and actual biases (researcher and research design?) | R | U | U | N | N | U | N | N | N |
| Has the researcher identified potential and actual biases (researcher and research design?) | SI | U | U | N | N | U | N | N | N |
| Has the researcher identified potential and actual biases (researcher and research design?) | C | U | U | N | N | U | N | N | N |
| Did the researcher(s) use a reflective journal in the analysis and interpretation? | R | N | U | U | N | U | N | Y | N |
| Did the researcher(s) use a reflective journal in the analysis and interpretation? | SI | N | U | U | N | U | N | Y | N |
| Did the researcher(s) use a reflective journal in the analysis and interpretation? | C | N | U | U | N | U | N | Y | N |
| Is the process of data analysis presented with sufficient detail and depth to provide insight into meanings and perceptions of the sample? | R | Y | Y | Y | U | Y | Y | Y | Y |
| Is the process of data analysis presented with sufficient detail and depth to provide insight into meanings and perceptions of the sample? | SI | Y | Y | Y | U | Y | Y | Y | Y |
| Is the process of data analysis presented with sufficient detail and depth to provide insight into meanings and perceptions of the sample? | C | Y | Y | Y | U | Y | Y | Y | Y |
| Are quotes used to match concepts and themes derived from the raw data | R | Y | Y | Y | Y | Y | Y | Y | Y |
| Are quotes used to match concepts and themes derived from the raw data | SI | Y | Y | Y | Y | Y | Y | Y | Y |
| Are quotes used to match concepts and themes derived from the raw data | C | Y | Y | Y | Y | Y | Y | Y | Y |
| Do the findings emerge from the experience of the sample? | R | Y | Y | Y | Y | Y | Y | Y | Y |
| Do the findings emerge from the experience of the sample? | SI | Y | Y | Y | Y | Y | Y | Y | Y |
| Do the findings emerge from the experience of the sample? | C | Y | Y | Y | Y | Y | Y | Y | Y |
| Was member checking employed? | R | N | U | N | N | U | N | N | Y |
| Was member checking employed? | SI | N | U | N | N | U | N | N | Y |
| Was member checking employed? | C | N | U | N | N | U | N | N | Y |
| Did the researcher provide a “thick description” of the sample and results to appraise transferability? | R | Y | Y | Y | N | Y | Y | N | Y |
| Did the researcher provide a “thick description” of the sample and results to appraise transferability? | SI | Y | Y | Y | N | Y | Y | N | Y |
| Did the researcher provide a “thick description” of the sample and results to appraise transferability? | C | Y | Y | Y | N | Y | Y | N | Y |
Table 3: The Qualitative Research Quality Checklist.
Types of Studies Included in the Review
28 studies met the inclusion criteria (Table 3). Nineteen studies focused only on the caregiver qualitative=1 and 1 mixed method approach). Three studies used a non-care giving age matched comparative group [1, 2, 3]. The majority of the studies were conducted in the USA (11), with three from the UK, 2 from Australia and 3 from Brazil. The remainder of studies were international and comprised 1 from China, 1 from Turkey, (quantitative studies = 13; qualitative studies = 5 and 1 mixed method approach) and four included caregivers and the person with a SCI (quantitative studies=2;
1 from the Netherlands, 1 from Canada, 1 from Denmark, 1 from Fiji and 1 from Iran (Table 3). The total number of SCI carers was 1772; the majority were female (ranging from88 % to 100% of the samples included) with an age range average (where this has been calculable) of 43.6.
| Authors & | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample | Test | Design | Results | Conclusions | |||||||||||||
| Year | |||||||||||||||||
| Weitzenka mp, et al. 1997 UK | One hundred twenty-four spouses of a longitudinally followed sample of SCI survivors, all of whom had been injured 23 or more years when the study was conducted in 1993 | CES-D; PSS, LSI-Z and responses to survey questions. | Survey, including demographics, health concerns questionnaire, alongside Administration of the Center for Epidemiologic Studies Depression Scale (CES-D), the Perceived Stress Scale (PSS), the Life Satisfaction | Spouses had more depressive affect (p < .001) than their partners with disabilities, as measured by the CES- D. On the PSS, they exhibited no significant differences. Compared with spouses who were not caregivers, the care giving spouses reported more physical stress (p = .005), emotional stress (p = .011), burnout (p = .007), fatigue (p = .002), and anger and resentment (p = .029). On the CES-D, they had more symptoms of depressive affect (p = .004) and somatic depression (p = .005). | Spouses of long-term SCI survivors who fulfill a care giving role report more symptoms of stress and depression than their partners with disabilities and other spouses who are not caregivers. |
Nursing & Healthcare International Journal
Index (LSI-Z), and the Quality
of Life and Individual
Needs Questionnaire
11 male and 55 female caregivers Design: Correlational methods were used to test the were matched with data from 38 men and 18 Acceptance of Disability Scale score and pressure Elliott et al., 1999 USA women with recent spinal cord injuries.
sore diagnosis hypothesis.
Coping strategies,
depression, care- giving burden, life satisfaction and marital adjustment.
Levenson’s Internality, Powerful Others, and Chance Scale (LIPC) Provision of Social Relationship A cross- sectional correlation design. A set of (PSR) Ways of Coping Checklist Chan, 2000 Forty spouses of persons with SCI structured questionnaires China (WOC) Beck Depression Inventory (BDI) Satisfaction with and semi- structured interviews were Life Situation (SWLS) Katz’s Adjustment Scale – administered.
Relative Forms 2
and 3 (KASR) Caregiver Burden
Inventory (CBI) Dyadic Adjustment
Scale (DAS)
To compare the
quality of life scores of primary caregivers of spinal cord injury survivors living in the community with Fifty primary caregivers of healthy age spinal cord injured patients matched- population based controls Unalan et SF-36 (short form- living in the community and 40 healthy age- al., 2001
36) questionnaire and to determine the Turkey
forms.
matched population based-controls.
relationship between some severity parameters related with spinal cord injury and the quality of life scores of primary caregivers.
Caregiver characteristics
Caregiver tendencies to impulsively and carelessly solve problems were associated with lower acceptance of are associated with the adjustment of persons with SCI and warrant consideration in terms of disability and were significantly predictive of pressure sore diagnosis psychological interventions and health among those returning for a medical evaluation 1 year later.
policy The identification of the
The most stressful situations concerned health issues of their injured partners, the family and marital interactions, and the care- potential at-risk group indicates that spouses of persons with SCI suffer levels of stress comparable giving burden imposed on them. Cluster analysis indicated a potential to those of their injured partners. Rehabilitation plans should include this potential at-risk group to at-risk group, characterized by high scores in external locus of control, inadequate coping modes and limited help them release the stress and to prevent them social support. They were noted to manifest high levels of depression, care-giving burden, low levels of life satisfaction and marital adjustment.
from developing clinically significant mental disorders.
Quality of life scores measured by SF-
36 were significantly low in the primary caregivers group compared Being a primary caregiver significantly interferes with quality of life; some to age-matched healthy population based controls. No significant relation was demonstrated between severity parameters related to the injury however do not seem to have an additional impact on the primary caregiver's the quality of life scores of primary caregivers and parameters such as the duration of injury, lesion levels, ASIA scores, degree of spasticity, bladder and/or bowel incontinence life quality.
and pressure sores respectively
Nursing & Healthcare International Journal
this mixed method, descriptive, longitudinal SF-36 and two horizontal visual analog scales, one for pain and one for feasibility (pilot) study was to describe A convenience sample of 12 SCI participants and Lucke et al., 2004 QOL and a face-to- and compare QOL in 10 adult face in-depth interview at 1-, 3-, USA their FCs SCI individuals and their family caregivers (FCs) and 6-months following inpatient rehabilitation.
during the initial 6 months following rehabilitation.
Cross-sectional survey. Burden of support was measured by a Physical disability of All members of the person with SCI was measured using the Dutch six-item measure (Cronbach’s alpha 0.92), Mean age of the patients organisation DON the Barthel Index (BI). A number of (N¼1004) and their caregivers, secondary conditions, other practical problems Post et al., if applicable, were invited. Responses were partners was 49.4 years (SD 12.2) and 69.8%
2005 Netherland
and psychosocial problems were recorded. Partner
s obtained from 461 persons with were women. Mean BI of the support was described using a list of ADL support, SCI. Of 265 couples, patient as well as partner persons with SCI was12.3 (SD other practical
4.7) on a 0–20 scale and 60.4%
data were support and emotional support.
available.
were seriously disabled (BIo15).
This comprised a
one-page spinal cord injury questionnaire (SCIQ) designed to collect information from the individual Descriptive survey conducted with with SCI, and a family caregiver The survey collected social
154 family caregivers nominated by SCI
questionnaire (FCGQ) for completion by his or Foster et and demographic information and al., 2005 Australia respondents and her family caregiver. The FCGQ an additional 25 family caregivers details of the comprised four sections: socio- type of care provided by demographic family caregivers information; description of family care giving, additional care provided by others;
and services required SCI individuals reported low physical function, role physical (RP), and role emotional (RE) scores on the SF-36, suggests that more work is while reporting high general health needed to identify interventions which could (GH), mental health and social functioning on the SF-36. FCs reported lower RP, GH and vitality enhance QOL during the transition from rehabilitation to home for scores, while reporting higher physical functioning and RE scores. On the visual analog scales, persons SCI individuals and their FCs. individuals and their with SCI reported lower QOL while FCs.
FCs reported more pain at 3 and 6
months.
Nonparametric descriptive statistics
and correlations were used. Linear
regression was used to identify predictors of caregiver burden. Most
partners provided various kinds of support. ADL support and other practical support were given much more often by partners of persons with serious disability, but less A substantial proportion of difference was seen regarding emotional support. Professional partners of persons with SCI suffer from serious (paid) support was obtained by burden of support. Prevention of caregiver burnout should be part of
45.3% of all couples. Perceived burden of support was high in 24.8%
of partners of persons with serious disabilities against 3.9% of partners the lifelong care for persons with SCI.
of persons with minor disabilities. Significant predictors of caregiver burden were (in order of importance) the amount of ADL support given, psychological problems of the patient, partner age, partner gender, BI score and time after injury (total explained variance
47%).
Family caregivers' perceptions of the
types of services they require to assist them in their caring roles. Family care giving typically involved Mapping caregiver needs in this area establishes a critical basis for service physical, practical, and emotional planning and more importantly provides a guide for the development support, and in many cases this occupied in excess of three hours a day, with no additional source of care of a range of services dedicated to maintaining the health and well-being giving provided. The most frequently reported service types required by family caregivers included respite, of family caregivers of personal support, information services, and health professional individuals with SCI.
services.
Nursing & Healthcare International Journal
| Boschen et al. 2005 USA | Convenience sample; self- selected subsample in focus groups. | Productivity status, satisfaction with community integration, quality of life. | Quantitative phase (interview- completed questionnaire; n=100), followed by qualitative phase (8 focus groups; n=46). | Supporting a person with SCI brings significant life change. Greater support provision was related to lower productivity and community integration of the SPs. They felt underserved and unprepared emotionally and cognitively for their new, unanticipated role. | More attention, understanding, and service directed to SPs are required to reduce trial- and-error learning and emotional and physical burden. Enhanced injury resource materials, peer networks, and knowledge- building opportunities may ameliorate SP difficulties |
|---|---|---|---|---|---|
| DeSanto- Madeya, 2006 USA | 20 spinal cord injured persons and their family members to examine the meaning of living with spinal cord injury 5 to 10 years after the initial injury. | Interviews | Phenomenologi cal study | Seven themes emerged from the data. The themes are looking for understanding to a life that is unknown, stumbling along an unlit path, viewing self through a stained glass window, challenging the bonds of love, being chained to the injury, moving forward in a new way of life, and reaching normalcy. The uncovered meanings enhance our understanding and appreciation that living with spinal cord injury is a continuous learning experience. | The study findings may be useful in the development of self-care strategies and ongoing interventions that focus on maintaining physical and psychological health for both spinal cord injured persons and their family members throughout the course of living with the disability. |
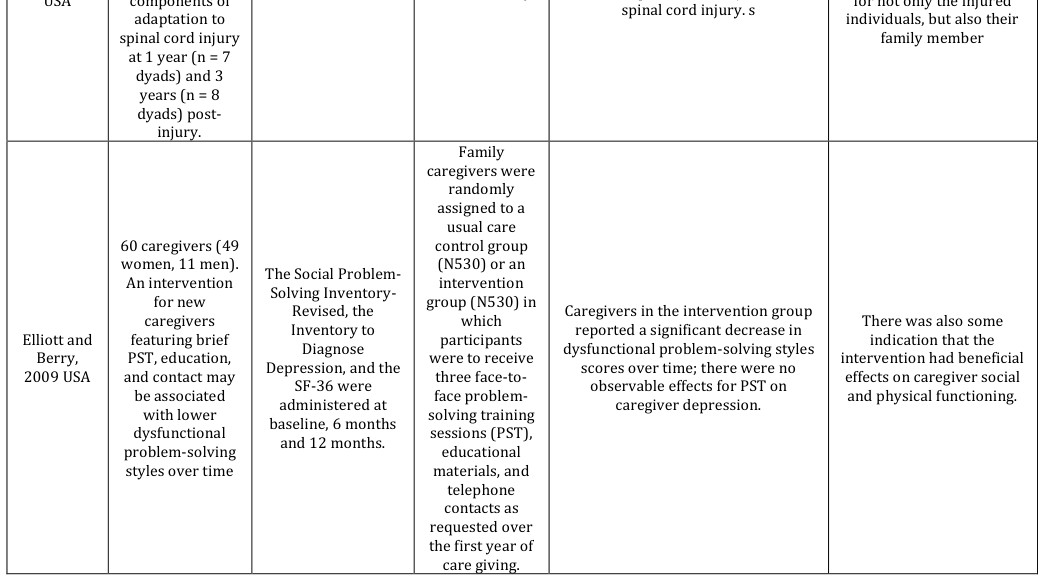
| Blanes et al., 2007 Brazil. | 60 primary caregivers of persons with paraplegia (T1 to S2) following traumatic spinal cord injury (SCI). Among 60 caregivers evaluated, 49 (81.7%) were female, with mean age of 35.8 (SD=12.91) years, 16 (26.6%) being wives and 14 (23.4%) sisters of persons with paraplegia | structured questionnaires and interviews The HRQoL was assessed by the Short Form-36 (SF- 36) health survey questionnaire and caregiver burden was evaluated by the Caregiver Burden Scale (CBS). | A cross- sectional descriptive study | It was found that the caregivers spend an average of 11.3 h/day caring for individuals with paraplegia. Twenty-three caregivers (38.3%) had a chronic disease and 32 (53.3%) were sole caregivers taking upon themselves the full responsibility of caring for the persons with paraplegia. The subjects reported lower scores on bodily pain and vitality than the other dimensions of the SF-36. The mean global CBS score was 1.71 (SD=0.50) and mean scores for each dimension ranged from 1.39 (SD=0.64) for emotional involvement to 2.44 (SD=0.79) for environment dimension. | The primary caregivers of spinal cord-injured persons reported low scores on all of the SF-36 and CBS dimensions, bodily pain and vitality being the SF-36 dimensions that received the lowest scores. |
| Dreer et al., 2007 USA | Eighteen men and 103 women caregivers (mean age of caregivers = 45.66 years, SD = 12.88) of individuals with SCI. | Inventory to diagnose depression | Correlational and logistic regression analyses of data collected in a cross-sectional design. | Nineteen caregivers (15.7%) met criteria on the Inventory to Diagnose Depression for a major depressive disorder. A dysfunctional problem- solving style was significantly predictive of caregiver depression, regardless of the severity of physical impairment of the care recipient or the physical health of the caregiver and caregiver demographic variables. | The percentage of caregivers with probable depressive disorder may parallel that observed among persons with SCI, using a more conservative self-report measure designed to assess symptoms associated with a depressive syndrome. Family caregivers with a dysfunctional problem- solving style and assisting individuals with more severe injuries may have probable depression |
Nursing & Healthcare International Journal
Qualitative study with a cross-sectional and descriptive- Data were collected through in-depth, tape-recorded, semi-structured explorative interviews and observation of a group discussion and two religious design. Grounded theory was used Chen & Boore, Fifteen family
2009 Taiwan
carers to explore the activities Eight
psychosocial implications for individual interviews and seven participating family carer who has a relative with in the group discussion.
spinal cord injury.
A multisite, three-group,
randomized controlled trial comparing two active intervention conditions with each other and to an information- only control group. One hundred seventy-three caregiver and care-recipient A multivariate outcome comprised dyads were of six indicators linked to the goals of the interventions randomly assigned to one of three conditions: a caregiver-only was the primary outcome of the One hundred seventy-three caregiver and care-recipient study. The multivariate outcome included treatment condition in Schulz et al., 2009 which caregivers received a multicomponen USA measures of dyads depressive symptoms, burden, social support and t intervention based on their integration, self- care problems, and risk profile; a physical health dual-target condition in symptoms.
which the caregiver intervention was complemented by a treatment targeting the care recipient, designed to address both caregiver and care recipient risk factors; and an information- only control condition in The findings resulted in the core category ‘living with a relative who Family carers experience a has a spinal cord injury’ and identified the experience of taking catastrophic life event, they have to confront challenges and the positive care of a relative who has a spinal cord injury. Three stages, including consequence is family resilience, the negative four categories: stage 1 ‘A catastrophic life event’; stage 2 ‘Confronting challenges’; and stage 3 consequence is family breakdown ‘Family resilience’ or ‘Family breakdown’.
At 12 months, caregivers in the dual- target condition had improved quality of life as measured by our multivariate outcome when compared to the control condition. Using the dyad as the unit of analysis, the dual-target condition was Caregivers are in need of superior to both the control condition and the caregiver-only and can benefit from interventions that help them manage the medical and functional limitations condition in our multivariate outcomes analysis. Dyads enrolled in the dual-target condition had significantly fewer health symptoms than control condition and caregiver- of the care recipient. Intervention strategies that target both the only condition participants and were caregiver and care recipient are particularly less depressed when compared to participants in the caregiver-only condition. In follow-up analyses we promising strategies for improving the quality of found that a higher proportion of life of caregivers.
caregivers in the dual-target condition had clinically significant improvements in depression, burden, and health symptoms when compared with the caregiver-only condition.
The data suggested that adaptation to spinal cord Findings indicate that spinal cord injured individuals and their family injury during the first 3 years can be enhanced by members, regardless of time since the initial injury, have a moderate level of adaptation and adjustment to for not only the injured individuals, but also their
Nursing & Healthcare International Journal
| Arango- Lasprilla et al., 2010 Colombia | 37 caregivers | Care giver needs questionnaire composed of 27 questions (1–5 scale) and 9 sub- scales (emotional, information, economic, community, and household support, respite, physical health, sleep, and psychological health). The Patient Health Questionnaire (PHQ-9) was used to measure caregiver depression, the Zarit Burden Interview (ZBI) measured stress, the Interpersonal Support Evaluation List Short Version (ISEL-12) measured social support, and the Satisfaction With Life Scale (SWLS) was used to assess satisfaction with life | Cross-sectional. | Information, economic, emotional, community support, and respite needs were most frequently reported among this group of Colombian caregivers. Forty-three percent of the family caregivers reported some level of depression, 68% reported being overwhelmed by their caretaking responsibilities, and 43% reported dissatisfaction with their lives. Information, emotional, economic, physical, sleep, and psychological needs were positively correlated with depression and burden. Those with more household, physical, sleep, economic, and psychological needs had less satisfaction with life and social support. Caregivers with more community and respite needs had less social support, while those with more emotional needs had less satisfaction with life. Caregivers with more respite needs had more burden and those with more household needs had more depression. | Approximately half of the sample reports some level of burden, depression, or being dissatisfied with life. Psychosocial functioning was related to various family needs. |
|---|---|---|---|---|---|
| Beauregar d & Noreau; 2010 Canada | Twenty-four spouses (eighteen women and six men) of persons with SCI | Individual interviews | The impact of SCI is focused primarily on three main areas: leisure, domestic tasks and family responsibilities, and sexuality. Spouses apply several strategies to overcome the difficulties they encounter, such as setting aside time for hobbies without the spouse, hiring staff to reduce the increased task load, reshuffling roles to coincide with the capabilities of the person with the spinal cord injury and maintaining open, honest communication with one's spouse on the topic of sexuality. | All these techniques, implemented and proven by experienced spouses, can be used as courses of action for clinical practitioners who work with spouses of people with disabilities in order to help them achieve a healthy balance in their life | |
| Dickson et al., 2010 UK | 11 participants who were both the spouse and primary caregiver of an individual with a SCI; of these, 10 were female and 1 was male. All interviews were transcribed verbatim and were subjected to Here we | Individual in-depth interviews | This study aimed to explore the lived experience of assuming the primary caregiver role in a group of spouses of individuals living with a traumatic spinal cord injury (SCI) (injuries ranged from paraplegia to quadriplegia). Interpretative | Three inter-related master themes: ‘The emotional impact of SCI’; ‘Post- injury shift in relationship dynamics’ and ‘Impact of care giving on identity’. Regarding the emotional impact of spinal injury, participants reported an almost instantaneous sense of loss, emptiness and grief during the injured person's rehabilitative period and feelings of anxiety were reported in anticipation of their return to the family home. | A distinct change in role from spouse and lover to care provider was reported and this ultimately contributed to relationship change and a loss of former identity. |
Nursing & Healthcare International Journal
phenomenologi cal analysis (IPA).
Qualitative interview study
focuses on the personal experiences of seven partners’ narratives 1 and Angel &Buus;
partners to a
2 years after their partner’s Interview
spinal cord injured person,
2011 Denmark
injury.
using a Ricoeurian phenomenologi cal-hermeneutic
approach.
30 primary caregivers of persons with SCI.
The majority of the participants
(n=20) were women, who had The Index of Psychological Well-
an ethnic Fijian
background (n=18) and were Being (IPWB) was used to assess the married (n=18), and were spouses psychological impact of care (n=13). Mean BI giving, and Caregiver Burden Inventory (CBI) was used to evaluate the of the persons with SCI was 7.1 Gajraj- (s.d.=5.23) on a 0–20 scale, with Singh, 2011 Fiji Cross-sectional burden associated with care giving for $$ 90 \% (n = 2 7) \mathrm {suffering from} \mathrm {moderate - to - very} $$ persons with SCI. Barthel Index (BI) severe disability scale was used to (BI<15). The mean duration of measure the functional abilities care giving was of the care recipients.
6.1 years (s.d.=4.23). On
average, the caregivers provided 6.1 h (s.d.=2.19) of care giving per day.
11 spousal caregivers to people with a traumatic spinal cord injury The
findings are discussed in relation to the wider literature Interpretative phenomenologi Dickson et Semi-structured al., 2012 interviews cal analysis UK (IPA).
and recommendation s for future caregiver support are highlighted.
The study revealed how the injury was experienced from the partners’ perspective through the aftermath. n The partner struggled to manage the overwhelming the acute phase after the injury, amount of everyday tasks. Some sought to reestablish partners also felt harmed, and support was needed in relation to their usual functions their own daily activities, eating, outside the family, whereas others focused on resting, and managing distress.
During the institutionalized rehabilitation, partners felt torn between supporting the injured partner and the demanding tasks of everyday life outside the institution.
establishing a new life together. The partners experienced much distress and appreciated the support they got, but felt that they were mainly left After discharge, partners struggled for the injured partner to regain a well-functioning everyday life and for to manage the difficult process on their own.
reestablishing life as a couple.
Being a primary caregiver of a SCI person contributes The experiences of care giving adversely affected the caregiver to caregiver burden and psychological distress. The psychological well-being. Participants demonstrated high findings indicate that the contributions of these levels of time-dependent and development burden. Care giving was people should be recognized and interventions should be tailored not only toward significantly related to the number of hours spent providing care (r_s=0.35, _P<0.05), and the older caregiver age the needs of the care recipients but also to the (r_s=0.46, _P<0.01).
needs of the caregivers.
Two inter-related master themes: (1)
Within these, the analysis
coping with the spousal caregiver role; and (2) putting the pieces back describes how regular venting of emotion, social together again. Adjustment was support and focusing on the positive aspects of the reportedly hindered by the introduction of paid caregivers as this represented a loss of privacy and situation all promoted coping.
power for the participants.
Nursing & Healthcare International Journal
59 individuals with SCI and their respective caregivers. Most
patients with SCIs were male, aged 35.4 years Cross-sectional
The scale Short Form 36 (SF-36) was used to assess observational study carried Nogueira et al., 2012 old on average, out by reviewing medical records with a predominance of HRQOL and the Caregiver Burden Scale (CBScale) for Brazil thoracic injuries and applying questionnaires.
followed by cervical injuries.
care burden.
Most caregivers were female aged
44.8 years old on average.
Secondary analyses of cross-sectional
data from a large cohort of adults aging with SCI and their primary Caregivers of caregivers. A community- dwelling adults hierarchical multiple regression aging with SCI (n=173) were interviewed as part of a multisite analysis examined the effects of social supports (social Rodakows Abridged Version of ki et al., 2013 USA randomized controlled trial. The mean age ± SD of caregivers was 53±15 years the Zarit Burden Interview integration, received social support, and negative social interactions) on and of care- recipients, 55±13 burden in caregivers of years.
adults aging with SCI while controlling for demographic characteristics and care giving characteristics.
Preventing care burden
through strategies that Tetraplegia and secondary complications stand out among the prepare patients for hospital discharge, integrating the support clinical characteristics that contributed to greater care burden network, and enabling and worse HRQOL. Association between care burden with HRQOL revealed that the greater the burden access to health care services are interventions that could minimize the effects arising from care burden and contribute to the worse the HRQOL.
improving HRQOL.
Findings demonstrate that
social support is an After controlling for demographic important factor associated with burden in characteristics and care giving characteristics, social integration caregivers of adults aging (β̂=−.16, P<.05), received social support (β̂ =−.15, P<.05), and negative with SCI. Social support should be considered for social interactions (β̂ =.21, P<.01) assessments and interventions designed to were significant independent predictors of caregiver burden.
identify and reduce caregiver burden.
Nursing & Healthcare International Journal
Cross-sectional secondary data analysesas part
of a multisite randomized controlled trial.
A hierarchical
multiple regression analysis examined the effect of social support (social Community- The Center for Epidemiological Studies Depression dwelling caregivers of aging adults with integration, received social Rodakows ki et al., 2012b USA Scale measured support, and negative social interactions) on spinal cord injuries (N = 173) caregiver depression symptom levels.
interviewed depressive symptom levels for the caregivers of adults aging with spinal cord injuries, controlling for demographic characteristics, and care giving characteristics Pearson's correlation was carried out to find any correlation between demographic variables with SF-36 dimensions. To find the effect of
72 wives of 72 veterans who were categorized the factors like age, employment status, duration as spinal cord injured patients Health related quality of life was Ebrahimza deh et al., 2013 Iran based on the American Spinal assessed by the Short Form (SF-36) of care giving, education, presence or absence of knee Injury Association Health Survey.
(ASIA) classification.
osteoarthritis, and mechanical back pain on different domains of the SF-36 health survey, Multivariate analysis of variance (MANOVA) was used.
Caregivers were, on average, 53
Findings demonstrate that negative social interactions years old (SD = 15) and care- recipients were 55 years old (SD = and social integration are associated with the burden
13). Average Center for Epidemiological Studies Depression Scale scores indicated that 69 (40%) in caregivers of adults aging with spinal cord injuries. Negative social of caregivers had significant depressive symptoms (mean 8.69, SD interactions and social = 5.5). Negative social interactions integration should be (β ˆ β^ = 0.27, P< 0.01) and social integration (β ˆ β^ = −0.25, P< 0.01) investigated in assessments and interventions intended to target caregiver depressive were significant independent predictors of depressive symptom levels in caregivers of adults aging symptom levels.
with spinal cord injuries.
The mean age of the participants was
44.7 years. According to the ASIA classification 88.9% and 11.1% of the veterans were paraplegic and tetraplegic respectively. Fifty percent The burden of care giving of them had a complete injury (ASIA can impact the QOL of A) and 85% of the spouses were exclusive care givers. All of the SF-36 caregivers and cause health problems. These scores of the spouses were significantly lower than the normal problems can cause limitations for caregiver spouses and it can lead to a population. Pearson's correlation demonstrated a negative significant decrease in the quality of correlation between both age and given care duration of caring with the PF domain. The number of children had a negative correlation with RE and VT.
Nursing & Healthcare International Journal
| Graca et al., 2013 Brazil | Fourteen women (seven caregivers and seven controls) | Medical Outcomes Study 36 - Item Short-Form Health Survey (SF-36) and the Caregiver Burden Scale (CBS) Questionnaires. | The data from both questionnaires were compared using the Mann- Whitney U testing procedure for differences between caregivers and controls (p<0.05). | The results from SF-36 were not statistically significant between groups, however, for the CBS data, there were significant differences between groups (p>0.05), characterized by the percentage difference of 62%, 66.7%, 55%, 50%, 57% and 63% for tension, isolation, disappointment, emotional involvement, environment and overall score, respectively. | The CBS questionnaire was more adequate for verifying quality of life of caregivers of SCI patients, and care giving may have a negative impact on their quality of life. |
|---|---|---|---|---|---|
| Lucke et al., 2013 USA | Family caregivers of Latino/Hispanic individuals with spinal cord injury (SCI) during the early years of recovery. 10 self- reported Latino family caregivers from whom informed consent was obtained from two Participants included 2 English/Spanish- speaking, and 7 Spanish speaking family caregivers who were interviewed within 2 years after their respective family member’s injury. Five caregivers were wives, 3 were mothers, and 1 was a father. Ages ranged from the 30s to the 60s, with a mean age of 48 years. Educational levels ranged from some grade school to some college. Only 1 of the caregivers was working full time outside the home; one family had a paid caregiver around the clock for their son. | Semistructured interviews with 9 family caregivers of Latino SCI survivors injured within the previous two years. Two interviews were conducted face to-face face, and seven interviews were conducted by telephone at the request of family members because of distance of the families from the researchers. A total of eleven interviews were conducted: nine in-depth interviews and two follow-up interviews. Interview questions were developed from the literature and previous studies. | Grounded Theory | “Resolving to go forward” was the core category that emerged from two simultaneous processes of “learning to care for” and “getting through” during the initial years as the primary informal caregiver. Most caregivers felt alone and abandoned after the injured person returned home, and experienced barriers to services and resources primarily because of language issues and economic status. | We recommend that researchers develop and evaluate culturally appropriate, informal care giving models to improve outcomes for both Latino individuals with SCI and their family caregivers. |
| Middleton et al. (2014) Australia. | (NZ44; spouses, parents, others) nominated as a primary caregiver by the person with SCI. | General Health Questionnaire-28 (GHQ-28), Medical Outcomes Study 36- Item Short-Form Health Survey (SF- 36), and Caregiver Strain Index (CSI) assessed the extent of psychological distress, HR-QOL, and burden, respectively, among caregivers. Functional status and community participation/care needs of the persons with SCI were assessed by the FIM and Craig Handicap Assessment and Reporting Technique, respectively. | Prospective longitudinal cohort study with measurements at 4 time points (6wk prior to discharge from subacute inpatient rehabilitation and 6wk, 1y, and 2y post discharge to community). | Multilevel piecewise models showed that psychological distress (GHQ-28 score) decreased significantly after discharge (slope estimate Z_.03, P<.008). At the pre discharge time point, the caregivers’ mental component summary score on the SF-36 was significantly lower than Australian national norms. The scores improved from pre discharge to 6 weeks post discharge (slope estimateZ.39, P<.001), but they did not change significantly across the following 2 time points (slope estimateZ.02, PZ.250). At all 3 post discharge time points, the mental component summary scores were not significantly different to national norms. In contrast, the physical component summary score of the SF- 36 did not significantly change across the pre discharge and 6-week post discharge time points (slope estimateZ_.14, PZ.121) and the 3 post discharge time points (slope estimate <.01, PZ.947). Scores at all 4 time points were not significantly different to the national norms. Caregiver burden showed no significant change over the study period (pre discharge to 6wk post discharge slope estimateZ.02, PZ.426; 3 post discharge time point slope estimates<_.01, PZ.334). Reflecting this, 42%ofcaregivers met CSI criterion at the first time point, and 46% met the criterion at the fourth (2y) time point. Higher burden was significantly correlated with increased hours of care being provided by the caregiver and lower FIM scores and lower community participation (for the person with SCI)at each time point. Psychological distress correlated with caregiver burden at 6 weeks and 1 year post discharge but not at 2 years post discharge. | The trajectory of scores for psychological distress and HR-QOL was consistent with caregiver adaptation to the challenge of providing support to a person with SCI in the early post discharge period. Caregiver burden did not display similar reductions but did not worsen over the study period. |
Nursing & Healthcare International Journal
Data Extraction
A data extraction form was developed and uploaded electronically into a reference management file. Data extraction of the available data (e.g., statistical power, sampling strategies, and strength of the comparison groups and methods of evaluation, internal and external validity) was undertaken. The author assessed the level of statistical power on reported differences between treatment and comparison groups and the sample size available for the analyses. To assess the rigour of the age matched comparators designs, the author assessed the presence of, or appropriateness and comparability of the comparison groups as well as the recruitment strategies to determine whether relevant sources of bias could have potentially been introduced. To address the quality of evidence available, the author considered whether the studies presented sufficient descriptions of the components and their mechanisms according to quality appraisal techniques. The verification of emergent findings may be deemed credible with regards to the decision making implicit within this article.
Nursing & Healthcare International Journal
Synthesis
According to Popay et al. (2006) [27], a realist synthesis review tells a trustworthy story. Thematic analysis invoking a constant comparative approach [28] was applied to the data to synthesise the findings, relationships and general robustness [27] of the research articles.
Findings
Prevalence of Caregiver Psychological Distress in Carers of Individuals with SCI
17studies provided estimates of the prevalence of psychological distress among SCI caregivers. Estimates included measures of depression [2, 17, 29, 30, 31, 32, 33, 34], stress and mood [35], mental health measure as part of a generic quality of life tool [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42]. Four questionnaire based studies [31, 32, 33, 34] used the Centre for Epidemiological Studies Depression Scale (CES-D) (REF). The CES-D is a self-report instrument consisting of 20-items, each scored 1-4, and individuals scoring 16 or more are generally considered to be at risk for clinical depression. In a cross- sectional study, Dreer, et al. (2007) [30] found 15.7% (n=121) met the criteria on the Inventory to Diagnose Depression (IDD) for a major depressive disorder. Rodakowski, et al. (2013) [32] using a sample of 173 subjects further demonstrated that caregiver perceived health status significantly predicted caregiver depression. Schulz, et al. (2009) [33] using a randomised controlled trial design (n=44) demonstrated depression scores as high with mean scores above the risk threshold for clinical depression (8 on the 10-item CESD). Weitzenkamp, et al. (1997) [34] reported that carers were at risk of increased depression that other spouses who were not carers and indeed scored lower quality of life scores compared with their partners who had the SCI. Caregiver stress was measured in 8 studies [3, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41] using predominantly the Caregiver Burden Inventory (CBI). The CBI is a multi-dimensional instrument developed by Novak and Guest (1989) [43] that measures the impact of burden on the caregivers. CBI consists of five subscales: (i) Time-Dependence Burden (burden because of restriction on the caregiver’s time); (ii) Development burden (feeling of being left behind in their development in respect to their peers); (iii) Physical Burden (feelings of chronic fatigue and damage to physical health); (iv) Social Burden (feelings of role conflict, resulting in arguments and time limitation) and (v) Emotional Burden (negative feelings towards the care recipient). Each subscale consists of five items except for the Physical Burden Scale, which contains only four items. Each item is scored on a Likert Scale from 1 (strongly disagree) to 4 (strongly agree). Scores from each subscale (with a maximum score of 20) are added to give a total score ranging from 0 to 100. The higher the scores in each subscale, the ore severe the burden imposed on the caregivers. CBI has shown good internal reliability (0.73- 0.85) and inter-correlations of subscales, and high-factor loadings [43]. The Medical Outcomes Study 36 – Item Short-Form Health Survey [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 37, 38, 39, 40, 41, 42, 43, 44, 45] was administered to a total of 312 SCI caregivers. The majority of carers were female (85.3%) and married to the patient (61%). According to the SF-36 mental component summary, caregiver scores were below the standardised normal values, and the lowest scores were observed for bodily pain and vitality [37]. However, because this study did not use a control group, it is not possible to quantify differences in percentage terms, which makes inferences about the larger impact of the act of providing assistance in the lives of caregivers difficult. However, the SF-36 often cannot measure with depth the effects and consequences that caring can have on the life of family caregivers of people with SCI. Lucke, et al. (2004) [40] determined family carers reported lower physical role, general health and vitality scores and reporting higher physical functioning and emotional role scores. Further, Nogueira, et al. (2012) [41] found statistically significant correlations in all domains of the SF-36 including general strain, isolation, disappointment, emotional involvement, environment and overall burden. Unalan, et al. (2001) [2] determined caring for a SCI individual significantly interferes with QoL using the Turkish version interview mode of administration SF-36. Graca, et al. (2013) [3] determined no statistical difference on the SF-36 though the Caregiver Burden Scale (CBS) revealed statistically significant negative impact on quality of life with an overall score of 63%.
Perceived Adequacy of Professional Support
This section relates to the literature pertaining to carers perceptions of professional support to assist them in their care giving role. Central to this theme was the need for information pertaining to SCI, its trajectory and symptom management of secondary complications of the resulting disability. Some carers expressed frustration and a lack of understanding by healthcare professionals [51] and felt they were left to manage the process on their own. Chan (2000) [29] reported that rehabilitation professionals were perceived to limit their attentions to the SCI person. Lucke, et al. (2013) [54], with a Latino- Hispanic population found that even though families had home care services for a period of time following discharge, the perception of the caregivers was that assistants did not help or even left early, before the care was completed: “We had home health for an hour a day to bathe him and get him up, but they never stayed their time. I ended up doing everything anyway”.
Nursing & Healthcare International Journal
Specifically, carers expressed a need for support to better manage the complex and challenging sequelae a SCI had wrought upon them [51]. DeSanto-Madeya (2009) [46] reported that depressed carers want support from other family members, each other and friends alongside access to a support from nurses and other healthcare professional services. Indeed, Dreer, et al. (2007) [30] state that the percentage of caregivers with probable depressive disorder may parallel that observed among persons with SCI. Beauregard & Noreau (2010) [49] presented qualitative data to suggest that the greatest help came in the form of hiring staff to reduce the increased task load the carer perceives, and in the form of respite care [47]. In reality, access and utilisation of support mechanisms can be problematic, with many carers stating that they lack knowledge of and access to professional services [17, 54] Dickson, et al. (2010) [52] outline a number of key issues with regard to paid care potentially impeding to some extent the maintenance of a sense of personal control and self-efficacy: “I have real difficulty with home carers coming in and out of the house because I … your life’s not your own, nothing is private any more. Somebody comes in every morning and every night for the rest of our lives” (Erin). However, this is counterbalanced by Amy “I can’t do it [caring] full time so we have to use the facilities that we are offered and the funding that we are given to have somebody in to do it” There was also a tendency for carers to actively seek professional support during the initial acute rehabilitation episodes only [41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52]. Upon discharge, there appears to be a lack of support available other than a caregivers own resourcefulness, resilience and optimism. This is an understandable source of frustration for carers with some relaying stories of trying to survive with what is available to them and desperate to avoid placing their loved one in a residential home: “[We can’t put him in a nursing home; what we have here is meagre, it is clean. He would not do well there. This is what God wants. [We] can’t put him in a home; [We] have to deal with it” [54]. A trend of reluctance to bother health care professionals is evident and contributes to the unmet needs of caregivers in this situation [48], despite the evidence that time and interest in the family would have clear positive benefits [17, 33, 51]. There was an expectation by some carers that professional services should be readily available and should not require the carer to seek services [39, 54]. The positive benefits to utilisation of respite and support were most evident when carers described care that was provided by someone who understands the condition [54]. However, in these studies conducted in what can be construed as developing countries the absence of paid support and the presence of other family members in the care of SCI persons are apparent. Extended family structure is a common feature of such cultures. Caregivers acknowledged the support of family members who provided assistance with ADL, helped with respite care, accompanied SCI individuals on outdoor activities and provided financial support. Assistance of other family members is also reported in minority ethnic groups and other cultures [1, 29, 37, 56]. Although paid support is a common feature in Western countries [35] it appears to be almost non-existent in developing countries. In these instances, the gap in the continuation of care is most likely filled by others present around these individuals.
Discussion
The primary objective was to determine the prevalence of psychological distress and risk factors of distress for informal caregivers of people with SCI. It is important to develop a greater understanding of care giving and psychological distress to identify caregivers whom may require more intensive assessment and support mechanisms. This review was limited by the sparse amount of studies that have assessed the prevalence of psychological distress, in particular depression, in this population. Common methodological limitations of studies included in this review were a lack of non- caregiver age-matched comparison groups, focus on the experience of female carers, small sample sizes, and failure to follow caregivers longitudinally. In this review only six studies [29, 31, 32, 33, 34, 35, 36] used a psychometrically validated measure of depression with scores suggestive of depression ranging from 40% to 59%. The largest study that measured depression in SCI carers (N=173) [32] reported the strongest prediction of depression levels, coinciding with the work of Blanes, et al. (2007) [37]. In comparison, estimates show that between 40% and 70% of the caregiver population have clinically significant symptoms of depression, with approximately one quarter to one half of these caregivers meeting the diagnostic criteria for major depression [4]. Other studies indicate that the mean CES-D scores for the studies by Weitzenkamp, et al. (1997) [34] and Arango- Lasprilla, et al. (2010) [36] are higher than a meta- analysis of CES-D score across a range of chronic conditions [10]. In particular, isolation and lack of support Nursing & Healthcare International Journal
are likely to be a high burden and result in distress or mental health problems, which have been identified as being 20% higher in carers than non-carers [57]. The conflicting reports of psychological distress identified in this review of SCI caregivers are likely to be related to the small number of studies and small sample sizes include in the review that may have been subjected to sampling bias. In summary, no reliable estimates of the prevalence of depression for SCI caregivers can be made at this present time. Psychological distress in caregivers results from a complex interplay of factors that included characteristics of the SCI individual and caregiver [3, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47]. Limited research has focused on potential caregiver risk factors, such as age, gender, SCI severity and characteristics, for caregiver psychological distress. Only two studies [2, 3] compared the presence of psychological distress of female SCI caregivers with an age-matched control group. Although these studies have the advantage of an age- matched comparator group, they are limited by small non-random samples, cross-sectional designs and the inclusion of wives only. No studies focused exclusively on males. No meta-analyses were located in reviewing the literature. It is apparent that caregivers’ subjective perception of SCI severity and the ability to alleviate distressing sequelae following SCI, reflects carers self-reported levels of psychological distress [3, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47]. In support of this, qualitative research uncovered aspects of care issues specific to SCI that are particularly distressing for caregivers. Nurses are ideally placed to provide education and management strategies to assist caregivers to cope with living a meaningful life with SCI. Involving the caregiver in SCI rehabilitation sessions and other patient focused interactions for the promotion of self- management, are likely to be of benefit to both patient and caregiver [33]. However, this needs to be viewed within the context that many caregivers are reluctant to initiate engagement with healthcare professionals for non-emergency situations [29, 47, 49]. There has been increasing recognition in recent years of the importance of providing support for carers in their caring role. In the UK, this has been evident, for example, in the 2006 Health and Social Care Whiter Paper [7], and the inclusion of carers; support in social services’ performance ratings [58]. Despite these important advances, this review indicates that SCI carers are generally not aware of or receive formal services to assist with the care giving role [54].
Caregiver perceived burden was most frequently measured using the ZBI. This is a well validated and widely used tool to assess burden in the general caregiver literature. Perceived burden was associated with caregiver depression and other measures of psychological distress. Interestingly, objective measures of caregiver burden, such as time spent attending to the patient, were not significantly related to poorer psychological outcomes [36, 42]. However, it cannot be assumed that objective measures of care giving, such as time spent attending to a patient with SCI, provide reliable indicators of caregiver perceived burden and psychological distress. This highlights the importance of healthcare professionals to address carers’ needs, including the emotional impact of care giving. Research exploring the impact of SCI in relationship dynamics between the patients and carer has consistently found that communication often suffered placing an increasing amount of strain on the relationship [3, 48, 55]. This finding is significant because poorer relationship quality was significantly associated with increased carer psychological distress [1, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54]. Despite the adversity of providing care for loved ones, self determination and commitment to the person with SCI was apparent. In particular, wives of men with SCI disclosed a determination to continue providing care to their partners for as long as possible [34, 35, 36, 37, 38, 39, 40]. This determination is likely to be at great emotional cost to the caregiver and highlights the importance of the provision of carer support services.
Review Limitations and Future Research
Achieving the aim of the review was limited by the complexity of the phenomenon under investigation, the volume of ‘evidence’ available and the disparate settings and cultures from whence it emerged. Future research would benefit from real-world collaborative research reviewing the effects of caring for family members with spinal injuries in the non-sterile, complex and dynamic environments in which they live. First, psychological wellbeing of carers should be studied in context and with cognisance of the longitudinal effects. Secondly, the one- dimensional nature of many of the studies reported here needs to be addressed. There is a need for triangulation in improving the utility of research into such interactions and effects, and the dearth of mixed method approaches should be remedied. It may therefore be useful for researchers in an area dominated by psychology to undertake interdisciplinary work involving people who can use their respective skills, knowledge and research Nursing & Healthcare International Journal
methodologies to inform a topic that so clearly permeates and transcends boundaries and disciplines. Further longitudinal research is needed to determine whether caregivers with more needs report worse psychosocial functioning or if those with worse psychosocial functioning report more needs.
Conclusion
This paper has provided a review and analysis of studies that have explicitly investigated the subjective well-being of informal caregivers of patients with SCI and the attendant physical ramifications of doing so. The totality of the current evidence-base suggests that many factors are related to caregiver distress but it is not possible to gauge the prevalence of this at present. To date, research into the psychological impact of SCI care giving has largely been confined to small, local investigations with a potential for selection bias. Despite these methodological shortcomings, the messages arising from these international studies are clear - SCI care giving is associated with psychological distress, and is influenced by lack of practical interventions and support mechanisms. Sub-optimal carer support is likely to lead to greater reliance on the health system. Whilst it is acknowledged that providing informal care provide a valuable service to society and can be rewarding to the caregiver, there is growing international concern about increased psychological distress and overall health deterioration experienced by family carers [57]. International policies focusing on future provision of long term care recommend a number of strategies to counteract the negative consequences of providing informal care – including payments for unpaid care, promoting flexible working conditions to enable carers to remain in the workforce, improved support service, such as respite [57]. Whilst such initiatives require significant upfront financial and social support family carers represent the key to long term care; the implementation of strategies to reduce the burden of providing care are essential. Further studies are needed to clarify the prevalence of SCI caregivers’ psychological comorbidities and specific factors that predict poorer carer health outcomes, so that appropriate interventions can be initiated, developed, and evaluated with a view to enhancing quality of life. Social and support networks, access to rehabilitation centres and health services with professionals cognisant of contemporary knowledge concerning individuals with SCI and caregivers are all extremely important towards a goal of minimising care burden. Corroborated by what occurred in mental health decades ago, a decrease in length of rehabilitation stay had forced the responsibility of Caring for people with SCI onto family members and caregivers. Although the goal of formal and informal caregivers is to prevent complications and enhance quality of life, without adequate resources these costs are transferred to physical and psychological sequelae for family caregivers. If properly supported in the transition to caring for a spinal cord injured individual with a focus on daily functioning and support, new ways of engaging in desired and necessary activities can be fostered.
References
-
Elliott TR, Shewchuk RM, Richards JS (1999) Caregiver social problem-solving abilities and family member adjustment in recent onset physical disability. Rehabilitation Psychology 44(1): 104-123.
-
Unalan H, Gencosmanoglu B, Akgun K, Karamehemetoglu S, Tuna H, et al. (2001) Quality of life of primary caregivers of spinal cord injury survivors living in the community: controlled study with short form-36 questionnaire. Spinal Cord 39(6): 318-322.
-
Graca A, Amarante do Nascimento M, Lavado EL, Garanhani MR (2013) Quality of life of primary caregivers of spinal cord injury survivors. Rev Bras Enfermagen 66(1): 79-83.
-
Zarit S (2006) Assessment of family caregivers: a research perspective. In: Family Caregiver Alliance (Edn) Caregiver Assessment: Voices and Views from the Field. Report from a National Consensus Development Conference (vol II) San Francisco, pp: 120.
-
Spence A, Hasson, F, Waldron M, Kernohan G, McLaughlin D, et al. (2008) Active carers: living with chronic obstructive pulmonary disease. International Journal of Palliative Nursing14 (8): 368-372.
-
Beesley L (2006) Informal Care in England. The King’s Fund, London, UK, pp: 43.
-
Department of Health (2006) Our Health, Our Care, Our Say. A New Direction for Community Services. NHS, London, UK, pp: 236. Nursing & Healthcare International Journal
-
Bergs D (2002) “The Hidden Client” – women caring for husbands with COPD: their experience of quality of life. Journal of Clinical Nursing 11(5): 613-621.
-
Seamark DA, Blake SD, Seamark CJ, Halpin DMG (2004) Living with severe chronic obstructive pulmonary disease (COPD): perceptions of patients and their carers. An interpretative phenomenological analysis. Palliative Medicine 18(7): 619-625.
-
Pinquart M, Sorensen S (2003) Differences between caregivers and non-caregivers in psychological health and physical health: a meta-analysis. Psychological Aging 18(2): 250-267.
-
Schulz R, Beach SR (1999) Care giving as a risk factor for mortality: the Caregiver Health Effects Study. JAMA 282(23): 2215-2219.
-
Lim JW, Zebrack B (2004) Caring for family members with chronic physical illness: a critical review of caregiver literature 2: 50
-
Toseland RW, Rossiter CM, Labrecque MS (1989) The effectiveness of peer-led groups to support family caregivers. The Gerontologist 29(4): 465-471.
-
Vrabec NJ (1997) Literature review of social support and caregiver burden 1980-1995. Image: Journal of Nursing Scholarship 29(4): 383-388.
-
Donelan K, Hill CA, Hoffman C, Scoles K, Feldman PH (2002) Challenged to care: Informal Caregivers in a changing health system. Health Affairs 21(4): 222- 231.
-
Vitaliano PP, Zhang J, Scanlan JM (2003) Is care giving hazardous to one’s health. A meta-analysis. Psychological Bulletin 129(6): 946-972.
-
Elliott TR, Berry JW (2009) Brief problem-solving training for family caregivers of persons with recent- onset spinal cord injuries: A randomized controlled trial. Journal of Clinical Psychology 65(4): 406-422.
-
Pawson R (2006) Evidence-based policy: A realist perspective, Sage, London, pp: 208.
-
Pawson R, Boaz A (2004) Evidence-based policy, theory-based synthesis, user-led review: An ESRC Research Methods Programme Project, London: ESRC UK Centre for Evidence Based Policy and Practice.
-
Pawson RT, Greenhalg, Harvey G, Walshe K (2004) Realist synthesis: an introduction. ESRC Research Methods Programme Working Paper Series.
-
Pope C, Mays N, Popay J (2008) Synthesising Qualitative and Quantitative Health Evidence: A Guide To Methods, Sociology of Health Illness 30(2): 330- 331.
-
Dixon Woods M, Fitzpatrick R (2001) Qualitative research in systematic reviews: opportunities and problems. BMJ 323(7316): 765-766.
-
Slavin RE (1995) Best evidence synthesis: an intelligent alternative to meta-analysis. Journal of clinical Epidemiology 48(1): 9-18.
-
Baumeister R, Leary MR (1997) Writing narrative literature reviews. Review of General Psychology 1(3): 311-320.
-
Derish PA, Annesley TM (2011) How to write a rave review. Clinical Chemistry 57(3): 388-391.
-
Saini M (2011) Qualitative research quality checklist, University of Toronto.
-
Popay J, Roberts H, Sowden A, Arai A, Rodgers H (2006) Guidance on the Conduct of Narrative synthesis in systematic Reviews. ESR: 1.
-
Glaser BG, Strauss AL (1967) The Discovery of Grounded Theory: Strategies for Qualitative Research, Hawthorne NY Aldine de Gruyter, Chicago.
-
Chan RC (2000) Stress and coping in spouses of persons with spinal cord injuries. Clinical Rehabilitation, 14(2): 137-144.
-
Dreer L, Elliott TR, Shewchuk R, Berry JW, Rivera P, et al. (2007) Family caregivers of persons with spinal cord injury: Predicting caregivers at risk for probable depression. Rehabilitation Psychology 52(3): 351- 357.
-
Elliott TR, Shewchuk RM, Richards JS (2001) Family caregiver social problem-solving abilities and adjustment during the initial year of the care giving role. Journal of Counselling Psychology 48(2): 223- 232.
-
Rodakowski J, Skidmore ER, Rogers JC, Schulz R (2013) Does social support impact depression in Nursing & Healthcare International Journal caregivers of adults ageing with spinal cord injuries. Clinical Rehabilitation 27(6): 565-575.
-
Schulz R, Czaja SJ, Lustig A, Zdaniuk B, Martire LM, et al. (2009) Improving the quality of life of caregivers of persons with spinal cord injury. Rehabilitation Psychology 54(1): 1-15.
-
Weitzenkamp DA, Gerhart KA, Charlifue SW, Whiteneck GG, Savic G (1997) Spouses of spinal cord injury survivors: The added impact of care giving. Archives of Physical Medicine and Rehabilitation 78(8): 822-827.
-
Post MW, Bloemen J, De Witte LP (2005) Burden of support for partners of persons with spinal cord injuries. Spinal Cord 43(5): 311-319.
-
Arango Lasprilla JC, Plaza SL, Drew A, Romero JL, Pizarro JA, et al. (2010) Family needs and psychosocial functioning of caregivers of individuals with spinal cord injury from Colombia, South America. Neurological Rehabilitation 27(1): 83-93.
-
Blanes L, Carmagnani MI, Ferreira LM (2007) Health- related quality of life of primary caregivers of persons with paraplegia. Spinal Cord 45(6): 399-403.
-
Ebrahimzadeh MH, Shojaei BS, Golhasani Keshtan F, Soltani Moghaddas SH, Fattahi AS, et al. (2013) Quality of life and the related factors in spouses of veterans with chronic spinal cord injury. Health and Quality of Life Outcomes 11: 48.
-
Gajraj Singh P (2011) Psychological impact and the burden of care giving for persons with spinal cord injury (SCI) living in the community in Fiji. Spinal Cord 49(8): 928-934.
-
Lucke KT, Coccia H, Goode JS, Lucke JF (2004) Quality of life in spinal cord injured individuals and their caregivers during the initial 6 months following rehabilitation. Qual Life Res 13(1): 97-110.
-
Nogueira PC, Rabeh SA, Caliri MH, Dantas RA, Haas VJ (2012) Burden of care and its impact on health- related quality of life of caregivers of individuals with spinal cord injury. Rev Latino Am Enfermagem 20(6): 1048-1056.
-
Rodakowski J, Skidmore ER, Rogers JC, Schulz R (2012) Role of social support in predicting caregiver burden. Archives of Physical Medicine and Rehabilitation 93(12): 2229-2236.
-
Novak M, Guest C (1989) Application of a multidimensional caregiver burden inventory. The Gerontologist 29(6): 798-803.
-
Ware JF, Kosinski M, Weller SD (1994) The SF-36 Physical and Mental Health Summary Scales: A User’s Guide. The Health Institute. New England Medical Centre, Boston.
-
Middleton JW, Simpson GK, De Wolf A, Quirk R, Descallar J, et al. (2014) Psychological distress, quality of life, and burden in caregivers during community reintegration after spinal cord injury. Archives of Physical Medicine and Rehabilitation 95(7): 1312-1319.
-
DeSantoMadeya S (2009) Adaptation to spinal cord injury for families post-injury. Nursing Science Quarterly 22(1): 57-66.
-
Foster M, Amsters D, Carlson G (2005) Spinal cord injury and family caregivers: A description of care and perception of service need. Australian Journal of Primary Health 11(1): 91-101.
-
Angel S, Buus N (2011) The experience of being a partner to a spinal cord injured person: A phenomenological-hermeneutic study. International Journal of Qualitative Studies in Health and Well- Being 6(4).
-
Beauregard L, Noreau L (2010) Spouses of persons with spinal cord injury: Impact and coping. British Journal of Social Work 40(6): 1945-1959.
-
Chen HY, Boore JRP (2008) Living with a relative who has a spinal cord injury: a grounded theory approach. Journal of Clinical Nursing 18(2): 174-182.
-
De Santo Madeya (2006) The meaning of living with spinal cord injury 5 to 10 years after the injury. Western Journal of Nursing Research 28(3): 265-289.
-
Dickson A, O'Brien G, Ward R, Allan D, O'Carroll R (2010) The impact of assuming the primary caregiver role following traumatic spinal cord injury: An interpretive phenomenological analysis of the spouses’s experience. Psychology and Health 25(9): 1101-1120. Nursing & Healthcare International Journal
-
Dickson A, O'Brien G, Ward R, Flowers P, Allan D (2011) Adjustment and coping in spousal caregivers following a traumatic spinal cord injury: an interpretative phenomenological analysis. Journal of Health Psychology 17(2): 247-257.
-
Lucke KT, Martinez H, Mendez TB, Arévalo-Flechas LC (2013) Resolving to Go Forward: The Experience of Latino/Hispanic Family Caregivers, Qualitative Health Research 23(2): 218-230.
-
Dickson A, O'Brien G, Ward R, Flowers P, Allan D (2012) Adjustment and coping in spousal caregivers following a traumatic spinal cord injury: an interpretative phenomenological analysis, J Health Psychol 7(2): 247-257.
-
Pinquart M, Sorensen S (2005) Ethnic differences in stressors, resources, and psychological outcomes of family care giving: A meta-analysis. The Gerontologist 45(1): 90-106.
-
Organisation for Economic Co-operation and Development (2011) Help wanted? Providing and Paying for Long-Term Care.
-
Commission for Social Care Inspection (2005) Performance Ratings for Social Services in England, CSCO, London, UK.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City