Proposed Plan of Home Based New Born Care in Kamis Mushayt, Saudi Arabia -Dr. Krishnavellie Chetty & Mary Johnson
The global burden of neonatal deaths is estimated to be 2.6 million, of which 0.76 million—more than a quarter—occur in India. With a neonatal mortality rate (NMR) of 26 per 1000 live births and infant mortality rate of 39 per 1000 live births,2 deaths in the neonatal period alone contribute to two-thirds of infant deaths in India. Even among postneonatal infant deaths (1–12 months), a major proportion of deaths occur in the second month of life. Any further reduction in infant mortality is therefore intricately linked to a major reduction of neonatal and young infant (0–59 days) deaths. Various attempts have been made to implement innovative approaches for newborn care at community/home level. The Cochrane review on communitybased interventions found a significant reduction—by about 25%—in neonatal mortality with community mobilisation and antenatal and postnatal home visits by health workers. The Lancet Every Newborn Study Group estimated that immediate scaling up of various community-based and primary care interventions can avert almost a third of all neonatal deaths by 2017 and one-fifth by 2025. Khamis Mushayt or Khamis Mushait city in south-west Saudi Arabia, located east of Abha, the provincial seat of the Asir province, It is the capital of the Shahran tribe. 8th largest in Saudi Arabia with an estimated population of 1,300,000. The infant mortality rate is a significant indicator of the quality of the health care provided to the population and gives insight into the factors that influence health. According to Millennium Development Goal 4, minimizing the infant mortality rate is a major challenge. Substantial efforts and resources are necessary to overcome these challenges, especially during the neonatal period, which is the main contributor to mortality figures for children under age five.The nursing team is striving to take initiative in promoting the new born care to the best possible so that the morbidity and mortality rates can come down even further and the new born wellbeing will be promoted in the areas of Khamis Mushait where the proposed plan of care is not available.
Introduction
Effective interventions to reduce neonatal deaths span both maternal and neonatal care and encompass interventions for appropriate care during pregnancy, care for the mother and newborn during and immediately after delivery, and care for the newborn during the first weeks of life, Home Based New Born Care.Home based New Born care is imperative to promote new born well-being and prevent morbidities and mortalities in the new born [1, 2, 3, 4, 5].
Hence a plan of new born care would be proposed and submitted in order to promote newborn well-being in Kamismushyt area where the health care coverage may be missing in one or two areas and such area of lacunae will be focused to make this proposal successful [6, 7].
The Team consists of mainly following activities:
- Home visits: For two to three hours every day, for at least four or five days a week, the ASHA should visit the families living in her allotted area. Home visits should take place at least once in a month if not more. Home visits are mainly for health promotion and preventive care. Over time, families will come to her when there is a problem and she would not have to go so often to their houses. Meeting them anywhere in the community/ village is enough. However, where there is a child below two years of age or any malnourished child or a pregnant woman, she should visit the families at home for counselling them. Also, if there is a newborn in the house, a series of five visits or more becomes essential.
- Visits to health facility: This is usually accompanying a pregnant woman or some other neighbour who requests her services for escort. The visit could also be to attend a training program or review meeting. In some months, there would be only one visit, in others, there would be more.
- Maintain records: Which would make her more organized and make her work easier, and help to plan better for the health of the people.
Newborn and Child Health
- That every newborn is visited as per the schedule, more often if there are problems and receives essential home based care as well as appropriate referral for the sick newborn.
- That every family receives the information and support it needs to access immunization.
- That all families with children below the age of two years counselled and supported for prevention of illness such as malaria, recurrent diarrhoea and respiratory infection.
- That every child below five years with diarrhoea, fever, acute respiratory infection (ARI) and worms, brought to her attention is counselled on whether referral is immediately required or whether, given the problems of access to a doctor, first contact curative care with home remedies and drugs in her kit, the child can be managed.
Essential Skills
The essential skills that the health worker requires can be classified into six sets. These are simple skills requiring only a few hours to learn, but they can save thousands of lives. These six sets of skills are given below: • Newborn care when visiting the newborn at home a. Counseling and problem solving on breastfeeding.
b. Keeping the baby warm. c. Identification and basic management of LBW (Low Birth Weight) and pre-term baby. d. Examinations needed for identification/first contract care for sepsis and asphyxia.
Qualities that Make an Effective Home Based Nurse
For a Home based Nurse to be effective in improving people’s access to health services and their health status, an ASHA should: i. Have the knowledge and skills to explain the basic maternal and child health services, educate on preventive and promotive aspects of maternal and child health, and provide some measure of immediate relief and advice if there is any illness. ii. Have the knowledge and skills on other general health issues, especially related to common infections, and be able to provide information on access to services and preventive and promotive aspects of healthcare. iii. Be friendly and polite with people and known among community, and establish rapport with the family during household visits. iv. Be a special friend to the needy, the marginalized, and the less powerful. v. Possess the art of listening. vi. Have the skill of coordination with community based hospital , AWW and ANM. vii. Be competent in conducting meetings in the community. viii. Be motivated and feel happy and rewarded to help community/serve people. ix. Have a positive attitude and be keen to learn new skills.
What Records need to be Maintained?
Village Health Register in which you will record details of pregnant women, children, 0-5 years, eligible couples and others in need of services. • Maintaining drug kit stocks: You are provided with a drug kit so as to be able to treat minor ailments/ problems. The drug kit contains: Paracetomol tablets, Albendazole tablets, Iron Folic Acid (IFA) tablets, Chloroquine tablets, Oral Rehydration Salts (ORS), and eye ointment. In addition, the kit may contain condoms and oral contraceptive pills, pregnancy testing kits, and malaria testing kits. The contents of the kit may change depending on the needs of the state. The drug kit is to be re-filled on a regular basis from the nearest PHC [8]. To keep a record of consumption of the drugs, and for effective re-filling and ensuring adequate/timely availability, a drug kit stock card is maintained. This can be completed by the person who refills the kit or by you.
Newborn Health
Care of the Baby at the Time of Delivery
• Many babies die immediately after birth due to asphyxia. In case of home delivery, when mild labor pains start; you can manage asphyxiated babies by removing mucus and can initiate respiration with the help of the instruments you have.
• You should encourage the mother to start breastfeeding immediately after the delivery, as this will help in quick delivery of placenta and minimizes bleeding. Starting to breastfeed immediately after the birth makes the baby stronger.
• Chances of the baby’s death and getting sick are higher among the babies born before time (pre-term) and in LBW babies. (Weight less than 2500 gm increases the risk and below 1800 gm, the risk is considered very high.)
Schedule of Home Visits for the Care of the Newborn
The purpose of these visits is to ensure that the newborn is being kept warm and breastfed exclusively. Encourage the mother to breastfeed; discourage harmful practices such as bottle feeds, early baths, giving other substances by mouth, and to identify early signs of sepsis or other illnesses in the newborn.
• The newborn requires a visit immediately after birth (or within the first 24 hours), and on Day 2, if the baby is born at home.
• If the baby is born at a facility, persuade and support the mother to stay for at least 48 hours, and therefore, the first two visits are taken care in the institution. However, if you are there with the mother, as a birth companion, then you could be of assistance to the nurse/ANM there.
• If the baby is born in a health facility, or at home, you should visit the baby on Days 3, 7, 14, 21 and 28. Additional visits are needed for newborn babies which are LBW, born before term and are sick.
Examining the Newborn at Birth
Steps for you to take “just after” the baby is born
➢ If the baby is born at home, or if you are present at the delivery
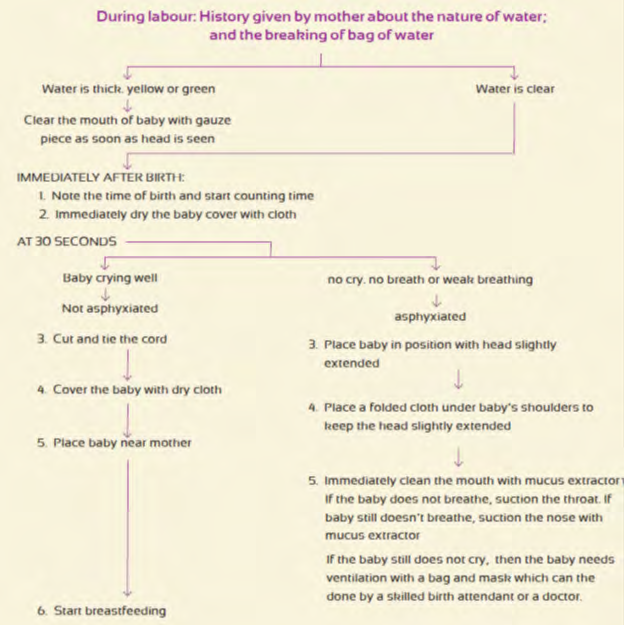
I. Ask the mother about/observe the fluid after the waters break.
II. If the fluid is yellow/green, as soon as the head is seen (even before delivery of complete baby), clean the mouth of the baby with gauze piece.
III. As soon as the baby is born, note the time of birth and start counting time.
IV. Observation of baby at birth or within the first 30 seconds and at 5 minutes after birth for movement of limbs, breathing and crying. The figure below will enable the assessment of whether the newborn should be recorded as a live or still birth. All six have to be “No” to declare a still birth. Even if one is “yes” the baby should be declared as live birth [9].
V. If there is no cry or a weak cry, if there is no breathing or weak breathing or gasping, this condition is called Asphyxia. If the baby is asphyxiated (does not breathe at birth), and there is no doctor or nurse, you should try to help and this skill is taught to you, in Module 7. However, in many such newborns, your efforts may not make enough difference and you should not feel bad or blame yourself for this. (Management of asphyxia will be taught in Module 7).
VI. Provide normal care at birth.
✓ Dry the baby: Immediately after delivery, the newborn should be cleaned with a soft moist cloth and then the body and the head wiped dry with a soft dry cloth. The soft white substance with which the newborn is covered is actually protective and should not be rubbed off.
✓ The baby should be kept close to mother’s chest and abdomen.
✓ The baby should be wrapped in several layers of clothing/woolen clothing depending upon the season.
✓ The room should be warm enough for an adult to feel just uncomfortable. The room should be free from strong wind.
VII. You should weigh the newborn and decide whether the baby is normal or LBW.
VIII. Determine whether the baby is term or pre-term.
IX. Measure newborn temperature.
First Examination of Newborn
➢ You should conduct the first examination within first 24 hours of delivery and look for the following:
• Whether the baby has any abnormality such as curved limbs, jaundice, and bump on head, cleft lip etc.
• How the baby’s suckling at the breast?
• Whether the baby has loose limbs.
• Listen to the cry of the baby.
• Provide care of eyes. If there are pus/purulent discharge from eyes and no doctor or nurse available, apply tetracycline ointment. Even for normal eyes, tetracycline is used as a preventive, so even in doubt as to whether it is pus, it could be given.
• Keep umbilical cord dry and clean.
➢ General precautions the family must take
The newborn is delicate and can easily fall sick if the family and mother are not careful. You should explain some general precautions that the family should take.
• Bathing the baby: Although it is recommended that the baby should not be bathed until the first seven days, many families would like to bathe the baby on the first or second day. For a normal baby, if the family insists, the baby could be bathed after the second day (48hrs). But in the case of LBW baby, you must insist on their waiting for at least seven days (one week). You should explain that bathing the baby and leaving it wet or exposed may cause it to get cold and fall sick. Thus, it is better to wipe the baby with a warm wet cloth and dry the baby immediately.
- Keep the baby away from people who are sick.
- People who are sick with cold, cough, fever, skin infection, diarrhea, etc. should not hold the baby or come in close contact with the baby.
- The newborn baby should not be taken to places where there are other sick children.
- The newborn baby should also not be taken to places where there are large gatherings of people.
What are you expected to do during the newborn visits?
- Enquire and fill the mother's information on home visit form.
- Enquire and fill newborn information on home visit form. These forms help you to think about all the steps you need to take.
- Take out the necessary equipment from the bag and keep on a clean cloth.
- Wash your hands well as taught.
- Then examine the baby –
- Measure temperature
- Weigh the baby
- Perform other activities in the sequence provided in the newborn home visit form.
- Provide the care of eyes, skin and cord.
- Check that the home visit form is filled in completely
Learning proper hand washing
- You must make sure that your hands are washed properly with soap before touching the baby. You should also teach the mother and family members to wash their hands before touching the baby.
Learning how to measuring temperature
- You should measure the temperature of the newborn using a special thermometer to see if the body temperature is normal or if baby has hypothermia (colder than normal).
Learn how to weigh the newborn
- Baby should be weighed within two days of birth.
- It is important to weigh the baby after birth because babies may require special care on the basis of the birth weight.
- It is better to use a special color-coded weighing machine meant just for weighing newborn which records the weight as green, yellow or red.
- If the baby's weight is “in the green zone: baby’s weight is normal and can be managed with normal care as described above.
- If in the yellow zone, the baby is mildly underweight, but can be managed at home with extra care as given below. (Below 2.5 kg but above 1.8 kg).
- If in the red colored zone, this means that the baby is very small and must be referred to the health centre. These babies also need extra care as given below. (less than 1.8 kg)
Learn how to take care of babies less than 2.5 kg
- Babies whose weight is in the yellow or red zone are small and require extra care as follows:
- Provide extra warmth.
- Family should ensure.
- Baby is wrapped well with thin sheets and blankets.
- The head is covered to prevent heat loss.
- The baby is kept very close to the mother’s abdomen and chest.
- Warm water filled bottles wrapped in cloth may be kept on either side of the baby’s blankets, when not being kept close to the mother’s body.
- The baby must be fed more frequently.
- All babies below 1.8 kg must be taken to a 24x7 facility or other facility known to provide referral care for sick newborn and examined by a doctor or nurse.
Umbilical cord care
- Cord should be kept clamped, till it dries and falls off.
- No application of any medicine is required if there is no bleeding or discharge.
- The umbilical cord should be kept clean and dry at all times.
Eye care
- Skill checklist for applying eye ointment
If a newborn has pus discharging from its eyes you can put antibiotic ointment in the baby’s eyes or a capsule which is available in the market.
How to put antibiotic ointment?
- Gently pull the baby’s lower eyelid down.
- Squeeze a thin line of ointment moving from the inside corner to the outside of the eye.
- Do not touch the baby’s eye with the tip of the tube. If the tube touches the baby’s eyes, it shouldn’t be used again.
- If the eyes are swollen with pus, then put the ointment two times a day for 5 days.
Breastfeeding
Benefits for the Baby
- Early skin-to-skin contact keeps the baby warm.
- It helps in early secretion of breast milk.
- Feeding first milk (colostrum) protects the baby from diseases.
- Helps mother and baby to develop a close and loving
- relationship.
- Benefits for the Mother
- •
- Helps womb to contract and the placenta is expelled easily.
- •
- Reduce the risk of excessive bleeding after delivery
- •
- Burns calories and lose pregnancy weight faster
- •
- Uterus returns to its pre pregnancy size
- •
- Lowers risk of breast and ovarian cancer
- Important Facts about Breastfeeding
- •
- Start breastfeeding immediately or at least within one
- Signs of breastfeeding going well
- Signs of possible difficulty
- Mother’s body relaxed, comfortable, confident, eye contact with baby, touching
- Mother tense, leans over baby. Not much eye contact or touching
- Baby’s mouth well attached, covering most of the areola, opened wide, lower lip turned outwards
- Mouth not opened wide, not covering areola Lips around nipple
- Suckling well, deep sucks, bursts with pauses
- Rapid sucks, cheeks tense or sucked in Smacking or clicking sounds
- Cheeks round, swallowing heard or seen
- Baby calm and alert at breast, stays attached, Mother may feel uterus cramping, some milk may be leaking (showing that milk is flowing)
- After feed, breast soft, nipples protruding
- After feed, breast full or enlarged, nipples may be red, cracked, flat or inverted
Table 1: Breastfeeding Observation Tips.
Correct Position for Breastfeeding
To obtain maximum benefit of breastfeeding, the baby should be held in the correct position and be put correctly to the breast. The baby is in the correct position when:
- While holding the baby, the mother also supports the baby’s bottom, and not just the head or shoulders.
- Mother holds the baby close to her body.
- The baby’s face is facing the breast, with nose opposite the nipple (Figure 1).

Figure1: Breastfeeding Positions.
Counseling Tips
- You are there to help the mother, not to take over.
- Use verbal and non-verbal skills to make her feel at ease.
- Encourage and praise her; every mother has the ability to breastfeed. Often mothers are worried that they are inexperienced and lack the confidence. Many women do not breastfeed successfully because they do not get good advice, support and encouragement.
- If she says something that you do not agree with, do not say ‘that is wrong’. Do not make her feel bad or stupid. You can repeat what she says.
- (For example, ‘I hear you saying that you think you don’t have enough milk...’ Ask her why she thinks so. Listen to what she is saying and why).
- After you assess the breastfeeding, you should check the baby’s weight gain.
- Give advice in simple and clear language.
- Make sure the mother understands what you are saying.
- Have her repeat what she will try to do.
Why only Breastfeeding?
Giving other food or fluid may harm the baby in following ways
- It reduces the amount of breast milk taken by the baby.
- It may contain germs from water or on feeding bottles or utensils. These germs can cause diarrhea.
- It may be too dilute, so the baby becomes malnourished.
- Baby does not get enough iron from cow’s and goat’s milk and may thus develop anemia.
- Baby may develop allergies.
- Baby may have difficulty digesting animal milk; the milk can cause diarrhea, rashes or other symptoms. Diarrhea may become persistent.
- Breast milk provides all the water a baby needs. Babies do not need extra water even during the summer months.
Managing Common Breastfeeding Problems
Sore Nipples
- Causes: poor latch-on or positioning at breast
- Management
- Improve attachment and/or position.
- Continue breastfeeding (reduce engorgement if present).
- Build mother’s confidence.
- Advise her to wash breast once a day; not to use soap for this.
- Put a little breast milk on nipples after feeding is finished (to lubricate the nipple) and air-dry.
- Wear loose clothing.
- If nipples are very red, shiny, flaky, itchy, and their condition does not get better with above treatment, it may be fungus infection. Apply gentian violet paint to nipples after each breastfeed for five days. If the condition does not improve, refer to a doctor.
Inverted Nipples
Sometimes the nipple will retract in to the breast, and can be checked even during pregnancy. The best treatment is to encourage the mother to gently pull out the nipple and roll it, several times in a day.
Not Enough Milk
- Causes: Delayed initiation of breastfeeding; infrequent feeding; giving fluids other than breast milk; mother’s anxiety, exhaustion, insecurity; inadequate family support.
- Management
- Decide whether there is enough milk or not:
- Does the baby pass urine six times or more each day?
- Has the baby gained sufficient weight? (During the 1st week there is usually a small weight loss, after that a newborn should gain 150-200 gm per week.)
- Is the baby satisfied after feeds?
- Re-assure mother.
- If there is not enough milk, have the baby feed more often.
- Check breastfeed to observe mother attachment and positioning of the mother and baby.
- Encourage rest. Emphasize the mother to drink and eat more.
- Praise her and return for follow-up.
Engorged and Painful Breasts (Very Full Breasts)
- Causes: Delayed initiation of breastfeeding, poor attachment, incomplete emptying of breasts, restricting the length of the feeds.
- Management
- Prevent by:
- Starting breastfeeding soon after delivery and feeding often.
- Ensuring correct attachment.
- Encouraging on-demand feeding.
- If baby is able to suckle, feed more frequently, help with positioning.
- If the baby is not able to attach [10], apply warm compresses to breast, gently massage from outside toward the nipple and express some milk until the areola is soft, then put baby to the breast, making sure that the attachment is correct.
- Have baby feed often to empty out the breasts. If it is not possible, ask the mother to express some milk herself.
- If breasts are red and hard, continue to feed often. Use
warm compresses and gently massage breasts towards nipple. Take mother’s temperature. If she has fever, mother should visit the doctor. She should continue to breastfeed (from both sides) even if she is taking antibiotics.
Expressing Milk by Hand
- Wash hands with soap and water.
- Place a warm compress on the breast for a few minutes if desired.
- Gently massage the breast starting from the chest moving toward the nipple; do this in a circle (near the underarm, and then to the bottom of the breast etc.), so that all parts of the breast are massaged.
- Lean forward and support the bottom of the breast with one hand.
- Hold the areola between thumb and two fingers of other hand. Put her hand on the areola above the nipple and the two fingers on the areola below the nipple [11].
- Press toward the chest (about 1-2 cm) and then squeeze the milk reservoirs beneath the areola (do not squeeze the nipple).
- Press and release the thumb and first finger several times until the milk drips out. Use a clean bottle or a cup to collect the milk. Milk may drip at the beginning and then spray out after it starts flowing.
- Rotate the thumbs and finger around the areola so that the milk is removed from all the reservoirs.
- Repeat with the other brea1st.
Signs That the Baby is Not Getting Enough Milk
- Poor weight gain
- Weight gain of less than 500 gm in a month
- Less than birth weight after two weeks
- Passing small amounts of concentrated urine
- Less than six times a day
- Yellow and strong smelling
- Other signs are:
- Baby not satisfied after breastfeed and often cries
- Very frequent breastfeeds
- Very long breastfeeds
- Baby refuses to breastfeed
- Baby has hard, dry or green stools
- No milk comes when mother tries to express
- Breast did not enlarge
- Milk did not come in.
Mothers and families think that in the following situations, their milk is not enough, but in fact, these do not affect the breast milk supply:
- Age of mother
- Sexual intercourse
- Return of menstruation
- Disapproval of relatives and neighbors
- Age of baby
- Caesarean Section
- Many children
- Simple, ordinary diet
Breastfeeding Low Birth Weight/Pre-Term babies
Advantages of breast milk for LBW and pre-term Babies:
- Has the right nutrients for the pre-term/LBW baby
- Pre-term babies need more protein and a mother who has delivered pre-term has more breast milk.
- Is easily digestible.
- Contains factors to fight infection (small babies are more vulnerable to disease).
- Breastfeeding keeps the baby close to the mother and therefore, warm.
- This protects the pre-term baby from cold (Hypothermia), which can lead to infection.
Key Messages
For small babies who can suckle
- Try the underarm hold for more support or the alternate underarm hold.
- If sleeping, wake baby every 2-3 hours for breastfeeding by rubbing a damp cloth over its face.
For Babies Who are not Able to Suckle
- Babies less than 1500 gm may not be able to breastfeed in the beginning.
- Express milk by applying gentle pressure over entire breast and collect milk in a clean bowl.
- Express milk every 2-3 hours to keep the milk supply up.
- Put baby to breast and allow her to lick the nipple, and try to suckle.
- Once the baby is able to suckle, she should be put to the breast as often as possible to stimulate milk production.
- Continue feeding with the spoon as well until the baby is getting its milk requirements directly from the breast.
How Much to Give?
- For a LBW baby: For first day 60 ml/kg body weight.
- Add 20 ml/kg body weight until baby is taking 200 ml per day.
- Divide the total into 8-12 feeds (every 2-3 hours).
- Colostrum can be kept for up to 12 hours at room temperature.
- Mature milk (after first 72 hours) can be kept for 6-8
hours at room temperature. • Continue until baby can be fully breastfed.
Keeping the Newborn Warm
Why is it Important to Keep Baby Warm after Delivery?
Babies have difficulty maintaining their temperature at birth and in the first day of life. They come out wet, and lose heat quickly. If they get cold, they use up energy, and can become sick. LBW and pre-term babies are at greater risk of getting cold.
When and Why do Most Newborns Get Cold?
Most newborns lose heat in first minute after delivery. They are born wet. If they are left wet and naked, they lose a lot of heat to the air. A newborn baby’s skin is very thin and baby’s head is big in size compared to the baby’s body [12]. It loses heat very quickly from its head. Babies do not have the capacity to keep themselves warm. If the newborn baby is not properly dried, wrapped, and its head is not kept covered, it can lose 2 to 4 degree Celsius within 10-20 minutes.
Example: If the baby’s temperature was 97.7 degree Fahrenheit (36.5 degree Celsius) (normal temperature) at the time of birth and if there was a loss of 2.7 degree Fahrenheit because the baby was not properly dried and covered, the body temperature will become 95 degree Fahrenheit (35.0 degree Celsius), which is below normal.
What is the Term for a Situation When a Baby’s Temperature Falls below Normal?
When a baby has temperature below normal, it suffers from hypothermia.
What Happens to a Baby with Hypothermia?
A baby who is cold, and has a low temperature (hypothermia) suffers from:
- Decreased ability to suckle at the breast, leading to poor feeding and weakness. Increased susceptibility to infections.
- Increased risk of death, especially in LBW and pre-term babies.
How can you tell if a Baby is Hypothermic?
- The early sign is cold feet.
- Then, the body becomes cold.
- The best method is to measure the baby’s body temperature.
How to Keep Newborns Warm?
- Before delivery, warm up the room (warm enough for adults).
- Immediately after delivery, dry the baby.
- Put a cap on the baby since a lot of heat could be lost though its head.
- Place in skin-to-skin contact (Kangaroo Mother Care) with mother.
- Cover or put clothes on the baby, wrap it up with clean cloth, and place it close to its mother.
- Initiate early breastfeeding.
- Bathing for newborns:
- It is best to wait until the second day to bathe the baby. One should wait seven days in case of LBW baby.
- If the family insists on bathing the first day, please ask them to delay for at least six hours to give the baby time to adjust with its new environment.
- For small and pre-term babies, do not give a bath until the baby gains weight (this could be few weeks) and weight of baby become 2,000 gm.
- To keep a small baby clean, you can give a light oil massage but making sure that the room is warm and the baby is not left uncovered for more than 10 minutes. DO NOT pour oil into any orifice, like the nose or ears at any time.
- Keep baby loosely clothed and wrapped.
- If it is very warm outside, make sure the baby is not too heavily clothed and wrapped; the baby can also get too hot.
- Wherever possible, insist on referral to a facility that is managing sick newborns. If this is not immediately possible, begin the following steps:
How to Re-warm a Baby getting Cold?
<97 degree Fahrenheit (36.1 degree Celsius) or too cold <95 degree Fahrenheit (35.0 degree Celsius)
- Increase the room temperature.
- Remove any wet or cold blankets and clothes.
- Hold the baby with its skin next to its mother’s skin (skin-to-skin contact) and place a warmed cloth (not too hot to avoid burns) on its back or chest. As this cloth cools down, replace it with another warmed one, and repeat until the baby is warmer. Continue until the baby’s temperature reaches the normal range.
- Put on its clothes and its cap, put it in warm bag, and make it lie close to its mother.
- Continue to breastfeed the baby to provide calories and fluids to prevent a drop in the blood glucose level.
- A common problem in hypothermic babies.
If a baby is too cold <95 degree Fahrenheit (35.0 degree Celsius), follow the above and advice.
- Place skin-to-skin, and once the baby is a little warmer, then clothe baby and place in a bed pre-warmed with warm clothes, or a hot stone or hot water bottle. (Remove these articles before putting baby on the bed.)
- In an institutional delivery, there should be a newborn corner available with a radiant warmer or some other suitable heating arrangement where the newborn baby can be kept.
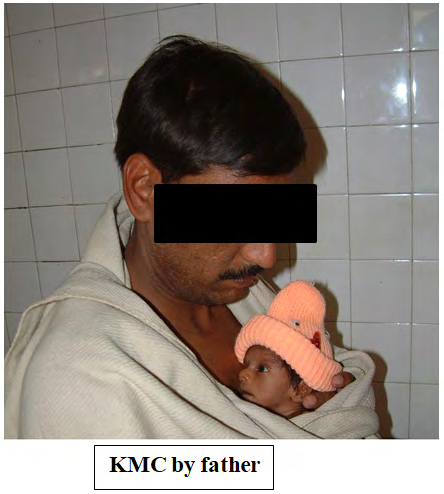
Kangaroo mother care or skin to skin contact:
- A special way of caring for Low birth weight (LBW) babies
- It promotes
- Effective thermal control
- Breast feeding
- Prevention of infection
- Parental bonding Components of KMC i. Skin-to-skin contact: Early, continuous and prolonged skin-to-skin contact ii. Exclusive breast feeding: Promotes lactation and facilitates feeding Benefits of KMC
- Breast feeding
- Increased breast feeding rates
- Increased duration of breast feeding
- Thermal control
- Effective thermal control
- Equivalent to conventional incubator care
- Lesser morbidity
- Regular breathing
- Decreased episodes of apnea
- Protection from nosocomial infections
- Early discharge
- Better weight gain enhances early discharge
- Other benefits
- Less stress to the infant
- Stronger bonding
- Deep satisfaction for mother
- More confident parents Eligibility criteria: Baby
- Birth weight >1800 gm: Start at birth
- Birth weight 1200-1799 gm: Hemodynamically stable
- Birth weight <1200 gm: Hemodynamically stable Eligibility criteria: Mother
- Willingness
- General health & nutrition
- Hygiene
- Supportive family
- Supportive community Preparing for KMC
- Mother’s clothing Front-open, light dress as per the local culture.
- Baby’s clothing Cap, socks, nappy and front-open sleeveless shirt or ‘jhabala’.
KMC Procedure
Kangaroo Positioning
- Place baby between the mother’s breasts in an upright position
- Head turned to one side and slightly extended
- Hips flexed and abducted in a “frog” position; arms flexed
- Baby’s abdomen at mother’s epigastrium
- Support baby’s bottom
Check If
- Neck position is neutral
- Airway is clear
- Breathing is regular
- Color is pink
- Temperature is being maintained (Figures 2 & 3). Any family member can do it!
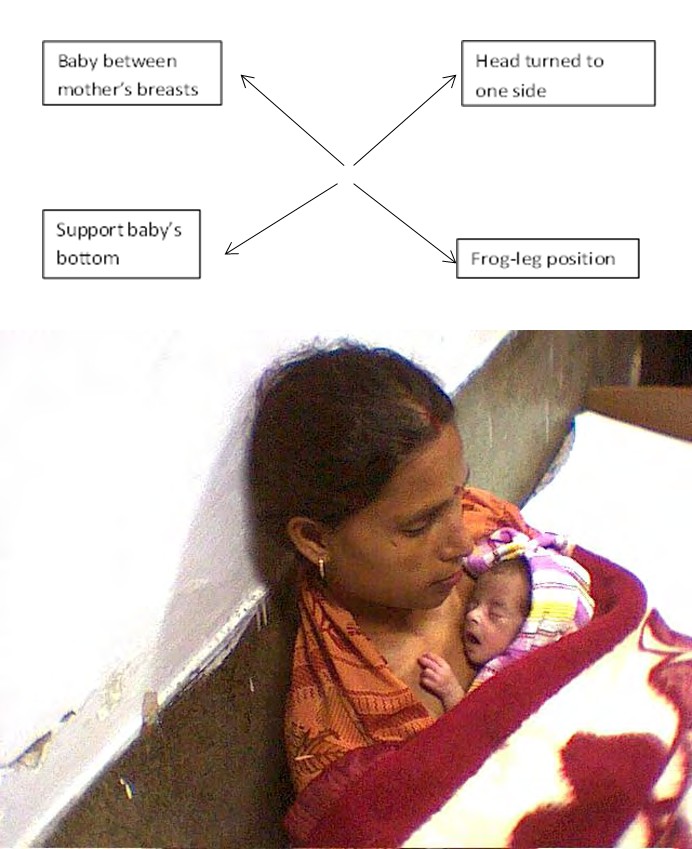
Figure2: Positions.
Management of Fever in Newborn
A baby has fever if the temperature is above 99 degree Fahrenheit (37.2 degree Celsius). In the case of high body temperature of the baby during summer, verify in the following manner whether this is due to the body being overdressed or does it really have fever:
- Unwrap the baby and take off its cap.
- Ventilate the room too to cool the baby.
- Ask the mother to start breastfeeding.
- If there is a source of extra heat (like a fire) in the room, put it out.
- Wait for 30 minutes and take the temperature once again. If the baby’s temperature returns to normal, explain to the mother that in very warm weather, the baby does not have to kept covered with additional cloth or kept wrapped [13].
If the temperature is still above normal after the above measures have been taken, refer the baby for treatment.
Immunization
Universal Immunization Program
- Immunization Program is one of the key interventions for protection of children from life threatening conditions, which are preventable. It is one of the largest immunization programs in the world and a major public health intervention in the country.
- Immunization Program in India was introduced in 1978 as Expanded Program of Immunization (EPI)
- The program gained momentum in 1985 and was expanded as Universal Immunization Program (UIP) to be implemented in phased manner to cover all districts in the country by 1989-90.
- UIP become a part of Child Survival and Safe Motherhood Program in 1992 Since, 1997, immunization activities have been an important component of National Reproductive and Child Health Programme and is currently one of the key areas under National Rural Health Mission (NRHM) since 2005
- Under the Universal Immunization Program, Government of India is providing vaccination to prevent seven vaccine preventable diseases i.e.
- Diphtheria, Pertussis, Tetanus, Polio, Measles, severe form of Childhood Tuberculosis and Hepatitis B, Haemophilus influenza type b (HIB) and Diarrhoea (Table 2).
| When to give | Dose | Route | Site | |
|---|---|---|---|---|
| For Infants | ||||
| BCG | At birth or as early as possible till one year of age | 0.1ml (0.05ml until 1 month of age) | Intra -dermal | Left Upper Arm |
| Hepatitis B Birth dose | At birth or as early as possible within 24 hours | 0.5 ml | Intramuscular | Anterolateral side of mid-thigh-LEFT |
| OPV Birth dose | At birth or as early as possible within the first 15 days | 2 drops | Oral | - |
| OPV 1,2 & 3 | At 6 weeks, 10 weeks & 14 weeks | 2 drops | Oral | - |
| IPV (inactivated Polio Vaccine) | 14 weeks | 0.5 ml | Intramuscular | Anterolateral side of mid-thigh-RIGHT |
| Pentavelant 1,2 & 3 | At 6 weeks, 10 weeks & 14 weeks | 0.5 ml | Intramuscular | Anterolateral side of mid-thigh-LEFT |
| Rota Virus Vaccine | At 6 weeks, 10 weeks & 14 weeks | 5 drops | Oral | - |
| Measles 1st Dose | 9 completed months-12 months. (give up to 5 years if not received at 9-12 months age) | 0.5 ml | Subcutaneous | Right Upper Arm |
| Vitamin A, 1st Dose | At 9 months with measles | 1 ml (1 lakh IU) | Oral | - |
Table 2: National Immunization Schedule.
High Risk Assessment and Management of Low Birth Weight/Pre-Term Babies
Guidelines for ASHA on Identifying A High Risk Baby
- Birth weight less than 2000 gm.
- Pre-term (delivery which happens when mother is 8 months and 14 days pregnant or less).
- Baby not taking feeds on Day 1.
If you were not present at the time of delivery and your first visit to the newborn is delayed, then the newborn is to be weighed on the day of your first visit. In such cases, using the following Table 3, determine whether the baby is high risk or not:
| Weighed for the first | Time | |
|---|---|---|
| 1 to 14 days | Less than 2 kg | High Risk Baby |
| 15 to 21 days | Less than 2 kg 100 gm | High Risk Baby |
| 22 to 27 days | Less than 2 kg 200 gm | High Risk Baby |
| 28th day | Less than 2 kg 300 gm | High Risk Baby |
Table 3: Whether the baby is high risk or not.
Guidance that you Should Give to the Family
- Keep the baby clothed from the very first day. In winter, cover the baby with a blanket.
- Do not bathe a baby until its weight is 2000 gm.
- Ensure that mother’s nails are cut and that her hands are washed every time the baby is breastfed.
- After returning from the toilet, all family members must wash their hands with soap before touching the baby.
- High risk babies should be breastfed after every two hours.
- If baby is not suckling milk, squeeze the breast milk in a small bowl and then feed the baby with a spoon.
- The weight of high risk babies should improve every week from second week. If this does not happen, counsel them to consult you.
- Ask them to call you immediately if the baby develops any of the following:
- All limbs become limp, stops feeding, has chest in drawing, has fever, and is cold to touch.
What should you do if The Baby is at High Risk?
• Increase the number of home visits after delivery from
5 to 13.
- A daily visit, if possible, for the first week
- Once every three days until the baby is 28 days old, and if the baby is improving once on the 42nd day.
- Weigh the babies on Day 7, 14, 21, 28. Babies who weigh less than 2300 gm on the 28th day have a higher risk of dying. If the baby is not gaining weight, refer the baby to the hospital.
- Explain the high risk issues to the parents and family (see box above).
- Provide specific care as per the problem but in general, keep the baby warm and breastfeed more often every two hours.
- For poor breastfeeding, observe the mother breastfeeding. Ensure proper latch on and positioning. Encourage the mother so that she is motivated to feed the baby well. Counsel the mother that she should not give other liquids or feeds.
- If on Day 28 the weight is less than 2300 gm or weight gain in 28 days is less than 300 gm, then you should continue to visit once a week in the 2nd month and take the weight every week.
- Fill home visit form for high risk baby
Asphyxia Diagnosis and Management
What is Asphyxia?
A baby having any one of the following symptoms at the time of birth is asphyxiated:
- No cry
- Weak cry
- No breathing
- Weak breathing. If a baby has asphyxia, it is an Emergency. A life can be saved or lost in these five minutes. If you are present at the time of birth, and there is no doctor or nurse, you should try to help to manage the baby. However, in many such newborns, your efforts may not make enough difference and you should not feel bad or blame yourself for this. Depending on the area in which you work, you may be trained in using a bag and mask to treat asphyxia.
Consequences of Asphyxia
- Immediate (at birth)
- Baby is born dead (stillbirth)
- Dies at once or within a few days
- Unable to suckle.
- Long term If the baby survives, it may have:
- Mental retardation
- Epilepsy (seizures and fits)
- Spasticity (difficulty walking or moving arms and hands).
- These signs warn of asphyxia during labour
- Prolonged or difficult labour
- Ruptured membranes with little fluid (dry delivery)
- Green or yellow colour thick amniotic fluid
- Cord comes out first or cord is wound tightly around the neck
- Pre-term labour (delivery taking place less than 8 months 14 days of pregnancy)
- Baby being born in a position in which the head does not come out first.
• Asphyxia Action Tree You must know the signs during labour that may indicate asphyxia at birth. In this module, ASHA will learn to manage asphyxia using a mucus extractor (Figure 4).
Neonatal Sepsis: Diagnosis and Management
“Sepsis” means infection. In newborn babies, “sepsis” refers to any serious infection in the baby whether in the lungs, brain or blood.
How Common Is Sepsis and How Serious?
- In rural India, one out of every ten newborns develops sepsis.
- Sepsis in the first month of life is very serious, and is the most common killer of newborns in the first month of life.
- Without treatment, many babies with sepsis will die; with treatment, most babies will get better, live and grow up normally.
Causes of Neonatal Sepsis
- Mother has infection during pregnancy or delivery.
- Unclean techniques during delivery (poor hand washing, use of unclean blade or cord ties) can cause sepsis.
- Cord becomes infected from unclean cutting or putting dirty things on it
- Baby is weak; born pre-term or with LBW (less than 2000 gm)
- Baby becomes weak from poor feeding practices; not giving breast milk early and exclusively.
- Baby becomes weak – exposed to the cold after delivery.
- Baby comes into contact with someone who has an infection: mother, family members, or ASHA Can Sepsis Be Prevented? Yes, if the Following are Observed Carefully
- Good hygiene: frequent hand washing; clean instruments during delivery; clean clothes
- Keeping the baby warm during the cold season
- Breastfeeding (early initiation and on demand, and exclusive)
- Keeping the umbilical cord clean and dry
- Information about danger signs to parents: You should teach the parents that if any of the following signs develop, you should be called immediately or the baby should be taken at once for referral.
- Limbs become limp
- Stops feeding
- Has chest in drawing
- Has fever
- Is cold to touch
Management of Sepsis
In case of sepsis in a newborn, if the baby is taken to the ANM, she would treat the baby with a combination of Oral Amoxicillin+ Injectable Gentamicin [14]. If the ANM is not available or the referral facility is far off or the parents are not in a position to take the baby immediately, ASHA should start the treatment with Oral Amoxicillin (as described in the box below) and refer the baby to the facility. In such situations you should also:
- Counsel the mother/caregiver for urgent referral to the nearest health facility
- Arrange transport by calling ambulance services as part of the JSSK scheme Amoxicillin is available as Syrup formulation and dispensable tablets. Syrup (contains 125mg/5 ml) (Table 4).
| Daily Dose (to be divided into two equal parts and given twice daily) | |
|---|---|
| Less than 2.0 kg | 2 ml |
| Between 2.0 to 3.0 kg | 2.5 ml |
| Between 3.0 to 4.0 kg | 3 ml |
| Between 4.0 to 5.0 kg | 4 ml |
Table 4: Dosage- 25 mg/kg/dose in two divided doses. *You may use dropper or dispenser to measure the accurate dose. **Avoid amox
During referral to the health facility, there are certain steps that you can take to help the sick child
- Keep the baby warm by skin to skin contact with mother /care giver while arranging referral and during transport
- Ask mother to breastfeed the child frequently, this will help in maintaining blood sugar in child. Give 20-50 ml expressed breast milk if baby is not able to breastfeed.
When to refer the baby?
- Baby has breastfeeding problems and is not solved by ASHA’s counseling and home management after 24 hours.
- Baby has danger signs:
- Not responding – after antibiotic treatment for 24 hours.
- Becomes yellow (jaundice) on first day or jaundice persists after 14 days.
- Bleeding from nose, mouth or anus.
- Convulsions.
- Body temperature of baby continues to remain less that 95 degree F even after re-warming the baby for 24 hours.
- Tetanus (stiffness after the fourth day), unable to suckle or open mouth.
Conclusion
A life can be saved or lost in the five minutes of delivery. If ASHAs are present at the time of birth, and there is no doctor or nurse, ASHA will try to help to manage the baby. So, training and teaching of ASHAs on HBNC is very important to manage a newborn at home.
References
-
Wang H, Bhutta ZA, Coates MM, Coggeshall M, Dandona L, et al. (2016) Global, regional, National, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet 388(10053): 1725-1774.
-
(2016) Registrar General of India, Sample registration system (SRS) statistical report 2014, New Delhi.
-
Lassi ZS, Bhutta ZA (2015) Community-based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database Syst Rev (3): CD007754.
-
Bhutta ZA, Das JK, Bahl R, Lawn JE, Salamet RA, et al. (2014) Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet 384(9940): 347-370.
-
Reidpath DD, Allotey P (2003) Infant mortality rate as an indicator of population health. J Epidemiol Community Health 57(5): 344-346.
-
Schell CO, Rosling H, Peterson S, Mia Ekström A, Reilly M (2007) Socioeconomic determinants of infant mortality: a worldwide study of 152 low-, middle-, and high-income countries. Scand J Public Health 35(3): 288-297.
-
Al-Mazrou YY, Alhamdan NA, Alkotobi AI, Nour OM, Farag MA (2008) Factors affecting child mortality in Saudi Arabia. Saudi Med J 29(1): 102-106.
-
Kumar V, Mohanty S, Kumar A, Misra RP, Santosham M, et al. (2008) Effect of community-based behaviour change management on neonatal mortality in Shivgarh, Uttar Pradesh, India: a cluster-randomised controlled trial. Lancet 372(9644): 1151-1162.
-
Baqui AH, El-Arifeen S, Darmstadt GL, et al. (2008) Effect of community-based newborn-care intervention package implemented through two service-delivery strategies in Sylhet district, Bangladesh: a cluster-randomised controlled trial. Lancet 371(9628): 1936-1944.
-
Darmstadt GL, Choi Y, Arifeen SE, Bari S, Rahman SM, et al. (2010) Evaluation of a cluster-randomized controlled trial of a package of community-based maternal and newborn interventions in Mirzapur, Bangladesh. PLoS One 5(3): e9696.
-
Bhutta ZA, Soofi S, Cousens S, Mohammad S, Memon ZA, et al. (2011) Improvement of perinatal and newborn care in rural Pakistan through community-based strategies: a cluster-randomised effectiveness trial. Lancet 377(9763): 403-412.
-
Kirkwood BR, Manu A, ten Asbroek AHA, Soremekun S, Weobong B, et al. (2013) Effect of the Newhints home- visits intervention on neonatal mortality rate and care practices in Ghana: a cluster randomised controlled trial. Lancet 381(9884): 2184-2192.
-
Bhandari N, Mazumder S, Taneja S, Sommerfelt H, Strand TA, et al. (2012) Effect of implementation of integrated management of neonatal and childhood illness programme on neonatal and infant mortality: cluster randomised controlled trial. BMJ 344: e1634.
-
Gogia S, Sachdev HPS (2016) Home-based neonatal care by community health workers for preventing mortality in neonates in low- and middle-income countries: a systematic review. J Perinatol 36(1): S55-S73.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City