Hands on Skills of NPCCs in Critical Care: Views from NPCCs, Healthcare Professionals and Other Stakeholders
Introduction: As demand for nurse practitioners in all types of intensive care units continues to increase; ensuring successful integration of these nurses into general and specialty intensive care units poses several challenges. Adding nurse practitioners in critical care requires strategic planning to define critical aspects of the care delivery model, acceptability and autonomy before the practitioners are hired or utilized. Autonomy can be achieved when NPs’ ability to deliver care independently is encouraged, they are well accepted in critical care units by the health care professionals and other stakeholders and when NPCC perceive they are viewed and Treated by administrators as integral members of the care teams. Multiple quantitative studies revealed the attributes of NPs’ practice autonomy and roles. However, researcher has not come across any study to assess the critical care skills performed by Nurse Practitioner in critical Care (NPCC) in India. Methodology: A quantitative descriptive research approach was used to conduct study among 35 NPCCs, 80 healthcare professionals (excluding physician) and 15 physicians through purposive sampling techniques. An expressed checklist was used to assess the critical care skills performed by NPCCs after taking formal permission from the competent authority. Results: Majority of the NPCCs (71%) had good critical care skills whereas (29%) had average critical care skills. None of the NPCCs had poor critical care skills views from NPCCs Out of 15 physicians, majority of the subject (87%) revealed that NPCCs had good critical care skills whereas (13%) had average critical care skills. None of the NPCCs had poor critical care skills. Majority of the health care professionals (excluding physicians) & other stakeholders (86%) said that NPCCs had good critical care skills, (14%) had average critical care skills. None of the NPCCs had poor critical care skills. Majority of the physicians refuse to participate in the research study, only 15 physicians participated from selected institute of the research. Out of the15 physicians accept the NPCCs but found the curriculum not appropriate as per the need of the NPCCs. Conclusion: Nurse practitioners need to become more visible to both the public and other health care professionals. Continuing to educate and expose the public and other health care professionals to nurse practitioners will influence perceptions which, in turn, may increase interest in learning more about the role and affect acceptance of the role and utilization of the nurse practitioner in critical care. The utilization of NPCCs continues to have much room for expansion, allowing NPs more autonomy and involvement in the care of critical care patients, it is important for physicians and other health care providers to be familiar with the capabilities of a NPCCs in order for them to be utilized to their maximum potential
Introduction
The role of the nurse practitioner was first introduced in the United States ‘ health care system in 1965 and the role of nurse practitioners in the intensive care unit (ICU) has evolved considerably since the 1990s [1, 2, 3, 4, 5]. After early descriptions of the role of these nurses in pediatric and adult ICUs, delineation of role development in a variety of critical care settings and recent descriptions of successful orientation programs, models of care, and evidence of positive outcomes for nurse practitioners have strengthened the value of having the practitioners on the critical care team. Today, the use of nurse practitioners as mid-level providers continues to grow and has become a positive force in providing health care in any settings. Despite the increasing prevalence of nurse practitioners, Edmunds writes that the nurse practitioner is still unknown to many as a member of the health care team [6, 7]. As per the information of American Association Of Nurse Practitioners (AANP) there are more than 278000 NPs licensed in U.S. about 95.7 % of NPs prescribe medication and more in full time practice write an average of 20 prescription and majority around 57.4% see 3 or more patients per hour. Malpractice rates remain low, only 1.1%. The Bureau of Labour Statistic estimates the NPs profession will have grown by 36 % by 2026, compared to 37% for physician (excluding anesthesiologists and surgeon). As AANP president Joyce Knestrick found that “couple with news that NPs conducted an estimated 1.02 billion patient visits last year alone, and it’s easy to see why millions of Americans are making NPs their providers of choice [8].” Considering these findings and those of previous research, the nurse practitioner in Critical Care plays an important dimension in meeting today’s health care needs. It has been estimated that 50% to 90% of the activities performed by physicians can be delegated to nurse practitioners [9]. In 25 states, plus the District of Columbia, nurse practitioners can practice independently without physician collaboration or supervision; several organizations have published reports of successful integration of NPs into care delivery models for ICU providers [10].
In context of India, this program of NPCCs was under plan of INC in the year of 2015 & started by various colleges all over the country in the year 2017, it’s just a beginning, there is long way to cover. The nurse practitioners in India are working under the title of staff nurses and do not have the authority to prescribe the drugs or practice independently. Nurse practitioners are educated in the advanced practice of nursing, which incorporates medical skills needed for curing while maintaining their nursing skills of caring. Nurse practitioners bring with them a holistic and humanistic, patient centered practice that incorporates health maintenance and promotion, patient education, counseling, and advocacy [11]. Despite mounting evidence of effectiveness as health care providers, nurse practitioners continue to struggle for professionals’ acceptance. A major deterrent is a lack of understanding from health care professionals as well as the general public regarding the role of the nurse practitioner. Additional impediments include variations in education among nurse practitioners, consecutive concerns from physicians, legislative restrictions to practice, reimbursement policies and prescriptive authority controversies [12, 13]. Combinations of these Actions can result in the underutilization of nurse practitioner services. The continued successful merger of the nurse practitioner into the health care arena will largely depend on the understanding and acceptance of their role by physicians, other health care professionals, and patients and the researcher has not come across with such study in India so far. There is a need for health care professional’s awareness regarding the nurse practitioner in critical care & their scope of practice [14]. The present study aims to assess the acceptance, utilization and autonomy of the nurse practitioner in critical care among health care professionals and other stakeholders. Understanding of these three aspects is imperative in order to guide future education of the health care professionals and the ultimate goal of that education will be favorable integration and utilization of the nurse practitioner who can work independently in the critical care units at tertiary level with good team support.
Material and Methods
The research approach selected for the study was quantitative with descriptive survey research design. Non probability sampling technique was used for the selection of 110 samples. In the present study sample comprised of 35 NPCCs, 80 healthcare professionals (excluding physician) and 15 physicians of selected institutes from Uttar Pradesh (Tables 1,2), Uttarakhand, Madhya Pradesh and Punjab .Inclusion criteria included NPCCs who were placed in the same institute‘s hospital from where they took their training, Nurse who have practiced nursing for a minimum of 2 years, Health care professionals and other stakeholders in the hospitals where NPCC training provided. The study excluded the NPCCs students in their 1st year session and Healthcare professional who are not involved with NPCCs. The tool developed and used for data collection was five point Likert scale to assess the acceptability, autonomy and utilization of NPCCs among healthcare professionals (excluding physicians), stakeholders and physicians of selected institutes. Presently the prescription authority is given to only physician & medical practitioners in the country hence a separate tool was prepared for the physicians apart from health care professional. To ensure the validity of tool, it was given to 7 experts from the field of Medicine, Psychiatry, Community Health Nursing, Critical care Nursing and reliability of the tool was established by using chronbach’s alpha formula found to be 0.928. The duration data were collected from October, 2019 to November, 2019 of the study was one month. The samples were visited only once to collect the data and around 15 minutes was spend on each sample. The study protocol was approved by Jamia Hamdard institutional ethical committee. For ethical clearance and written informed consent was obtained from the subjects. The data obtained was tabulated in Microsoft excel spreadsheet and was analyzed in terms of objectives of the study using descriptive and inferential statistics (Figures 1,2).
Result
*n1=35
| Frequency (f) | Percentage (%) | |
|---|---|---|
| Age (in years) | ||
| 25-30 | 34 | 97.14 |
| 31-35 | 1 | 2.85 |
| Gender | ||
| Male | 20 | 57.14 |
| Female | 15 | 42.85 |
| Average Monthly family income (Rs.) | ||
| Less than Rs.20,000 | 10 | 28.57 |
| 20,001 – 30,000 | 15 | 42.85 |
| 30,001 – 40,000 | 4 | 11.42 |
| 40,001 – .50,000 | 3 | 8.57 |
| More than 50,000 | 3 | 8.57 |
| Professional experience in critical care(in years) | ||
| 1-4 | 32 | 91.42 |
| 1-8 | 2 | 5.71 |
| >12 | 1 | 2.85 |
Table 1: Frequency and percentage of demographic variables of Nurse Practitioners in Critical Care. *n1=NPCCs
| Health care professionals(excluding physicians) & stakeholders (n ) 2 | Physicians (n ) 3 | |||
|---|---|---|---|---|
| Variables | Frequency (f) | Percentage (%) | Frequency (f) | Percentage (%) |
| Gender | ||||
| Male | 31 | 38.75 | 8 | 53.33 |
| Female | 49 | 61.25 | 7 | 46.66 |
| Professional qualification | ||||
| Diploma | 23 | 28.75 | 0 | 0 |
| Graduate | 13 | 16.25 | 6 | 40 |
| Post-graduate | 42 | 52.5 | 7 | 46.66 |
| Doctorate | 2 | 2.5 | 2 | 13.33 |
| Designation | ||||
| Staff Nurses | 59 | 73.75 | 0 | 0 |
| Hospital Administrators | 10 | 12.5 | 0 | 0 |
| Nurse administrators | 11 | 13.75 | 0 | 0 |
| Physician | - | - | 15 | 100 |
| Professional experience in critical care(in years) | ||||
| 1-4 | 53 | 66.25 | 11 | 73.33 |
| 5-8 | 16 | 20 | 2 | 13.33 |
| 9-12 | 2 | 2.5 | 0 | 0 |
| More than 12 | 9 | 11.25 | 2 | 13.33 |
Table 2: Frequency and Percentage Distribution of Demographic Data of Health Care Professionals (excluding physician), stakeholde
Discussion
71% NPCCs viewed themselves accepted in critical care while 29 % was unsure about it .On ground of autonomy half of the samples 63% found high level of autonomy while working in ICU whereas 37 % were indecisive of it. The result of the study is similar to study conducted by K Sneha in selected Government institution of New Delhi used an opinionnaire about ANPCC program revealed that majority (96%) of nursing personnel were aware of ANPCC, only 4% were not aware (85% ) had positive opinion towards the prospects of ANPCC in India (95 %) of nursing personnel opined that there is a great need of ANPCC in India and 92 % agreed that doctors needs to collaborate with the training of ANPCC [15].
According to the Indian Nursing Council the Critical Care Nurse Practitioner Program will be for B.Sc nurses with a minimum of one year clinical experience which use competency based education that emphasizes clinical (80%) supported by didactic course work (20%). The two year program would lead to M.Sc. degree in critical care NP [5]. The use of nurse practitioners is expanding; however, perceptions remain mixed regarding the scope of practice. One physician returned a Questionnaire with a saying “I feel if nurses want to practice medicine they should go to medical school.” Attitudes such as these prevail, despite studies such as this one and the increasing use of nurse practitioners in critical care [16, 17] and on the other hand one physician respond very positively related to this issue, “I totally accepted the NPCCs but there is need to reconstruct the curriculum, their curriculum contain all the needed procedures but written haphazardly which need to be modify and this course required a specialized authority to trained the NPCCs & NPCCs need to have broad base of knowledge & competent enough to implement this course successfully” [18]. Most of the institutes don’t grant the permission for conducting research study which shows lack of interest to the subject of study. In contrast state nursing council recognized institutions offering nurse practitioner in critical care (NPCC) programme, in academic year 2017- 2018, there are 44 colleges are listed from all over India but half of institutes has less or no admission as per allotted seats to them, showing lack of awareness related to the course or people are already see the failure of NPs program in various other primary levels of the country [19]. Despite the research finding this is the subjective feeling of the researcher that there is no separate cadre of nurse practitioner in critical care and no extra salary for NPCCs even though it is highly demanding area of practice considering a important factors contributing to no or less admission in this course of NPCC.
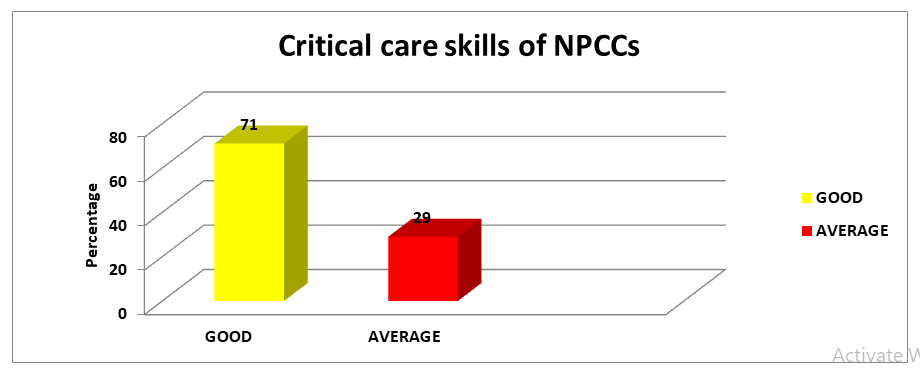
The data in Table No.9 describes the Frequency and Percentage distribution of assessment of skills performed in critical care by NPCCs. Majority of the NPCCs (71%) [20], had good critical care skills whereas (29%) had average critical care skills. None of the NPCCs had poor critical care skills.
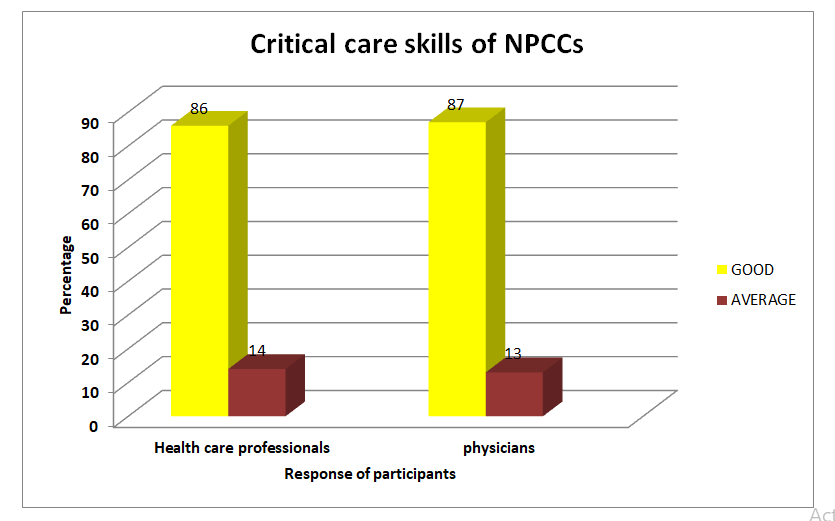
Out of 15 physicians, majority of the subject (87%) revealed that NPCCs had good critical care skills whereas (13%) had average critical care skills. None of the NPCCs had poor critical care skills. Majority of the health care professionals (excluding physicians) & other stakeholders (86%) said that NPCCs had good critical care skills, (14%) had average critical care skills. None of the NPCCs had poor critical care skills. (Figure 2)
Conclusion
Nurse practitioners need to become more visible to both the public and other health care professionals. Continuing to educate and expose the public and other health care professionals to nurse practitioners will influence perceptions which, in turn, may increase interest in learning more about the role and affect acceptance of the role and utilization of the nurse practitioner in critical care. The utilization of NPCCs continues to have much room for expansion, allowing NPs more autonomy and involvement in the care of critical care patients, it is important for physicians and other health care providers to be familiar with the capabilities of a NPCCs in order for them to be utilized to their maximum potential.
Acknowledgement
I express my deep sense of gratitude to my guide professor Urmila D. Bhardwaj, Principal of Rufaida college of nursing for the constant encouragement and guidance and Mr. Naseem Mancheri, Tutor, Rufaida college of nursing for critical evaluation throughout the study . It was a great privilege to work under them. I extend my immense gratitude to my guide and co-guide for their precious guidance throughout the study.
Conflict of Interest: None.
References
-
World Health Organization, Sudhir A, Victoria F (2016) The health workforce in India. World Health Organization.
-
Sharma DC (2015) India still struggles with rural doctor shortages. The Lancet 386(10011): 2381-2382.
-
WHO (2016) The 2016 update, Global Health Workforce Statistics, World Health Organization, Geneva.
-
Prashanth M, Putturaj M (2017) Enhancing the autonomy of Indian nurses. Indian J Med Ethics 2(4): 275-281.
-
INC (2016) Syllabus & Regulations; Nurse practitioner in critical care post graduate residency program, Indian Nursing Council, pp: 1-60.
-
Nanda L, Lobo E (2018) Nurse Practitioners – India’s Answer to Addressing Access to Healthcare. Public H Open Acc 2(2): 1-4.
-
Simone S, McComiskey CA, Andersen B (2016) Integrating Nurse Practitioners Into Intensive Care Units. Crit Care Nurse 36(6): 59-69.
-
AACN (2015) Outstanding dissertation and DNP Project awards, American Association of Colleges of Nursing.
-
Denicola L, Kleid D, Brink L (1994) Use of pediatric physician extenders in pediatric and neonatal intensive care units. Crit Care Med 22(11): 1856-1864.
-
CACCN (2011) Position statement: Nurse practitioner in critical care. Dynamics, Canadian Association of Critical Care Nurses 22(1): 12-13.
-
Bambini, Deborah R (1995) Nurse/Physician Perceptions of the Nurse Practitioner Role, Grand Valley State University, pp: 1-43.
-
James B, Marta T, Ines F, Luis L, Gilles D (2013) Nurses in advanced roles: a review of acceptability in Portugal, Rev. Latino-Am.Enfermagem 21(Spec): 38-46.
-
Chiayi C, Donna R, McNeese S, Marie C, Valda U, et al. (2009) Evaluation of a Nurse Practitioner- Led Care Management Model in Reducing Inpatient Drug Utilization and Cost. Nursing economics 27(3): 160-168.
-
Ruth K, Ward NS, Lynn A, Fred P, Douglas H (2015) Provider to Patient Ratios for Nurse Practitioners and Physician Assistants in Critical Care Units 24(3): e16-e21.
-
Leigh BP (2018) Feasibility And Acceptability Of Nurse Practitioner-Led Student Health Services On A Regional Campus Published by ProQuest LLC. University of South Carolina, pp: 1-70.
-
Lusine P, Jianfang L, Jingjing S, Thomas DA (2016) Practice environments and job satisfaction and turnover intentions of nurse practitioners: Implications for primary care workforce capacity. Health Care Manage Rev 42(2): 162-171.
-
Krishnan S (2018) A descriptive survey to assess the opinion of nursing personnel regarding the prospects and challenges of advance nurse practitioner in critical care in India in selected college and hospitals of Delhi. Masters Theses.
-
Gretch D (1999) Advanced practice nursing and the role of the pediatric critical care nurse practitioner. Crit Care 21(4): 16-21.
-
Catherine M (2017) Policies that restrict full utilization of nurse practitioners in primary care nursing economic. Nurs Econ 35(2): 71-99.
-
Bnana L (2011) Trauma nurse practitioners variations in utilization and role expansion jtn 10: 1097.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City