Associations of Molecular-Genetic Bioenergetics and Chemotherapy-Induced Fatigue Symptoms in Patients with Breast Cancer: A proposal development
Introduction: Cancer-related fatigue (CRF) occurs in 82%-96% of cancer patients receiving chemotherapy (CT). CT-induced CRF is a distressing, persistent sense of exhaustion related to the disease or its treatment, and negatively impacts health outcomes. CRF is one of the most prevalent side effects of CT in patients with breast cancer. Despite various attempts to investigate the etiology of CRF, the biochemical mechanisms remain elusive. Objectives: The study aims to explore the molecular-genetic pathway of mitochondrial bioenergetics and its association with CT-induced CRF. We hypothesized that the chemotherapeutic agent containing anthracycline targets cell cycle progression, which triggers genetic and cellular instability, altering expression of mitochondrial genes and proteins, inducing reduced electron transport chain enzymatic activity and impaired oxidative phosphorylation, resulting in adenosine triphosphate (ATP) depletion and excessive reactive oxygen species (ROS) generation, leading to the development and intensification of CRF. Methods: This is a prospective, hypothesis-testing, and longitudinal study design. A total of 60 patients with breast cancer undergoing CT will be enrolled. Validated instruments will be used to measure CRF, depression, sleep disturbance, and physical activity. Whole blood sample will be collected before, during, and at the completion of CT to determine profiles of mitochondrial bioenergetics. A linear mixed model repeated measures analysis will be used to examine associations between changes in study variables. Anticipated Results: Increased scores of CRF will be associated with altered mitochondria-related genes and mitochondrial bioenergetics (e.g., ↓oxidative phosphorylation, ↓electron transport chain complexes activity, ↓ATP content, and ↑ROS production) in patients receiving CT-containing anthracyclines. Conclusion: The results will enable us to discover biomarkers, support the design of nonpharmacological interventions, and initiate precision symptom management to improve CRF.
Introduction
Breast cancer is the most common malignancy and the second leading cause of cancer mortality among women in the United States [1]. Alongside surgery and radiotherapy, one of the primary treatment modalities for women with early-stage breast cancer is chemotherapy (CT), alone or combined with hormone therapy [2]. While CT has significantly increased survival rates with this disease, it carries adverse clinical complications, including neutropenia, alopecia, cardiomyopathy, muscle wasting, and fatigue [3, 4, 5, 6]. Of all treatment-related symptoms in cancer, fatigue is the most burdensome with the greatest adverse effect on quality of life [7, 8].
Defined by National Comprehensive Cancer Network (NCCN), cancer-related fatigue (CRF) is pervasive, a whole- body excessive tiredness unrelated to activity or exertion and not relieved by rest or sleep [9, 10]. CRF is very common during the treatment and causes long-lasting distress after the completion of treatment, even in disease-free stages [6, 11, 12, 13]. CRF negatively impacts health outcomes including depression, sleep disturbance, impaired cognitive function, decreased physical activity, and poor quality of life [14, 15, 16, 17]. Patients with breast cancer undergoing CT reported the poorest quality of life, with severe CRF, compared to those who received surgery or radiation therapy [18]. Factors that have been correlated with CRF severity in breast cancer patients receiving CT include depression, anxiety, poor sleep quality menopausal symptoms, and psycho-physiological factors [19, 20, 21]. Although various attempts have been made to investigate the etiology of CRF [22, 23, 24, 25, 26, 27, 28, 29, 30], the biochemical and pathophysiological mechanisms involved remain elusive. CT-induced CRF with multi-dimensions has not been well- characterized in patients with breast cancer.
There is no optimal effective pharmacologic therapy for CRF. The NCCN Practice Guidelines in Oncology for CRF currently recommend six nonpharmacological interventions: physical activity, physically based therapies, psychosocial interventions, nutrition consultation, cognitive behavioral therapy for sleep, and bright white light [9]. Using psychostimulants after other causes of CRF are ruled out that is the only pharmacologic intervention recommend by NCCN guidelines. Methylphenidate has been recommended, but two small, randomized clinical trials produced conflicting results [31]. With limited available options, evidence- based novel and precision strategies are needed to improve both pharmacologic and nonpharmacologic therapies for CRF. However, without a deeper more comprehensive understanding of precisely where and how CT impairs the metabolic cycle more robust testing of nutraceuticals, cannot be done. This study will provide that level of evidence.
Review of Literature
Previous studies have shown that nuclear genes regulating mitochondrial apoptosis, biogenesis, and bioenergetics in peripheral blood mononuclear cells (PBMCs) were associated with worsened CRF in prostate cancer patients receiving radiotherapy [32, 33]. PBMCs of fatigued patients with cancer showed reduced ATP coupling efficiency compared to those without fatigue [34]. Platelet bioenergetics correlated with muscle energetics and fatigability in older adult [35]. Deficiency of adenosine triphosphate (ATP) has been proposed as the basis of fatigue in patients with cancer and chronic fatigue syndrome [36, 37]. The mitochondrial respiratory chain is essential to produce and maintain an effective cell content of ATP [38, 39]. Mitochondria generate 90% of ATP via oxidative phosphorylation (OXPHOS) and convert 0.4% to 5% of superoxide (O2-) radical during normal mitochondrial OXPHOS. Mitochondria are vulnerable to reactive oxygen species (ROS), which are generated endogenously (e.g., mitochondrial superoxide) and exogenously (e.g., ionizing radiation, inflammation) [39].
Chemotherapeutic agents target rapidly dividing mitotic cells, trigger apoptosis, and cause the generation of excess ROS, which has been associated with mitochondrial dysfunction through increased mitochondrial ROS [4, 40, 41]. Doxorubicin is an effective antineoplastic agent and potent anthracycline antibiotic, and is widely used as a component of multiple-drug CT for breast cancer [42]. The cardiotoxicity of doxorubicin is characterized by a dose-dependent decline in cardiac function through increased ROS production in mitochondrial cardiac muscle [43]. Studies showed that epirubicin and doxorubicin induce a decrease in muscle strength and an accelerated rate of fatigue by interrupting mitochondrial energy metabolism and redox balance [42], as well as an associated worse quality of life [6]. Raised levels of ROS have also been associated with symptom development in patients with chronic fatigue syndrome [44]. CT has been associated with mitochondria dysfunction via increased mitochondrial ROS [45], eliciting significant side effects, including muscle fatigue [46]. ROS is considered one of the major, direct causes of ionizing radiation-induced damage [47], resulting in a number of adverse effects, including fatigue [48].
Both CT drugs and radiation-induced damage alter mitochondrial metabolism, inhibit the mitochondrial respiratory chain, and form highly reactive peroxynitrite (ONO2-) [49, 50]. Once mitochondrial proteins are damaged, the affinity of substrates or enzymes is decreased, resulting in mitochondrial dysfunction [38]. However, the studies that produced these findings did not identify the mechanism of inhibiting the mitochondrial respiratory chain related to mitochondrial dysfunction and CRF after CT.
Preliminary Findings
Our preliminary work revealed that, over time, 14 mitochondrial-related genes were differentially expressed in men with localized prostate cancer during radiation therapy [33]. One downregulated gene, BC1 (ubiquinol- cytochrome c reductase) synthesis-like (BCS1L), and three upregulated genes: BCL2-like1 (BCL2L1); solute carrier family 25, member 37 (SLC25A37); and fission 1 homolog (S. cerevisiae) (FIS1); were associated with increased CRF (β = 1.3-2.4, p = 0.001- 0.002) at the end of treatment compared to baseline [32]. Altered expression of these genes was accompanied by changes of protein concentrations [32, 33]. Worsened CRF was associated with impaired OXPHOS via complex III deficiency during radiotherapy in patients with prostate cancer [51, 52, 53]. BCS1L plays an important role in the assembly of complex III in the mitochondrial electron transport chain (ETC), which is essential for maintaining effective ATP levels [39, 54].
Mitochondrial OXPHOS enzymes, proteins, and lipids are vulnerable to free radicals [55]. A defect in complex III leads to a functional deficit in the respiratory chain and impairs ATP production [54]. BCL2L1 is located on the mitochondrial outer membrane, regulating the opening of the membrane’s voltage-dependent anion channel, controlling the production of ROS, and inducing cellular apoptosis [56]. SLC25A37 is a solute carrier localized in the mitochondrial inner membrane that serves as the principal iron importer. SLC25A37 plays a critical role in iron-consuming processes, including heme synthesis and Fe-S cluster synthesis in mitochondria [57, 58]. Overexpression of SLC25A37 leads to increased iron uptake into mitochondria and promotes heme synthesis [58]; this increased matrix-free iron potentially increases hydroxyl radical formation from hydrogen peroxide and results in mitochondrial dysfunction [59, 60]. In summary, our preliminary studies established that CRF is associated with mitochondria-related genes and impaired bioenergetics (e.g., ↓OXPHOS) in fatigued men treated with radiation therapy [32, 33, 52].
Characterization of both phenotype and molecular/ genotype of CT-induced CRF is imperative but has not been explored. We propose to investigate the molecular-genetic pathway of mitochondrial bioenergetics and its association with CT-induced CRF symptoms experienced by patients with breast cancer receiving CT-containing anthracyclines, compared to those with non-anthracycline-based CT. Understanding the mechanism/pathway underpinning CRF will enable the design of targeted therapeutics and non- pharmacological interventions, as well as to advance the science of symptom management.
Specific Aims
Our specific aims are to (1) characterize the profile of mitochondria-related genes associated with CRF symptoms, and (2) identify the profile of mitochondrial bioenergetics associated with CRF symptoms in patients with breast cancer receiving anthracycline-based CT, compared to patients with non-anthracycline-based CT at baseline, midpoint, and endpoint of CT, as presented in Figure 1.
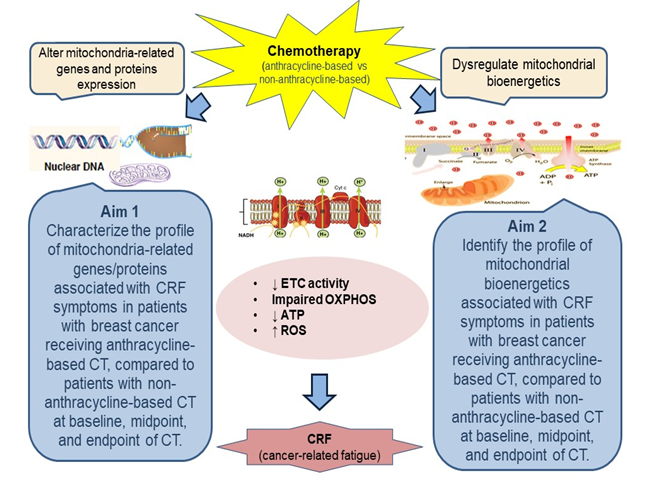
Hypothesis
We hypothesize that the chemotherapeutic agent containing anthracyclines will trigger changes in mitochondria-related genes and proteins, inducing a defect in ETC activity and impaired OXPHOS, leading to ATP depletion and excessive ROS generation, which are associated with developing and debilitating CRF.
Materials and Methods
This study is under reviewed by the Institutional Review Board (IRB) of University Hospitals and Case Comprehensive Cancer Center.
Design
This is a prospective, hypothesis-testing project using a longitudinal research design in patients with breast cancer receiving CT-containing anthracyclines (doxorubicin, epirubicin), compared to those with non-anthracycline- based regimens.
Sample and Setting
The study sample will be recruited from a population of breast cancer patients scheduled for CT. The study will be introduced to collaborating clinicians during one-on-one or team meetings at the study site, University Hospitals Seidman Cancer Center. The inclusion criteria are: (a) clinically confirmed early-stage (I-III) breast cancer; (b) anthracycline- based CT naive; (c) scheduled to receive a CT regimen with anthracycline-based (e.g., doxorubicin, cyclophosphamide, paclitaxel) or non-anthracycline regimen (e.g., docetaxel, cyclophosphamide); (d) able to provide written informed consent; and (e) ≥18 years of age. The exclusion criteria include: (a) progressive or unstable disease other than cancer of any body system causing clinically significant fatigue (e.g., class IV congestive heart failure, end-stage renal disease, stage IV chronic obstructive pulmonary disease), including systemic infections (e.g., HIV, active hepatitis, active COVID-19); documented recent (< 6 months) history of major depression, bipolar disease, psychosis, or alcohol/ drug dependence/abuse; uncorrected hypothyroidism; untreated anemia; or chronic inflammatory disease (e.g., rheumatoid arthritis, systemic lupus erythematosus); (b) regularly taking antipsychotics or anticonvulsants, since these medications cause significant fatigue; (c) presence of second malignancies; (d) presence of mitochondrial disease; or (e) taking medication for fatigue (e.g., methylphenidate, moldafinil).
Sample size: We plan to enroll a total of 60 subjects (30 with anthracycline-based and 30 with non-anthracycline-based CT), which accounts for an attrition rate of 15-20% similar to previous studies [61, 62].
Power analysis: Based on our preliminary work, the BCS1L expression values (mean + SD) at baseline, midpoint, and endpoint were 6.76+1.29, 7.88+1.63, and 7.89+1.36, respectively, in cancer patients with treatment, and changes from baseline to midpoint and endpoint were -1.12+0.93 and -1.13+0.85. With 50 patients (25 per group) treated with CT, there is >95% power to detect a significant increase in CRF during treatment and mean changes in BCS1L of -1.12 and -1.13 at the midpoint and endpoint, similar to results revealed in our pilot data, assuming similar standard deviations will be observed. The power is 80% to detect a mean change of -0.56, which is 50% of the effect seen in our pilot data. In addition, CRF severity increased significantly at midpoint (↑2.06+0.06, p< 0.05) and endpoint (↑2.71+0.14, p< 0.01) compared to baseline (1.45 +0.29) [51, 53], similar to the findings from patients with breast cancer receiving CT [63, 64]. Breast cancer patients receiving anthracycline-based CT experienced CRF severity increased threefold at the cycle 4 compared to baseline [65]. Assuming changes in CRF from baseline to endpoint in patients with anthracycline-based CT is twofold higher than those with non-anthracycline-based CT, the analytic sample size is expected to provide 80% power to detect a clinically meaningful difference of 3.4 in CRF changes from baseline to the endpoint between subjects with and without anthracycline-based CT. All calculations presented assume 2-sided tests with a significance level of 0.05.
Feasibility: The tumor registry of the study site shows that, in 2021, a total of 96 new patients with breast cancer were treated with CT at the University Hospitals Seidman Cancer Center. Assuming a 25% refusal rate and 10% ineligible rate as found in previous studies [61, 62], this accrual rate (65%) would result in 60 patients with CT enrolled during the 12 month recruitment period.
Procedure
Data collection: CT for breast cancer patients usually is administered every 3 weeks for six cycles. To represent different phases of the CT and reflect the peak time of CRF, we chose three times to collect data: (1) baseline (prior CT, Day 0); (2) midpoint (during CT, Day 61-70, 3rd cycle of CT); and (3) endpoint (upon completion of CT, Day 126-140, 6th cycle of CT) [11]. Before starting the study, subjects will be screened for eligibility and then scheduled for data collection at their most convenient times. It will take less than an hour to complete all measures and blood work at each study visit. All tests and study visits will be conducted at the University Hospitals Seidman Cancer Center. Figure 2 presents the study procedure.

Blood draws and self-administered questionnaires will be coordinated with the patient’s schedule for infusion. A total of 45 mL of blood will be collected at each time point from each subject. Blood samples will be kept at room temperature after collection and during transport to the mitochondrial research laboratory. PBMCs and platelets will be harvested from fresh blood anticoagulated with ethylenediaminetetraacetic acid (EDTA) within 24 hours after blood samples are collected, and either assayed immediately for bioenergetics or stored at -80ºC in a freezer for RNA extraction.
Study measures: biological and behavioral/psychosocial instruments. Demographics and clinical data (e.g., CT regimens, medications, CBC), as well as depression, sleep, and physical activity as covariates, will be collected.
Biological measures include (1) mitochondria-related gene/protein expression: (a) total ribonucleic acid (RNA) concentration, purity, and integrity will be tested after RNA extraction [26]. Extracted RNA will be converted to cDNA (complementary DNA) and stored at -20ºC until ready for gene expression. (b) Quantitative real time polymerase chain reaction (RT-PCR) will be used to detect expression values and changes in differentiated genes of mitochondrial bioenergetics. (c) Enzyme-linked immunoassay (ELISA) will be used to measure protein concentrations of differentiated genes, and data will be normalized and read in a microplate reader. (2) Mitochondrial bioenergetics: (a) the OXPHOS rate will be measured using validated protocols in the O2k high- resolution respirometry system [66, 67]. The oxygraphy-2k (O2k, OROBOROS Instruments, Austria)) system provides robustness and reliability of instrumental performance, and has unique specifications; the limit of detection of respiratory flux is 1 pmol∙s--1∙cm-¬3 (0.001 µM∙s-¬1) [68]. (b) ETC enzymatic activity will measured using spectrophotometry with validated protocols [67, 69]. (c) The ATP content will be measured by bioluminescence assay; fluorometric method will be used to quantify the ROS production [70, 71].
Behavioral and psychosocial assessments include (1) CRF: The revised Piper Fatigue Scale is a 22-item, paper/ pencil questionnaire with excellent reliability and validity;
specifically to measure multidimensions (i.e., severity, sensory, cognitive, and affective) of CRF in cancer patients [72]. CRF is defined as a score of > 6 [73, 74]. (2) Depression: The Hamilton Depression Rating Scale is a clinician-rated paper questionnaire with 21-item, assessing the severity of depressive symptoms. Scores can range from 0 to 78; higher scores (> 17) [75] indicate greater severity of depressive symptoms. (3) Sleep: The Pittsburgh Sleep Quality Index is a 19-item index with high validity and reliability that measures subjective sleep quality [76]. (4) Physical activity: The International Physical Activity Questionnaire is a well- validated, 7-item, self-report questionnaire that gauges physical activity levels for the past 7 days [77].
Statistical Approaches and Analysis
The study objective is to examine the associations among mitochondrial genes, bioenergetics, and CRF symptoms over time in breast cancer patients receiving CT, and to compare differences in the profiles of gene expression, bioenergetics and CRF between patients with anthracycline-based CT and with non-anthracycline-based CT at baseline, midpoint, and endpoint of CT. When calculating summary scores for outcomes (e.g., Piper Fatigue Scale) based on summing scores of multiple items, unless specified otherwise in the documentation supplied for each measure, missing data in individual items will be handled by the following algorithm. If more than 50% of the items are missing, then the entire summary measure will be set to missing. If fewer than 50% of the items are missing, then the score will be computed after imputing the mean of the non-missing items for each non-missing item. To account for missing outcome variables, sensitivity will be analyzed using multiple imputations of follow-up outcomes with an inclusive strategy of analyzing more baseline variables in the imputation model [78]. We will use the Benjamin-Hochberg method for controlling the false discovery rate for each outcome, allowing for multiple testing.
Descriptive statistics (means, standard deviation, median, and range) will be used to summarize expression levels of differentiated genes and different dimensions of CRF at each time point. Data will be transformed using log or other transformations, if necessary, to better fit normality assumptions. Pearson or Spearman correlations will be used to examine the associations of CRF dimensions with expression of differentiated genes (Aim 1) and mitochondrial bioenergetics (Aim 2) at each time point. To compare the difference in gene expression, bioenergetics, and CRF severity between the CT group (anthracycline-based vs. non- anthracycline-based), we will use two-sample independent t-tests/Wilcoxon rank sum tests at each time point. Both aims will be analyzed using a linear mixed model repeated measures analysis to examine associations between changes in CRF dimensions and changes in expression of differentiated genes (Aim 1) and changes in mitochondrial bioenergetics (Aim 2) over time. The linear mixed model will be included the CT group to assess group differences and the interaction term (CT group by change in expression of the differentiated gene for Aim 1 and CT group by change in bioenergetics for Aim 2) whether changes in CRF outcomes varied differently in changes in gene expression/bioenergetics between subjects with and without anthracycline-based CT. Further, to identify the important covariates, we will test one covariate (e.g., CT cycles, hormone therapy, depression, sleep, physical activity, age, and race) at a time to identify if the covariate has an impact on the analyses. In the linear mixed model, we will include identified covariates in the models to control for their effects. Statistical analyses will be performed using SAS version 9.4 (SAS Institute Inc., Cary, NC) and SPSS version.
Anticipated Results
Compared to the baseline and those with non- anthracyclines, we expect to find increased/worsened CRF with different dimensions, altered mitochondrial gene expression (p < 0.05, > twofold change), and decreased bioenergetics (e.g., ↓oxidative phosphorylation, ↓electron transport chain complexes activity, ↓ATP content, and ↑ROS production) at midpoint and endpoint in patients receiving CT-containing anthracyclines. Furthermore, increased scores from different dimensions of CRF will be associated with altered mitochondrial genes; reduced OXPHOS, ETC activity, ATP content; and increased ROS.
Conclusion
We proposed a novel mechanism of mitochondrial bioenergetics for CT-induced CRF using molecular-genetic approaches. This will be the first study to determine the role of mitochondrial bioenergetics and its association with the development of debilitating CT-induced CRF. Currently, there are no effective and optimal evidence-based interventions for CRF. This research project is an essential step in pursuing a novel hypothesis designed to reveal the physiologic mechanisms of CRF, a ubiquitous cause of patient distress. There is some promising evidence that nutritional supplements can target relevant energy-producing processing, including ascorbic acid, niacin, vitamin E, and coenzyme Q10 [79].
Establishing the association of mitochondrial bioenergetics with CRF will provide a key foundation for devising clinical trials, such as cytoprotective interventions ranging from delivery of antioxidants to enhance individual antioxidant compacity to reduce ROS-related cellular damage and improve CRF.
Acknowledgements
This research project was supported by National Institutes of Health, National Institute of Nursing Research (1R21NR020226)
References
-
(2022) Society AC, Cancer Facts & Figures 2022-American Cancer Society, pp: 1-77.
-
Gradishar WJ, Anderson BO, Balassanian R, Blair SL, Burstein HJ, et al. (2018) Breast Cancer, Version 4.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 16(3): 310-320.
-
Rybalka E, Timpani CA, Cheregi BD, Sorensen JC, Nurgali K, et al. (2017) Chemotherapeutic agents induce mitochondrial superoxide production and toxicity but do not alter respiration in skeletal muscle in vitro. Mitochondrion 42: 33-49.
-
Conklin KA (2004) Chemotherapy-Associated Oxidative Stress: Impact on. Integrative Cancer Therapies 3(4): 294-300.
-
Tao JJ, Visvanathan K, Wolff AC (2015) Long term side effects of adjuvant chemotherapy in patients with early breast cancer. The Breast 24(02): 149-153.
-
Schwentner L, Harbeck N, Singer S, Eichler M, Rack B, et al. (2016) Short term quality of life with epirubicin- fluorouracil-cyclophosphamid (FEC) and sequential epirubicin/cyclophosphamid-docetaxel (EC-DOC) chemotherapy in patients with primary breast cancer – Results from the prospective multi-center randomized ADEBAR trial. The Breast 27: 69-77.
-
Blackhall L, Petroni G, Shu J, Baum L, Farace E (2009) A Pilot Study Evaluating the Safety and Efficacy of Modafinil for Cancer-Related Fatigue. Journal of Palliative Medicine 12(5): 433-439.
-
Langston B, Armes J, Levy A, Tidey E, Ream E (2013) The prevalence and severity of fatigue in men with prostate cancer: a systematic review of the literature. Supportive Care in Cancer 21(6): 1761-171.
-
(2021) National Comprehensive Cancer Network, Cancer-Related Fatigue. National Comprehensive Cancer Network Practice Guidelines in Oncology.
-
Piper BF, Cella D (2010) Cancer-related fatigue: definitions and clinical subtypes. J Natl Compr Canc Netw 8(8): 958-966.
-
Fabi A, Falcicchio C, Giannarelli D, Maggi G, Cognetti F, et al. (2017) The course of cancer related fatigue up to ten years in early breast cancer patients: What impact in clinical practice? The Breast 34: 44-52.
-
O’ Regan P, Hegarty J (2017) The importance of self-care for fatigue amongst patients undergoing chemotherapy for primary cancer. European Journal of Oncology Nursing 28: 47-55.
-
Rotonda C, Guillemin F, Bonnetain F, Conroy T, et al. (2011) Factors correlated with fatigue in breast cancer patients before, during and after adjuvant chemotherapy: The FATSEIN study. Contemporary Clinical Trials 32(2): 244-249.
-
Byar KL, Berger AM, Bakken SL, Cetak MA, et al. (2006) Impact of adjuvant breast cancer chemotherapy on fatigue, other symptoms, and quality of life. Oncol Nurs Forum 33(1): 18-26.
-
Berger AM, Mitchell SA (2008) Modifying cancer-related fatigue by optimizing sleep quality. J Natl Compr Canc Netw 6(1): 3-13.
-
Monga U, Kerrigan AJ, Thornby J, Monga TN, et al. (1999) Prospective study of fatigue in localized prostate cancer patients undergoing radiotherapy. Radiat Oncol Investig 7(3): 178-185.
-
Pinto BM, Dunsiger S, Waldemore M (2013) Physical activity and psychosocial benefits among breast cancer patients. Psychooncology 22(10): 2193-2199.
-
Wöckel A, Schwentner L, Krockenberger M, Kreienberg R, Janniet W, et al. (2017) Predictors of the course of quality of life during therapy in women with primary breast cancer. Quality of Life Research 26(8): 2201-2208.
-
Fisher HM, Jacobs JM, Taub CJ, Lechner SC, Lewis JE, et al. (2017) How changes in physical activity relate to fatigue interference, mood, and quality of life during treatment for non-metastatic breast cancer. General Hospital Psychiatry 49(Supplement C): 37-43.
-
Von Ah DM, Kang DH, Carpenter JS (2008) Predictors of Cancer-Related Fatigue in Women With Breast Cancer Before, During, and After Adjuvant Therapy. Cancer Nursing 31(2): 134-144.
-
Downie FP, Mar Fan HG, Tchen NH, Yi Q, Tannock IF (2006) Cognitive function, fatigue, and menopausal symptoms in breast cancer patients receiving adjuvant chemotherapy: evaluation with patient interview after formal assessment. Psychooncology 15(10): 921-930.
-
St Pierre BA, Kasper CE, Lindsey AM (1992) Fatigue mechanisms in patients with cancer: effects of tumor necrosis factor and exercise on skeletal muscle. Oncol Nurs Forum 19(3): 419-425.
-
Monga U, Jaweed M, Kerrigan AJ, Lawhon L, Johnson J, et al. (1997) Neuromuscular fatigue in prostate cancer patients undergoing radiation therapy. Arch Phys Med Rehabil 78(9): 961-966.
-
Ryan JL, Carroll JK, Ryan EP, Mustian KM, Kevin Fiscella JL, et al. (2007) Mechanisms of Cancer-Related Fatigue. The Oncologist 12(suppl 1): 22-34.
-
Yavuzsen T, Davis MP, Ranganathan VK, Walsh D, Siemionow V, et al. (2009) Cancer-related fatigue: central or peripheral? J Pain Symptom Manage 38(4): 587-596.
-
Saligan LN, Hsiao CP, Wang D, Wang XM, St John L, et al. (2013) Upregulation of alpha-synuclein during localized radiation therapy signals the association of cancer- related fatigue with the activation of inflammatory and neuroprotective pathways. Brain Behav Immun 27(1): 63-70.
-
Bower JE, Ganz PA, Tao ML, Hu W, Belin TR, et al. (2009) Inflammatory Biomarkers and Fatigue during Radiation Therapy for Breast and Prostate Cancer. Clinical Cancer Research 15(17): 5534-5540.
-
Bower JE, Ganz PA, Irwin MR, Arevalo JMG, Cole SW, et al. (2011) Fatigue and gene expression in human leukocytes: increased NF-kappaB and decreased glucocorticoid signaling in breast cancer survivors with persistent fatigue. Brain Behav Immun 25(1): 147-150.
-
Orre IJ, Reinertsen KV, Aukrust P, Dahl AA, Fosså SD, et al. (2011) Higher levels of fatigue are associated with higher CRP levels in disease-free breast cancer survivors. J Psychosom Res 71(3): 136-141.
-
Okunieff P, Chen Y, Maguire DJ, Huser AK, et al. (2008) Molecular Markers of Radiation-related Normal Tissue Toxicity. Cancer metastasis reviews 27(3): 363-374.
-
Bruera E, Valero V, Driver L, Shen L, Willey J, et al. (2006) Patient-controlled methylphenidate for cancer fatigue: a double-blind, randomized, placebo-controlled trial. J Clin Oncol 24(13): 2073-2078.
-
Hsiao CP, Wang D, Kaushal A, Chen MK, Saligan L, et al. (2014) Differential Expression of Genes Related to Mitochondrial Biogenesis and Bioenergetics in Fatigued Prostate Cancer Men Receiving External Beam Radiation Therapy. Journal of pain and symptom management 48(6): 1080-1090.
-
Hsiao CP, Wang D, Kaushal A, Saligan L (2013) Mitochondria-Related Gene Expression Changes Are Associated With Fatigue in Patients With Nonmetastatic Prostate Cancer Receiving External Beam Radiation Therapy. Cancer Nursing 36(3): 189-197.
-
Feng LR, Wolff BS, Liwang J, Regan JM, Alshawi S, et al. (2020) Cancer‑related fatigue during combined treatment of androgen deprivation therapy and radiotherapy is associated with mitochondrial dysfunction. International journal of molecular medicine 45(2): 485-496.
-
Braganza A, Corey CG, Santanasto AJ, Distefano G, Coen PM, et al. (2019) Platelet bioenergetics correlate with muscle energetics and are altered in older adults. JCI insight 5(13): e128248.
-
Myhill SN, Booth NE, McLaren Howard J (2009) Chronic fatigue syndrome and mitochondrial dysfunction. Int J Clin Exp Med 2(1): 1-16.
-
Agteresch HJ, Rietveld T, Kerkhofs LGM, van den Berg JWO, Paul Wilson JH, et al. (2002) Beneficial Effects of Adenosine Triphosphate on Nutritional Status in Advanced Lung Cancer Patients: A Randomized Clinical Trial. Journal of Clinical Oncology 20(2): 371-378.
-
Pieczenik SR, Neustadt J (2007) Mitochondrial dysfunction and molecular pathways of disease. Exp Mol Pathol 83(1): 84-92.
-
Mandelker L (2008) Introduction to oxidative stress and mitochondrial dysfunction. Vet Clin North Am Small Anim Pract 38(1): 1-30.
-
Sorensen JC, Cheregi BD, Timpani CA, Nurgali K, Hayes A, et al. (2016) Mitochondria: Inadvertent targets in chemotherapy-induced skeletal muscle toxicity and wasting. Cancer Chemotherapy and Pharmacology 78(4): 673-683.
-
Kenneth AC (2004) Chemotherapy-Associated Oxidative Stress: Impact on Chemotherapeutic Effectiveness. Integrative Cancer Therapies 3(4): 294-300.
-
Gilliam LAA, Fisher Wellman KH, Lin CT, Maples JM, Cathey BL, et al., (2013) The anticancer agent doxorubicin disrupts mitochondrial energy metabolism and redox balance in skeletal muscle. Free Radical Biology and Medicine 65: 988-996.
-
Sarvazyan N (1996) Visualization of doxorubicin- induced oxidative stress in isolated cardiac myocytes. American Journal of Physiology-Heart and Circulatory Physiology 271(5): H2079-H2085.
-
Kennedy G, Spence VA, McLaren M, Hill A, Underwood C, et al. (2005) Oxidative stress levels are raised in chronic fatigue syndrome and are associated with clinical symptoms. Free Radical Biology and Medicine 39(5): 584-589.
-
Sarosiek KA, Chonghaile TNi, Letai A (2013) Mitochondria: gatekeepers of response to chemotherapy. Trends Cell Biol 23(12): 612-619.
-
Gilliam LA, St Clair DK (2011) Chemotherapy-induced weakness and fatigue in skeletal muscle: the role of oxidative stress. Antioxid Redox Signal 15(9): 2543- 2563.
-
Zhao W, Robbins ME (2009) Inflammation and chronic oxidative stress in radiation-induced late normal tissue injury: therapeutic implications. Curr Med Chem 16(2): 130-143.
-
Nicolson GL, Conklin KA (2008) Reversing mitochondrial dysfunction, fatigue and the adverse effects of chemotherapy of metastatic disease by molecular replacement therapy. Clin Exp Metastasis 25(2): 161- 169.
-
Zabbarova I, Kanai A (2008) Targeted delivery of radioprotective agents to mitochondria. Mol Interv 8(6): 294-302.
-
Sarosiek KA, Chonghaile TN, Letai A (2013) Mitochondria: gatekeepers of response to chemotherapy. Trends in cell biology 23(12): 612-619.
-
Hsiao CP, Chen MK, Daly B, Hoppel C (2018) Integrated mitochondrial function and cancer-related fatigue in men with prostate cancer undergoing radiation therapy. Cancer Manag Res 10: 6367-6377.
-
Pagan J (2017) Mitochondrial Bioenergetics Profile Indicates Likelihood of Radiation-Induced Fatigue in Prostate Cancer. ONS Annual Congress, Oncology Nurse Advisor: Denver, Colorado.
-
Hsiao CP, Chen MK, Veigl ML, Ellis R, Cooney M, et al. (2019) Relationships between expression of BCS1L, mitochondrial bioenergetics, and fatigue among patients with prostate cancer. Cancer Manag Res 11: 6703-6717.
-
Hinson JT, Fantin VR, Schönberger J, Breivik N, Siem G, et al. (2007) Missense Mutations in the BCS1L Gene as a Cause of the Björnstad Syndrome. N Engl J Med 356(8): 809-819.
-
Shigenaga MK, Hagen TM, Ames BN (1994) Oxidative damage and mitochondrial decay in aging. Proc Natl Acad Sci USA 91(23): 10771-10778.
-
Vander Heiden MG, Chandel NS, Williamson EK, Schumacker PT, Thompson CB (1997) Bcl-xL Regulates the Membrane Potential and Volume Homeostasis of Mitochondria. Cell 91(5): 627-637.
-
Shaw GC, Cope JJ, Li L, Corson K, Hersey C, et al. (2006) Mitoferrin is essential for erythroid iron assimilation. Nature 440(7080): 96-100.
-
Lill R, Diekert K, Kaut A, Lange H, Pelzer W, et al. (1999) The Essential Role of Mitochondria in the Biogenesis of Cellular Iron-Sulfur Proteins. Biol Chem 380(10): 1157- 1166.
-
Liu L, Rissling M, Natarajan L, Fiorentino L, Mills PL, et al. (2012) The longitudinal relationship between fatigue and sleep in breast cancer patients undergoing chemotherapy. Sleep 35(2): 237-245.
-
Sripetchwandee J, Sanit J, Chattipakorn N, Chattipakorn SC (2013) Mitochondrial calcium uniporter blocker effectively prevents brain mitochondrial dysfunction caused by iron overload. Life Sci 92(4-5): 298-304.
-
Oh PJ, Jung-Ran C (2020) Changes in Fatigue, Psychological Distress, and Quality of Life After Chemotherapy in Women with Breast Cancer: A Prospective Study. Cancer Nurs 43(1): 54-60.
-
Whisenant M, Wong B, Mitchell SA, Susan LB, Mooney K, et al. (2017) Distinct Trajectories of Fatigue and Sleep Disturbance in Women Receiving Chemotherapy for Breast Cancer. Oncol Nurs Forum 44(6): 739-750.
-
Goedendorp MM, Andrykowski MA, Donovan KA, Jim HS, Phillips KM, et al. (2012) prolonged impact of chemotherapy on fatigue in breast cancer survivors: a longitudinal comparison with radiotherapy-treated breast cancer survivors and noncancer controls. Cancer 118(15): 3833-3841.
-
Bower JE, Wiley J, Petersen L, Irwin MR, Ganz PA, et al. (2018) Fatigue after breast cancer treatment: Biobehavioral predictors of fatigue trajectories. Health Psychol 37(11): 1025-1034.
-
Mills PJ, Parker B, Dimsdale JE, Sadler GR, Ancoli-Israel S, et al. (2005) the relationship between fatigue and quality of life and inflammation during anthracycline- based chemotherapy in breast cancer. Biol Psychol 69(1): 85-96.
-
Ye F, Hoppel CL (2013) Measuring oxidative phosphorylation in human skin fibroblasts. Anal Biochem 437(1): 52-58.
-
Hsiao CP, Hoppel C (2018) Analyzing mitochondrial function in human peripheral blood mononuclear cells. Analytical Biochemistry 549: 12-20.
-
Gnaiger E (2008) Polarographic oxygen sensors, the oxygraph and high-resolution respirometry to assess mitochondrial function. In: Yvonne W, Dykens JA (Eds.), Drug-Induced Mitochondrial Dysfunction, John Wiley, pp: 327-352.
-
Krahenbuhl S, Chang M, Brass EP, Hoppel CL (1991) Decreased activities of ubiquinol:ferricytochrome c oxidoreductase (complex III) and ferrocytochrome c:oxygen oxidoreductase (complex IV) in liver mitochondria from rats with hydroxycobalamin [c-lactam]-induced methylmalonic aciduria. J Biol Chem 266(31): 20998-21003.
-
Moghaddas S, Hoppel CL, Lesnefsky EJ (2003) Aging defect at the QO site of complex III augments oxyradical production in rat heart interfibrillar mitochondria. Arch Biochem Biophys 414(1): 59-66.
-
Chen Q, Vazquez EJ, Moghaddas S, Hoppel CL, Lesnefsky EJ, et al. (2003) Production of Reactive Oxygen Species by Mitochondria: Central Role of Complex III. J Biol Chem 278(38): 36027-36031.
-
Lundgren-Nilsson Å, Dencker A, Jakobsson S, Charles T, Tennant A, et al. (2014) Construct Validity of the Swedish Version of the Revised Piper Fatigue Scale in an Oncology Sample-A Rasch Analysis. Value Health 17(4): 360-363.
-
Piper BF, Dibble SL, Dodd MJ, Weiss MC, Slaughter RE, et al. (1998) the revised Piper Fatigue Scale: psychometric evaluation in women with breast cancer. Oncol Nurs Forum 25(4): 677-684.
-
Piper BF, Borneman T, Chih-Yi VS, Koczywas M, Uman G, et al. (2008) Cancer-related fatigue: role of oncology nurses in translating National Comprehensive Cancer Network assessment guidelines into practice. Clin J Oncol Nurs 12(5): 37-47.
-
Hamilton M (1960) A rating scale for depression. J Neurol Neurosurg Psychiatry 23(1): 56-62.
-
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ, et al. (1989) The Pittsburgh sleep quality index: A new instrument for psychiatric practice and researc. Psychiatry Res 28(2): 193-213.
-
Craig CL, Marshall AL, Sjöström M, Bauman AE, Pratt M, et al. (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35(8): 1381-1395.
-
Collins LM, Schafer JL, Kam CM (2001) A comparison of inclusive and restrictive strategies in modern missing data procedures. Psychol Methods 6(4): 330-351.
-
Wesselink E, Koekkoek WAC, Grefte S, Witkamp RF, Zanten ARHV, et al. (2019) Feeding mitochondria: Potential role of nutritional components to improve critical illness convalescence. Clinical Nutrition 38(3): 982-995.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City