Cost-Utility of Venovenous Ecmo Associated with Protective Mechanical Ventilation in the Treatment of Patients with Acute Respiratory Distress Syndrome
Introduction: with the emergence of COVID-19 in the world, there was a race against time in the search for studies and scientific information that validated the most appropriate treatment. As a result, when caring for patients with the disease who developed ARDS and progressed to a severe condition with hospitalization in the ICU, the need for scientific evidence to guide care for these patients was even greater. Speculation about the effectiveness of using ECMO for these patients began to emerge, and with it, the need for scientific studies that would show the costs and benefits of acquiring this technology in the SUS. The dissertation that is intended to be defended is whether the use of VV ECMO associated with protective mechanical ventilation in patients with ARDS is more cost-effective compared to exclusive protective mechanical ventilation. General Objective: to analyze the cost-effectiveness of veno-venous ECMO in the treatment of patients with COVID-19 who evolve with severe Acute Respiratory Failure. Specific Objectives: review the scientific literature to summarize the best scientific evidence available on the safety and efficacy of using exclusive mechanical ventilation and venovenous ECMO in patients with acute respiratory failure, and estimate the costs associated with mechanical ventilation and the use of veno-venous ECMO. Method: Rapid systematic review for a complete health economic assessment based on a Markov model to estimate the incremental cost-effectiveness of using venovenous ECMO associated with protective mechanical ventilation in the treatment of patients with ARDS due to COVID-19. Results: Based on the estimated costs in each of the base case scenarios and the probabilities of the clinical effects resulting from the interventions, the study showed that the ECMO + protective IMV intervention offers around 0.295 AAQA compared to 0.2015 AAQA offered by the exclusive protective VMI. The incremental cost of ECMO + protective IMV is BRL 12,519.94 for 0.397 effectiveness compared to 0.215 exclusive protective IMV (incremental effectiveness of 0.182). For each qualityadjusted year of life gained, the amount of R$ 68,902.92 would have to be disbursed. Conclusion: the results showed that both veno-venous ECMO associated with protective mechanical ventilation and exclusive protective mechanical ventilation can be cost-effective alternatives for the treatment of patients with ARDS due to COVID-19 in the SUS, depending on the willingness to pay. However, in terms of effectiveness, ECMO was the most effective alternative, but with the highest cost increase.
Introduction
On December 31, 2019, the World Health Organization (OMS) was alerted to different cases of pneumonia in the city of Wuhan, People’s Republic of China. The reported cases were associated with a new strain of coronavirus not yet identified in humans, the SARS-CoV-2 that causes the disease COVID-19. A mass contamination began, which would soon turn into a Pandemic. On January 30, 2020, the WHO declared the outbreak a public health emergency of international concern, that is, an extraordinary event with great public health risk due to the international spread of diseases [1].
A race against time has begun for science to understand the mechanisms of the new virus, with regard to transmissibility, morbidity, pathophysiology, associated risk factors and mortality, in addition to the development and reviews of clinical protocols and therapeutic guidelines for the best possible assistance to hospitalized patients and for disease prevention. A daily work involving all members of the multidisciplinary team.
COVID-19 is an acute respiratory illness, which can progress to an acute respiratory distress syndrome (SDRA) [2]. Second Nishiura, et al. [3], the pathophysiological process of the disease results in destruction of the lung parenchyma, including extensive consolidation and interstitial inflammation, regardless of hypoxemia or respiratory distress, in addition to intravascular coagulopathy. Second Levi e Cate [4], intravascular coagulation is characterized by the diffuse activation of intravascular coagulation, leading to the formation and deposition of fibrin in the microvasculature.
We know that symptoms of COVID-19 can range from mild to severe. The latter are observed or can characterize ARDS, leading the patient to a severe clinical condition, with the need for hospitalization in Intensive Care Units (UTI), and not infrequently, mechanical ventilatory support, as an advanced life support measure, due to the acute respiratory failure that quickly sets in in those who develop the severe form of the disease. In the UTI, therefore, the patient will have the opportunity to be assisted by a specialized multidisciplinary team, increasing their chances of survival given the severity and lethality of the severe form of the disease. The SDRA caused by COVID-19 ends up leading the patient to a condition of Insufficiency Respiratória Aguda (IRA).
The IRA it is mainly characterized by the impairment of gas exchange caused by various clinical conditions, leading the patient to a potentially serious syndrome, so that it is necessary to hospitalize him in an intensive care unit [5]. It is always worth remembering that IRA is a consequence of a direct or indirect injury to the lung, such as SDRA caused by COVID-19.
Patients with Acute Respiratory Failure who require mechanical ventilation (VM) can benefit from UTI beds, which is undoubtedly the most appropriate place for hospitalization, especially due to the imminent need for mechanical ventilatory support, including invasive, due to the disease that impacts especially the respiratory function.
In 2019, before the Pandemic, the number of hospitalizations due to respiratory diseases in Brazil was 1.190.950, and 98.190 deaths [6]. However, in 2020, at the height of the pandemic, the number of hospitalizations was 760.929 and 92.828 deaths [7]. In 2021, the number of hospitalizations was 759.311 and 88.988 deaths [8].
With specific regard to hospitalizations of high complexity regardless of etiology, in 2019 in Brazil, 931.138 patients were admitted, and 27.944 deaths were recorded. In 2020, the numbers were 777.190 hospitalizations, and 26.638 deaths. Already in 2021, the numbers were 821.483 hospitalizations of high complexity and 28.356 deaths [6, 7, 8].
Although UTIs may have human and technological resources to provide advanced life support for patients who develop the severe form of the disease and have progressed to acute respiratory failure, specifically invasive mechanical ventilation (VMI), not all patients are able to benefit of this technology, requiring the need for other technological resources to ensure the survival of patients who do not respond clinically to VMI.
A study by Ranzani, et al. [9] analyzed the data of all patients aged 20 years or older, hospitalized due to COVID-19 in Brazil, in the period between 02/16/2020 and 08/15/2020, recorded in the Influenza Epidemiological Surveillance Information System (SIVEP-Gripe), totaling 254.288 individuals, which found a mortality in ICUs of 59% (47.002 / 79.687), and of the individuals who received mechanical ventilation, 80% (36.046 / 45.205) died.
Regarding the impacts of invasive mechanical ventilation on COVID-19 patients, the misuse of these resources can be considered as triggering lung injury or worsening the patient’s clinical condition, developing iatrogenic events such as barotrauma, as a result of flows, administration of large volumes and inadequate pressures during ventilatory support [10].
In this context, extracorporeal membrane oxygenation (ECMO) veno-venous (VV) has become indicated and used in some UTIs for patients with COVID-19 associated with refractory hypoxemic respiratory failure as an alternative to invasive mechanical ventilation (VMI) [11]. Although the scientific literature may suggest that the use of venovenous ECMO associated with protective VM results in some clinical benefit for patients with COVID-19 refractory to VMI [11], the costs of its use are high when compared to the costs of exclusive protective VM.
Faced with the uncertainties surrounding not only the clinical benefits of using veno-venous ECMO for these patients, but also the costs associated with its use, even though in theory this technology may be effective in reducing preventable deaths, improving the quality of life or reduction of disabilities caused by the severe form of the disease, the Ministry of Health (MS), through the National Commission for the Incorporation of Technologies in the SUS (CONITEC), based on Health Technology Assessment (ATS) studies, analyzes of cost-effectiveness and budgetary impact (CONITEC Recommendation Report nº. 636 of june 2021), evaluated the possibility of incorporating the technology, given the pressure exerted by stakeholders (term used in ATS studies to refer to interested people), including, the media, at a very troubled and critical moment of the pandemic, in which, the news that a famous Brazilian actor and comedian, with a serious condition of compromise the respiratory system due to the complications of COVID-19, was benefiting from a “new” technology that helped to maintain tissue oxygenation, helped to “popularize” the ECMO procedure and causing the Ministry of Health to take an official position regarding the possibility of incorporating and offering the procedure in the SUS.
The Scientific Technical Opinion (PTC) of the CONITEC Recommendation Report synthesized scientific evidence from six studies that evaluated the use of therapy with exclusive VMI and ECMO associated or not with ultra- protective mechanical ventilation. The meta-analysis showed a 33% gain in survival (RR=0,67; 95% IC: 0,57 to 0,79) for patients with Severe Acute Respiratory Syndrome (SRAG) or Severe Acute Respiratory Distress Syndrome (SARA) who received ECMO support in both the fixed and random effects models, but the odds of mortality were not significantly different between the two technologies (Estimate= 0,273; 95%CI: 0,06 to 1,111; I2= 0%, Q of Cochran, p value = 0,57) [12].
Among the six studies included in the systematic review to compose the set of evidence in the aforementioned CONITEC Report, two were published more than ten years ago, one in 1994 and the other in 2009 [13, 14]. Considering the possibility that new scientific evidence has been produced since the publication of this report, it should be considered reasonable and very timely to develop a new systematic review of the literature, in order to recover the most recent scientific evidence available about the clinical benefits of use of ECMO for patients with COVID, and that can be imputed in a mathematical model along the lines of a Markov model, for a new and more recent cost-effectiveness analysis, now at a more favorable moment due to the cooling of the pandemic, when it would be reasonable to believe that the costs related to the acquisition of equipment and inputs will probably be relatively lower.
Conitec members understood that despite the benefits of treatment, there is great difficulty in expanding and covering treatment for all patients who would eventually need therapy. The plenary also considered the moment of the pandemic as not favorable to the incorporation of ECMO, due to the existence of only nine centers belonging to the SUS registered in the Extracorporeal Life Support Organization (ELSO), being the majority in the Southeast region, which would lead to inequality of care, in addition to the impossibility of creating new centers at the time of the Pandemic [12].
ELSO is an international not-for-profit consortium that provides continuing education support, guidelines, original research, publications, and data recording of patients using ECMO to healthcare institutions, researchers, and industry partners.
With regard to economic aspects, the Report estimated that hospitalization costs with mechanical ventilation can reach R$ 78.750,34 to win 0,222±0,024 Quality-Adjusted Life Years (QALY) versus R$ 119.433,62 with ECMO to obtain 0,646±0,066 QALYs, resulting in the incremental difference of R$ 40.683,28/0,424±0,042 QALYs. In the incremental cost- effectiveness ratio, the Incremental Cost-Effectiveness Ratio (RCEI) was R$ 95.951,13 to obtain 1 year of life gained with quality (1 year of life without any disability) [12].
In terms of budgetary impact, the Report suggested that approximately 99% of critically ill patients with COVID-19 would respond clinically satisfactorily with conventional mechanical ventilation (VMI) and the remaining 1% would be refractory and require ECMO rescue therapy. Therefore, for Brazil, the Incremental Budgetary Impact with the ECMO intervention was estimated at R$ 15.703.746,08 in the 1st year and add R$ 80.816.036,09 with a 1% discount rate for the first five years [12].
Based on the scientific evidence presented in the PTC of the Report, the CONITEC Plenary decided that the matter should be made available in Public Consultation with a preliminary recommendation unfavorable to the incorporation of ECMO for the support of patients with severe acute respiratory syndrome due to viral infections, refractory to ventilation conventional mechanics within the SUS [12]. Later, a few months later, the CONITEC Plenary, in its 98th Ordinary Meeting, on June 10, 2021, decided by simple majority to recommend the non-incorporation of Extracorporeal Membrane Oxygenation (ECMO) as a therapy to support patients with respiratory failure severe and refractory in the SUS. To make this decision, the members of the Plenary of CONITEC considered that despite the benefits of the treatment, there is a great difficulty in expanding and covering the treatment for all the patients who might need the therapy, and that it would be unfeasible to create new centers in the country. current context.
The problem of this study is based on the premise that, with the expansion and consolidation of scientific knowledge about the disease, especially with regard to the clinical management of patients with the severe form of the disease and the advanced life support resources used, as well as the restructuring of the economic and industrial complex of health and the supply chain, significantly impacted at the height of the pandemic, contributing to a significant increase in the prices of inputs and medical-assistance equipment in the country and in the world, associated with the cooling of the pandemic in Brazil consequent reduction in demand, in a planned manner and outside a context of chaos in public health, CONITEC’s recommendation could be reconsidered, if new evidence, in view of the current context in which the pandemic is found, in Brazil and in the world, suggest that the use of veno-venous ECMO is cost-effective.
Given the above, the research question is whether the use of ECMO associated with protective mechanical ventilation in adult patients aged 18 years and over with SDRA is cost- effective as a therapeutic intervention to reduce mortality compared to exclusive protective mechanical ventilation.
Method
This is a Health Technology Assessment (HTA) study that can be defined as a process of analysis of the clinical, economic and social consequences of the use of health technologies. To compose the set of scientific evidence about the safety and efficacy of the interventions analyzed in this study, those already produced and presented in CONITEC Report nº 636 of June 2021 were considered, complemented by studies retrieved from a rapid systematic review carried out in October 2021, which consulted Medline databases, via PubMed, Embase, via Rede Cafe and Cochrane, which included randomized studies or with structured case-control pairing, prospective and even retrospective cohorts, in addition to systematic reviews with or without meta-analysis, including network meta-analyses.
Search strategies were guided by the following question structured by the acronym PICOS (population, intervention, comparator, outcome – outcome and type of studies – study):
Population
Adult patients aged 18 years and older with SDRA due to COVID-19, refractory to exclusive protective mechanical ventilation.
Intervention
Extracorporeal membrane oxygenation (ECMO) associated with protective mechanical ventilation.
Comparator
Exclusive protective mechanical ventilation.
Outcomes
Mortality and sepsis. MeSH and Emtree controlled terms used for the search strategies are shown in Table 1.
Search strategies were designed to be sensitive and specific enough to retrieve the largest possible number of documents that answer the research question. In this sense, in addition to limitations related to the type of study and age of individuals (≥ 18 years old), searches were limited to studies in English, Portuguese and Spanish, available in full texts, published in the last 10 years. The comparator and the outcomes were not considered in the strategies in order to make them more sensitive. The Medline search considered the PubMed Clinical Queries filter “treatment” to refine the search.
In Cochrane, the search was performed using the PICOs Beta resource, considering only the population (MeSH COVID-19) and the intervention (MeSH Extracorporeal Membrane Oxygenation), which were combined by the Boolean AND operator.
The controlled terms used in the search strategies in Medline, Embase and Cochrane are presented in Table 1. The search strategies by consulted base are presented in Table 2.
| MeSH | Emtree | |
|---|---|---|
| População | COVID-19 OR COVID 19 OR COVID-19 Virus Disease OR COVID 19 Virus Disease OR COVID-19 Virus Diseases OR Disease, COVID-19 Virus OR Virus Disease, COVID-19 OR COVID-19 Virus Infection OR COVID 19 Virus Infection OR COVID-19 Virus Infections OR Infection, COVID-19 Virus OR Virus Infection, COVID-19 OR 2019-nCoV Infection OR 2019 nCoV Infection OR 2019-nCoV Infections OR Infection, 2019-nCoV OR Coronavirus Disease-19 OR Coronavirus Disease 19 OR 2019 Novel Coronavirus Disease OR 2019 Novel Coronavirus Infection OR 2019-nCoV Disease OR 2019 nCoV Disease OR 2019-nCoV Diseases OR Disease, 2019-nCoV OR COVID19 OR Coronavirus Disease 2019 OR Disease 2019, Coronavirus OR SARS Coronavirus 2 Infection OR SARS-CoV-2 Infection OR Infection, SARS-CoV-2 OR SARS CoV 2 Infection OR SARS- CoV-2 Infections OR COVID-19 Pandemic OR COVID 19 Pandemic OR COVID-19 Pandemics OR Pandemic, COVID-19 | coronavirus disease 2019 OR 2019 novel coronavirus disease OR 2019 novel coronavirus epidemic OR 2019 novel coronavirus infection OR 2019-nCoV disease OR 2019-nCoV infection OR coronavirus disease 2 OR coronavirus disease 2010 OR coronavirus disease 2019 pneumonia OR coronavirus disease-19 OR coronavirus infection 2019 OR COVID OR COVID 19 OR COVID 19 induced pneumonia OR COVID 2019 OR COVID-10 OR COVID-19 OR COVID-19 induced pneumonia OR COVID-19 pneumonia OR COVID19 OR nCoV 2019 disease OR nCoV 2019 infection OR new coronavirus pneumonia OR novel coronavirus 2019 disease OR novel coronavirus 2019 infection OR novel coronavirus disease 2019 OR novel coronavirus infected pneumonia OR novel coronavirus infection 2019 OR novel coronavirus pneumonia OR paucisymptomatic coronavirus disease 2019 OR SARS coronavirus 2 infection OR SARS coronavirus 2 pneumonia OR SARS- CoV-2 disease OR SARS-CoV-2 infection OR SARS-CoV-2 pneumonia OR SARS-CoV2 disease OR SARS-CoV2 infection OR SARSCoV2 disease OR SARSCoV2 infection OR severe acute respiratory syndrome 2 OR severe acute respiratory syndrome 2 pneumonia OR severe acute respiratory syndrome coronavirus 2 infection OR severe acute respiratory syndrome coronavirus 2019 infection OR severe acute respiratory syndrome CoV-2 infection OR Wuhan coronavirus disease OR Wuhan coronavirus infection |
| Intervenção | Extracorporeal Membrane Oxygenation OR Extracorporeal Membrane Oxygenations OR Membrane Oxygenation, Extracorporeal OR Oxygenation, Extracorporeal Membrane OR ECMO Treatment OR ECMO Treatments OR Treatment, ECMO OR ECLS Treatment OR ECLS Treatments OR Treatment, ECLS OR ECMO Extracorporeal Membrane Oxygenation OR Extracorporeal Life Support OR Extracorporeal Life Supports OR Life Support, Extracorporeal OR Venoarterial ECMO OR ECMO, Venoarterial OR Venoarterial ECMOs OR Venoarterial Extracorporeal Membrane Oxygenation OR Venovenous ECMO OR ECMO, Venovenous OR Venovenous ECMOs OR Venovenous Extracorporeal Membrane Oxygenation | extracorporeal membrane oxygenation device OR CardioHelp OR extracorporeal membrane oxygenation circuit OR extracorporeal membrane oxygenator OR Minimax (extracorporeal membrane oxygenation device) OR Minimax Plus OR Primo2x OR Prolung (device) OR Quadrox PLS Oxygenator OR Rotaflow RF 32 OR veno- venous ECMO OR veno venous extracorporeal life support OR veno venous extracorporeal membrane oxygenation OR veno venous extracorporeal oxygenation OR venovenous ECMO OR venovenous extracorporeal life support OR venovenous extracorporeal membrane oxygenation OR venovenous extracorporeal oxygenation OR VV-ECLS OR VV-ECMO OR vvECLS OR vvECMO |
Table 1: Controlled terms used in Medline, Embase, and Cochrane search strategies. Rio de Janeiro, Brazil - 2021.
MedLine/Pubmed Cochrane Embase/Rede Cafe
(((((COVID-19 OR COVID 19 OR COVID-19 Virus Disease OR COVID 19 Virus Disease OR COVID-19 Virus Diseases OR Disease, COVID-19 Virus OR Virus Disease, COVID-19 OR COVID-19 Virus Infection OR COVID 19 Virus Infection OR COVID-19 Virus Infections OR Infection, COVID-19 Virus OR Virus Infection, COVID-19 OR 2019-nCoV Infection OR 2019 nCoV Infection OR 2019-nCoV Infections OR Infection, 2019-nCoV OR Coronavirus Disease-19 OR Coronavirus Disease 19 OR 2019 Novel Coronavirus Disease OR 2019 Novel Coronavirus Infection OR 2019-nCoV Disease OR 2019 nCoV Disease OR 2019-nCoV Diseases OR Disease, 2019-nCoV OR COVID19 OR Coronavirus Disease 2019 OR Disease 2019, Coronavirus OR SARS Coronavirus 2 Infection OR SARS-CoV-2 Infection OR Infection, SARS-CoV-2 OR SARS CoV 2 Infection OR SARS-CoV-2 Infections OR COVID-19 Pandemic OR COVID 19 Pandemic OR COVID-19 Pandemics OR Pandemic, COVID-19) and (Extracorporeal Membrane Oxygenation OR Extracorporeal Membrane Oxygenations OR Membrane Oxygenation, Extracorporeal OR Oxygenation, Extracorporeal Membrane OR ECMO Treatment OR ECMO Treatments OR Treatment, ECMO OR ECLS Treatment OR ECLS Treatments OR Treatment, ECLS OR ECMO Extracorporeal Membrane Oxygenation OR Extracorporeal Life Support OR Extracorporeal Life Supports OR Life Support, Extracorporeal OR Venoarterial ECMO OR ECMO, Venoarterial OR Venoarterial ECMOs OR Venoarterial Extracorporeal Membrane Oxygenation OR Venovenous ECMO OR ECMO, Venovenous OR Venovenous ECMOs OR Venovenous Extracorporeal Membrane Oxygenation)) AND ((y_10[Filter]) AND (clinicalstudy[Filter] OR clinicaltrial[Filter] OR meta- analysis[Filter] OR observationalstudy[Filter] OR randomiz edcontrolledtrial[Filter] OR systematicreview[Filter]) AND (fft[Filter]) AND (humans[Filter]) AND (alladult[Filter])))) AND (Therapy/Broad[filter])) AND (Therapy/Broad[filter])
- Covid-19 AND
- Extra corporeal
- Membrane
- Oxygenation
Table 2: Base search strategies.
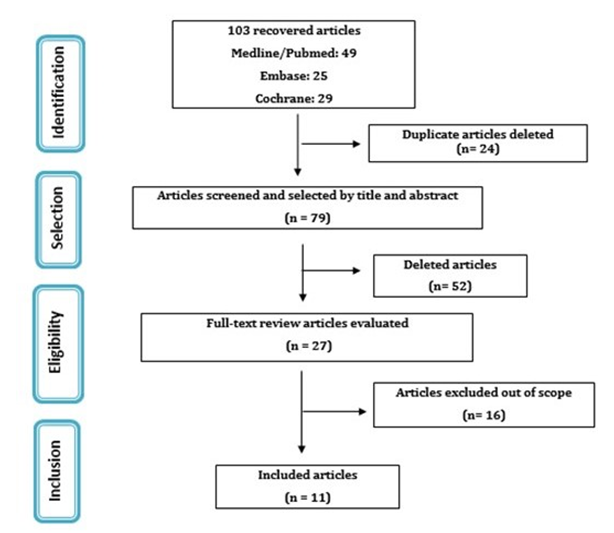
The searches returned a total of 103 documents, 49 of which were retrieved from Medline, 25 from Embase and 29 from Cochrane. The outcome of interest was mortality and SEPSE. The articles were read and evaluated by the research author himself with regard to the eligibility criteria, for inclusion or not of the studies, in two stages: in the first, (((((((((((((((((((((((((((((((((((((((((coronavirus AND disease AND 2019 OR 2019) AND novel AND coronavirus AND disease OR 2019) AND novel AND coronavirus AND epidemic OR 2019) AND novel AND coronavirus AND infection OR ‘2019 ncov’) AND disease OR ‘2019 ncov’) AND infection OR coronavirus) AND disease AND 2 OR coronavirus) AND disease AND 2010 OR coronavirus) AND disease AND 2019 AND pneumonia OR coronavirus) AND ‘disease 19’ OR coronavirus) AND infection AND 2019 OR covid) AND 19 OR covid) AND 19 AND induced AND pneumonia OR covid) AND 2019 OR ‘covid 10’ OR ‘covid 19’) AND induced AND pneumonia OR ‘covid 19’) AND pneumonia OR covid19 OR ncov) AND 2019 AND disease OR ncov) AND 2019 AND infection OR new) AND coronavirus AND pneumonia OR novel) AND coronavirus AND 2019 AND disease OR novel) AND coronavirus AND 2019 AND infection OR novel) AND coronavirus AND disease AND 2019 OR novel) AND coronavirus AND infected AND pneumonia OR novel) AND coronavirus AND infection AND 2019 OR novel) AND coronavirus AND pneumonia OR paucisymptomatic) AND coronavirus AND disease AND 2019 OR sars) AND coronavirus AND 2 AND infection OR sars) AND coronavirus AND 2 AND pneumonia OR ‘sars cov 2’) AND disease OR ‘sars cov 2’) AND infection OR ‘sars cov 2’) AND pneumonia OR ‘sars cov2’) AND disease OR ‘sars cov2’) AND infection OR sarscov2) AND disease OR sarscov2) AND infection OR severe) AND acute AND respiratory AND syndrome AND 2 OR severe) AND acute AND respiratory AND syndrome AND 2 AND pneumonia OR severe) AND acute AND respiratory AND syndrome AND coronavirus AND 2 AND infection OR severe) AND acute AND respiratory AND syndrome AND coronavirus AND 2019 AND infection OR severe) AND acute AND respiratory AND syndrome AND ‘cov 2’ AND infection OR wuhan) AND coronavirus AND disease OR wuhan) AND coronavirus AND infection AND ((((((((((((((((extracorporeal AND membrane AND oxygenation AND device OR cardiohelp OR extracorporeal) AND membrane AND oxygenation AND circuit OR extracorporeal) AND membrane AND oxygenator OR minimax) AND extracorporeal AND membrane AND oxygenation AND device OR minimax) AND plus OR primo2x OR prolung) AND device OR quadrox) AND pls AND oxygenator OR rotaflow) AND rf AND 32 OR ‘veno venous’) AND ecmo OR veno) AND venous AND extracorporeal AND life AND support OR veno) AND venous AND extracorporeal AND membrane AND oxygenation OR veno) AND venous AND extracorporeal AND oxygenation OR venovenous) AND ecmo OR venovenous) AND extracorporeal AND life AND support OR venovenous) AND extracorporeal AND membrane AND oxygenation OR venovenous) AND extracorporeal AND oxygenation OR ‘vv ecls’ OR ‘vv ecmo’ OR vvecls OR vvecmo) AND (2020:py OR 2021:py) AND (‘clinical article’/de OR ‘clinical trial’/ de OR ‘cohort analysis’/de OR ‘comparative study’/de OR ‘controlled study’/de OR ‘evidence based medicine’/de OR ‘human’/de OR ‘major clinical study’/de OR ‘multicenter study’/de OR ‘observational study’/de OR ‘prospective study’/ de OR ‘retrospective study’/de OR ‘systematic review’/de) AND (‘article’/it OR ‘article in press’/it OR ‘review’/it) only the title and abstract were read and in the second, the included studies were read in Complete text. In the end, 15 articles were included for the synthesis of evidence. The Prisma flowchart, describing the information retrieval process, from identification to inclusion of studies, is shown in Figure 1.
| Ref. | Study/Design/ Origin | Study/Design / OriginPopulation/ Duration of the study | Intervention and Comparator | Outcomes | Main results |
|---|---|---|---|---|---|
| 1 | Ramanathan, et al. Inglaterra Systematic review with meta- analysis | Adult patients with COVID-19 who develop SDRA while using ECMO. Two-year follow- up. | ECMO in adults with SDRA from COVID-19 | Primary: Hospital mortality. Secondary: duration of ECMO therapy and mechanical ventilation, ECMO weaning rate, and complications during ECMO. | The rate of patients who died on VV ECMO was 35.7% (95% CI 30.7–40.7%, high certainty). |
| 2 | Serafim, et al. BrasilSystematic review without meta-analysis | Patients with COVID-19 admitted to the UTI. The bibliographic search was carried out from December 1, 2019 to August 20, 2020. | None. | Incidence of SDRA, need for VM and TSR, use of vasopressors, death in the ICU/hospital and length of stay in the hospital/UTI. | In VMI, 59% evolved to death. On ECMO, 90%. |
| 3 | Domecq, et al. [15] Cross-sectional observational study | In VMI, 59% evolved to death. On ECMO, 90%. Patients with COVID-19 who did and did not need various types and combinations of organ support (VM, TSR, vasopressors, and ECMO). Follow-up at 9 months. | None. | The primary outcome was in-hospital mortality. Secondary outcomes were hospital discharge with or without assistance and length of hospital stay. | Mortality was 40.8% among patients receiving IMV alone. Mortality was 39% for patients receiving ECMO. |
| 4 | Giraud, et al. SuíçaRetrospective observational study | Adult patients with severe ARDS related to COVID-19 pneumonia admitted to the UTI supported by VV ECMO. 2-month follow-up. | None. | Indication of RRT, parameters and duration of ECMO support, length of stay in the ICU and length of hospital stay. | 60% mortality rate for VMI. The study failed to demonstrate a difference in 60- day mortality of 20% and failed to show a significant improvement in mortality (35% vs. 46%; relative risk [RR] 0.76; 95% confidence interval [CI] 0 .55–1.04, p = 0.09). |
| 5 | Yu, et al. China Prospective observational study | Adult patients with COVID-19 admitted to the UTI. 24 hour tracking. | None. | Outcomes and complications of patients with COVID-19 and the intensity of treatments these patients received. | SDRA occurred in 71.2% of patients, 37.6% received IMV, and 6.2% were treated with ECMO at the same time. Mortality for VMI was 38.5%. Septic shock occurred in 15%. |
| 6 | Stop, et al. Alemanha Retrospective observational study | Patients with COVID-19 who have developed ARDS requiring ECMO. 1 month follow-up. | ECMO | thromboembolism | 53% were successfully weaned from ECMO and discharged from hospital and 47% died. |
| 7 | Alhumaid, et al. Arábia Saudita Prospective observational study | Adult patients with SARS-CoV-2 admitted to the ICU. 6-month follow-up. | ECMO | Effect of ECMO rescue therapy | SDRA occurred in 86.5%. All patients in the ECMO group were intubated and placed on mechanical ventilation compared with 52% in the non-ECMO group (p = 0.005). In the ECMO group, VV mode was 93.5%, and 48.9% died. In the ECMO group, 55.4% were discharged, 48.9% died. Septic shock in 19.6% and multiple organ failure in 10.9%. |
| 8 | Yang, et al. Canadá Retrospective cohort study | Adult patients with COVID-19 pneumonia admitted to the UTI. 5-month follow-up. | None. | Characteristics, outcomes and management of critically ill patients with COVID-19 pneumonia. | 61.3% entered VMI. No patient required ECMO. UTI mortality in patients requiring mechanical ventilation was 18.5%. |
| 9 | Lebreton, et al. França Retrospective cohort study | Adult patients with severe ARDS due to COVID-19 requiring ECMO admitted to the UTI. 3-month follow-up. | ECMO | UTI and ECMO-related complications, ECMO duration and ICU stay, 90- day survival status after starting ECMO, and causes of death. | 95% underwent ECMO VV, where 96% survived and 95% died (p value 0.44). In 16% there was septic shock and all died (29%). Multiple organ failure was 18% and all died (32%) |
| 10 | Yang, et al. China Retrospective cohort study | Adult patients infected with SARS-CoV-2 who were treated with ECMO. 3-month follow- up. | ECMO | ECMO duration, complications and state of life. | ECMO VV was the configuration initiated in all patients. During the study period, of the 73 patients, 59 died, 14 survived, and 7 (9.6%) patients were discharged from the hospital. |
| 11 | Biancari, et al. França, Alemanha, Itália, Suécia e Reino Unido Retrospective cohort study | Adult patients with confirmed COVID- 19-related SDRA undergoing ECMO in any setting. 6-month follow-up. | ECMO VV or VA. | All-cause mortality within six months of starting ECMO therapy, ECMO mortality, UTI mortality, hospital mortality, pulmonary or pleural complications requiring thoracic surgery, stroke, AVC, LRA, TSR,ttransfusion of blood products, bloodstream infection , confirmed or suspected pulmonary embolism, duration of invasive surgery, mechanical ventilation, and length of stay in the UTI and hospital. | ECMO VV was used in 92.4% of patients. Of these, 96.8% survived and 88.6% died in the 1st execution, 6.5% survived and 2.9% died in the 2nd execution, and 1.4% died in the 3rd execution. Bloodstream infection was 31.8% |
Table 3: Characteristics and main results of the studies selected in the review.
The Proposed Analytical Model
The proposal is a dynamic analytical model, based on a Markov model. The first state of health of patients with COVID-19 was defined as “ARDS”, indicating that the patient has a complication associated with the disease, and that, therefore, he is experiencing its consequences and, therefore, has a higher risk of death than a subject without the disease and its complications.
Assumptions Assumed in the Model
- The following assumptions were assumed in the Model: SEPSIS was the only possible complication;
- After discharge, the patients were no longer followed up and, therefore, this state of health was also considered as an absorber;
- The Markovian cycles last 30 days (time horizon of 2 months with two cycles).
The Structure of the Model
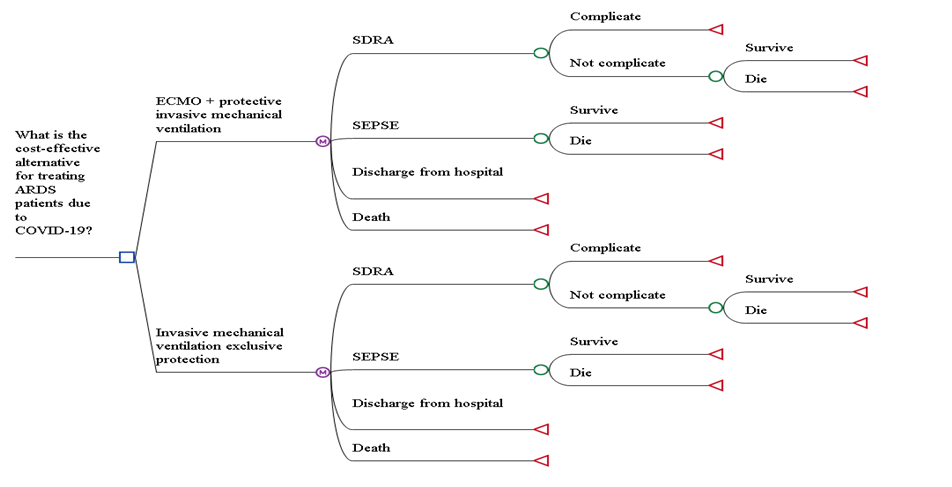
Patients enter the Markov model (Figure 2) after being diagnosed with severe acute respiratory failure and are submitted either to invasive mechanical ventilation alone or associated with ECMO. Starting from the “ARDS” disease state, the patient can transition to the “SEPSE”, “discharge” or “death” state. From the “SEPSE” state it may progress to the “discharge” or “death” states.
As the disease progresses, the patient begins to experience his deficient health condition with an increased risk of death caused by the direct result of the disease or its complications over all other causes of mortality. Below, in Figure 2, we have the proposed analytical model.
All possible transitions for this analysis are represented in the model by the transition diagram below (Figure 3).
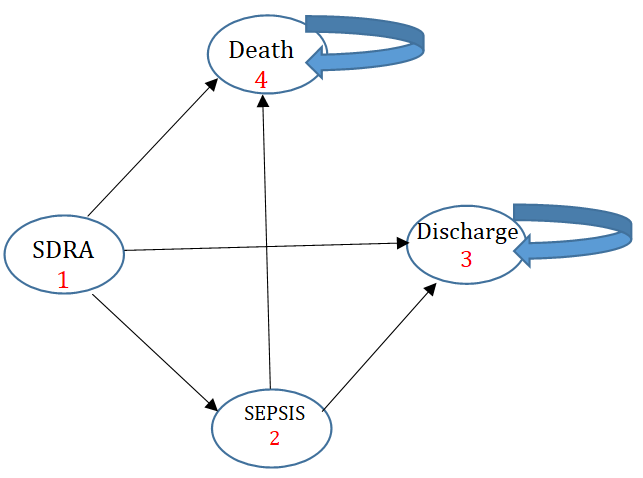
Figure 3: Transition diagram proposed for the analytical Markov model. Source: The author, 2023 Variables related to the probability of dying from sepsis or ARDS were imputed in the Markov model, in addition to costs related to the technologies, both in the ECMO+protective MV scenario and in the exclusive protective MV scenario, as shown in Table 3 below.
| Description | Average | Minimum | Maximum | Reference | |
|---|---|---|---|---|---|
| Custo_SEPSE | Total cost of sepsis treatment | 40873,7 | 28611,59 | 53135,81 | Conde, et al. [16] |
| Custo_VMeECMO | Cost of ECMO + Mechanical ventilation | 146,998,415 | 131448,48 | 162508,35 | IC HCFMUSP; HCPA UFRGS, |
| Custo_VMExc | Cost of ECMO + mechanical ventilationCosts with the use of exclusive mechanical ventilation | 121372,24 | 105526,05 | 137218,43 | IC HCFMUSP; HCPA UFRGS, |
| P_M_ECMO | Likelihood of dying on ECMO | 0,35 | 0,245 | 0,455 | DOMECQ |
| P_M_VM | Probability of dying in VM | 0,408 | 0,2856 | 0,5304 | DOMECQ |
| P_S_ECMO | Probability to survive in ECMO | 0,412 | 0,2884 | 0,5356 | DOMECQ |
| P_S_VM | Probability of surviving on mechanical ventilation | 0,298 | 0,2086 | 0,3874 | DOMECQ |
| P_SEPSE_ECMO | Likelihood of having sepsis on ECMO | 0,448 | 0,3136 | 0,5824 | ALLYN [17] |
| P_SEPSE_ECMO_M | Likelihood of getting sepsis on ECMO and dying | 0,262 | 0,1834 | 0,3406 | ALLYN [17] |
| P_SEPSE_ECMO_S | Probability of making sepsis on ECMO survive | 0,186 | 0,1302 | 0,2418 | ALLYN [17] |
| P_SEPSE_VM | Likelihood of sepsis on mechanical ventilation | 0,82165 | 0,6433 | 1 | COSTA |
| P_SEPSE_VM_M | Probability of developing sepsis on mechanical ventilation and dying | 0,5 | 0,35 | 0,65 | COSTA |
| U_COVID_ALTA | Post discharge COVID utility | 0,663 | 0 | 0,663 | Relatório Conitec nº 636 |
Table 4: Incremental cost effectiveness table. Source: The author, 2023
Results
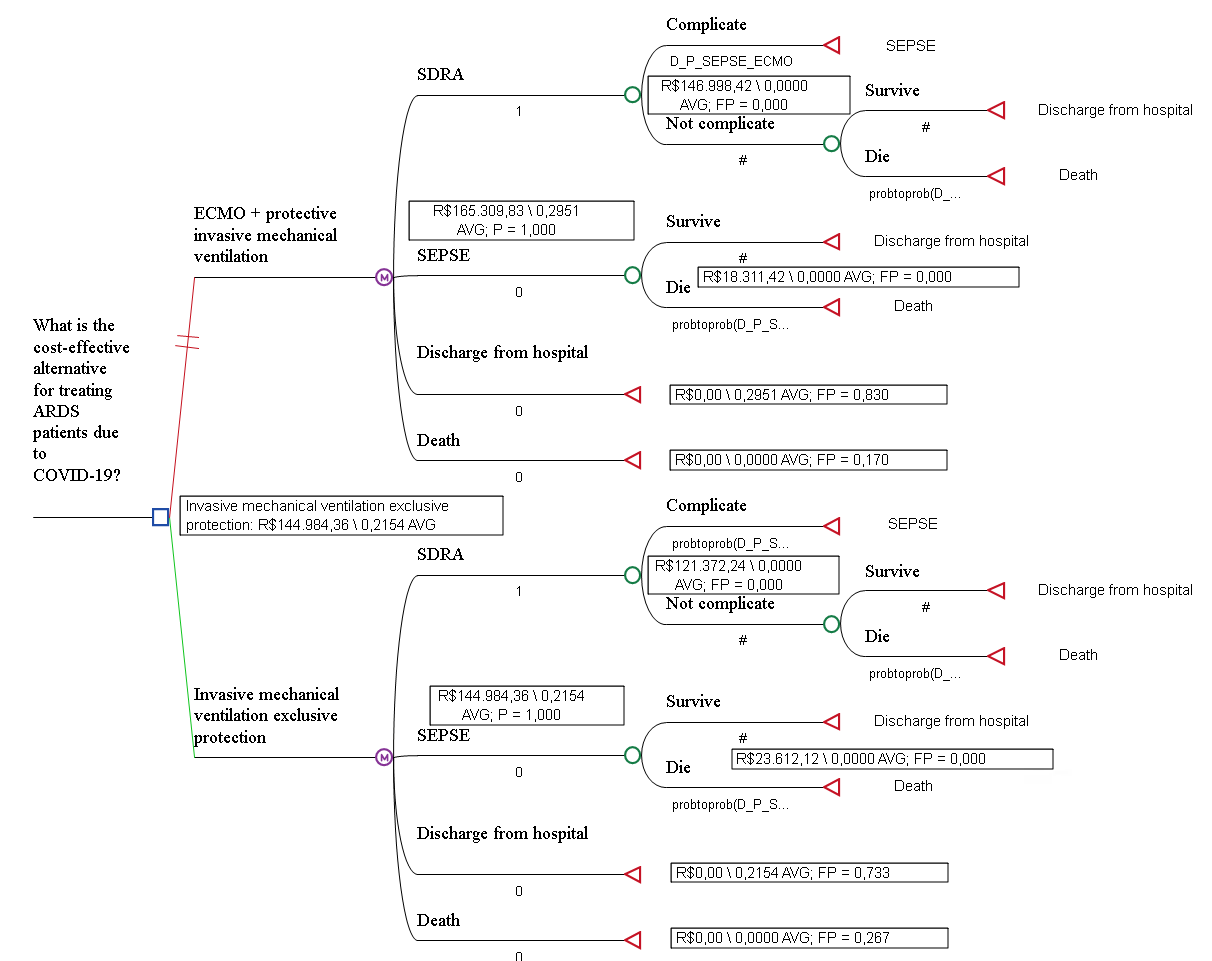
The proposed analytical model suggests that, in one year, exclusive invasive mechanical ventilation may represent a lower cost (R$ 144.984,36) although it may result in less effectiveness (0,215 QALY) when compared to ECMO + invasive mechanical ventilation, which, although it may represent higher cost, may also represent greater effectiveness (0,295 QALY), as suggested by the analytical model after Roll Back (Figure 4).
The cost-utility analysis chart (Figure 5), considering the willingness-to-pay threshold of R$ 120.000,00, shows that the ECMO intervention + protective VMI can offer around 0,295 AVAQ compared to 0,2015 AVAQ offered by the exclusive protective VMI.
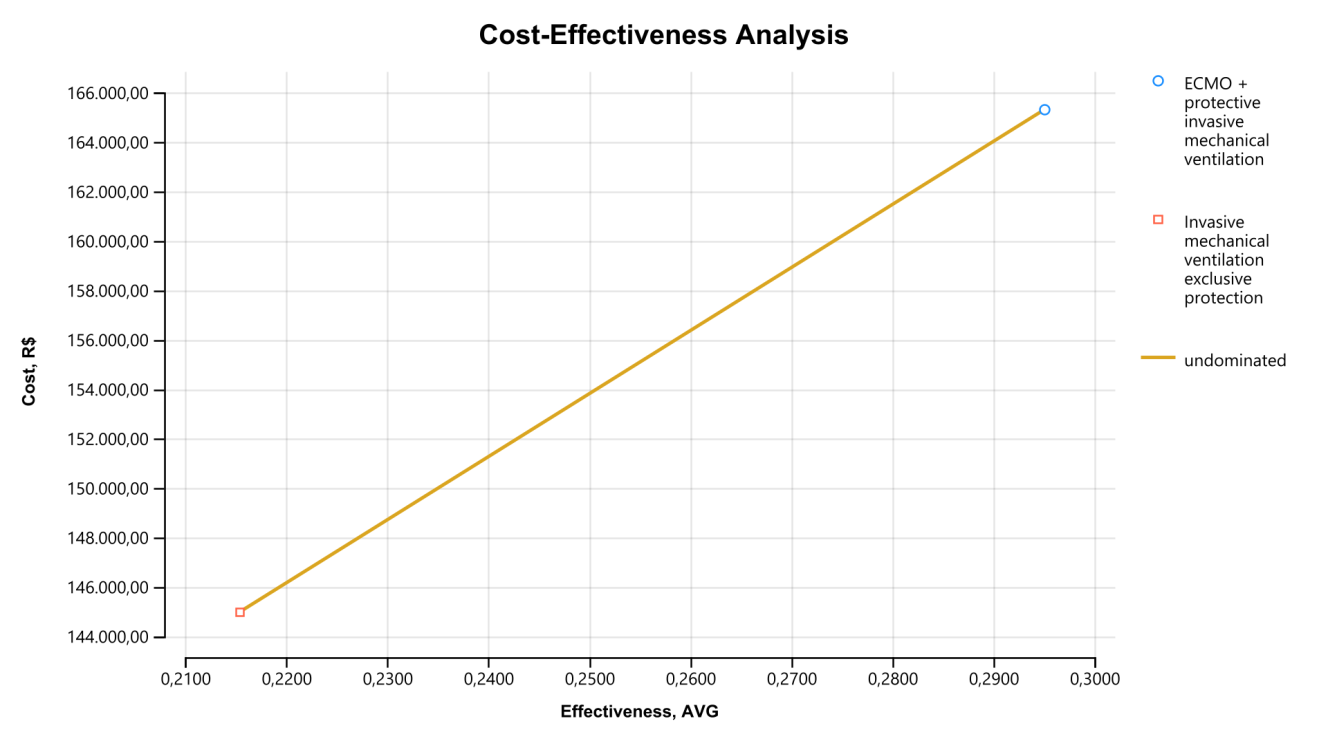
The incremental cost of ECMO + protective VMI is R$ 12.519.94 for 0,397 effectiveness compared to 0,215 exclusive protective VMI (incremental effectiveness of 0,182).
For each quality-adjusted year of life gained, the amount of R$ 68.902,92 (ICER) would have to be disbursed, as shown in Table 4 below.
| Cost | Cost Incr | Efe | Efe Incr | RCEI | NMB | |
|---|---|---|---|---|---|---|
| Exclusive Protective VMI | R$ 144.984,36 | 0,215 | -R$ 144.984,36 | |||
| ECMO + VMI Protective | R$ 157.504,30 | R$ 12.519,94 | 0,397 | 0,182 | R$ 68.902,92 | -R$ 157.504,30 |
Table 5: Incremental cost effectiveness table. Source: The author, 2023
Multivariate Deterministic Sensitivity Analysis
In the proposed analytical model, the robustness was evaluated from multivariate deterministic sensitivity analyses. A Tornado graph has been plotted. The willingness to pay threshold (LDP) was considered to be the value of R$ 120.000,00. The distribution of parameters for each variable is shown in Table 5 below.
| Description | Average | Smaller | Bigger | |
|---|---|---|---|---|
| Custo_SEPSE | Total cost of sepsis treatment | 40873,7 | 28611,59 | 53135,81 |
| Custo_VMeECMO | Cost of ECMO + Mechanical ventilation | 146,998,415 | 131448,48 | 162508,35 |
| Custo_VMExc | Cost of ECMO + mechanical ventilation Costs with the use of exclusive mechanical ventilation | 121372,24 | 105526,05 | 137218,43 |
| P_M_ECMO | Likelihood of dying on ECMO | 0,35 | 0,245 | 0,455 |
| P_M_VM | Probability of dying in VM | 0,408 | 0,2856 | 0,5304 |
| P_S_ECMO | Probability to survive in ECMO | 0,412 | 0,2884 | 0,5356 |
| P_S_VM | Probability of surviving on mechanical ventilation | 0,298 | 0,2086 | 0,3874 |
| P_SEPSE_ECMO | Likelihood of having sepsis on ECMO | 0,448 | 0,3136 | 0,5824 |
| P_SEPSE_ECMO_M | Likelihood of getting sepsis on ECMO and dying | 0,262 | 0,1834 | 0,3406 |
| P_SEPSE_ECMO_S | Probability of making sepsis on ECMO survive | 0,186 | 0,1302 | 0,2418 |
| P_SEPSE_VM | Likelihood of sepsis on mechanical ventilation | 0,82165 | 0,6433 | 1 |
| P_SEPSE_VM_M | Probability of developing sepsis on mechanical ventilation and dying | 0,5 | 0,35 | 0,65 |
| U_COVID_ALTA | Post discharge COVID utility | 0,663 | 0 | 0,663 |
Table 6: Distribution of parameters. Source: The author, 2023
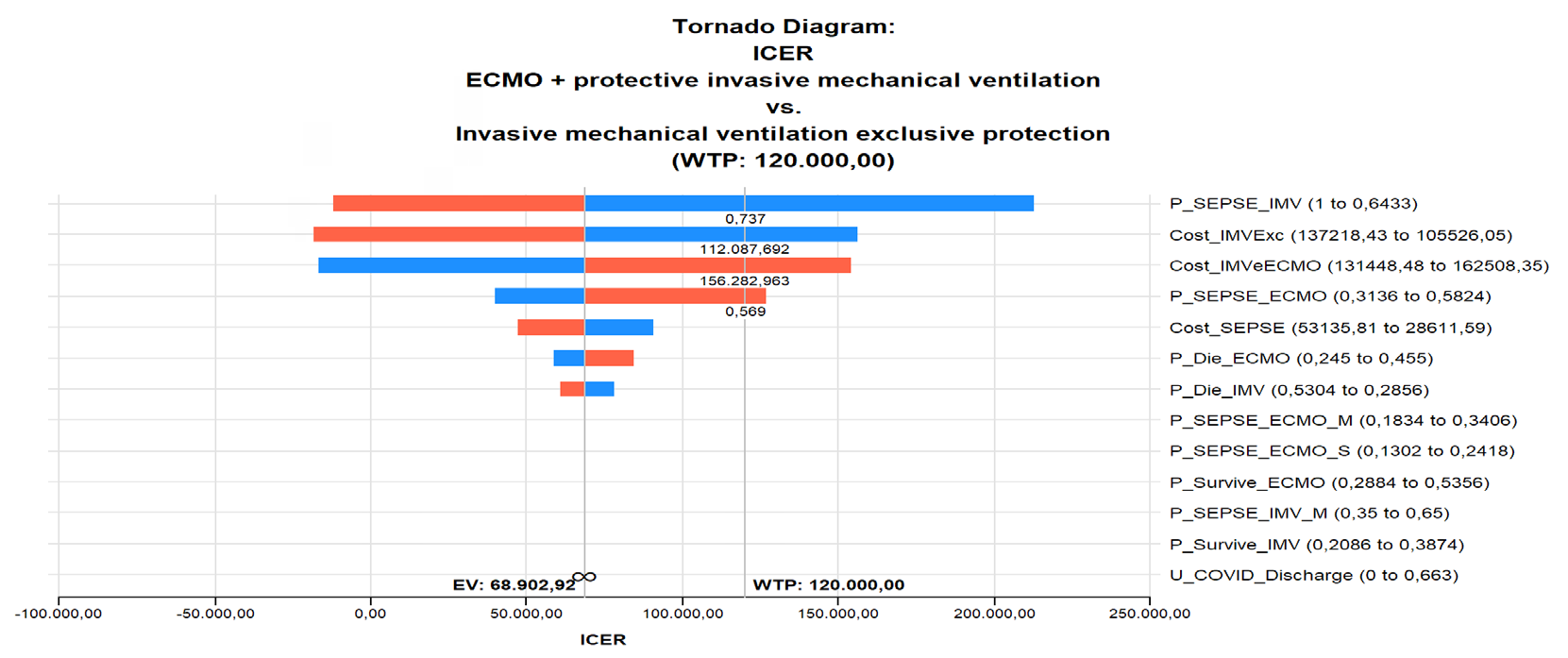
In the following Tornado diagram (Figure 6) we can see that when a value of R$ 120.000,00 of willingness to pay is defined, even so, four variables cross the line that represents this threshold. The lower the likelihood of sepsis on MV, the higher the ICER (RCEI) and therefore the less cost-effective ECMO. The same goes for the cost of the VM. The lower, the higher the ICER and therefore the less cost-effective ECMO.
On the contrary, it is observed in the Tornado diagram that the higher the cost of ECMO, the higher the ICER and, once again, the less cost-effective it will be. The same occurs in relation to the probability of having sepsis on ECMO. The cost of ECMO + IMV increases, as does the probability of sepsis on ECMO. That is, the result is unfavorable for ECMO.
Probabilistic Sensitivity Analysis
The probabilistic sensitivity analysis (PSA) was performed through 10.000 Monte Carlo simulations, in order to probabilistically analyze the impacts of the variation of the model parameters on the ICER results. The distributions assigned to the variables are shown in Table 6 below.
| Description | Parameter 1 | Parameter 2 | |
|---|---|---|---|
| Gama | Cost distribution with SEPSE | ((40873,7)^2)/((17341,24)^2) | (40873,7)/((17341,24)^2) |
| Gama | VM-ECMO cost distribution | ((146998,415)^2)/((21934,36)^2) | (146998,415)/((21934,36)^2) |
| Gama | Exclusive VM cost distribution | ((121372,24)^2)/((22409,9)^2) | (121372,24)/((22409,9)^2) |
| Beta | Probability distribution of dying on ECMO | (((0,35)^2)*(1-(0,35))/((0,148492)^2)-(0,35)) | ((1-(0,35))*((1-(0,35))*(0,35))/((0,148492)^2)-1)) |
| Beta | Probability distribution of surviving on ECMO | (((0,412)^2)*(1-(0,412))/((0,174797)^2)-(0,412)) | ((1-(0,412))*((1-(0,412))*(0,412))/((0,174797)^2)-1)) |
| Beta | Probability distribution of having sepsis on ECMO | (((0,448)^2)*(1-(0,448))/((0,19007)^2)-(0,448)) | ((1-(0,448))*((1-(0,448))*(0,448))/((0,19007)^2)-1)) |
| Beta | Probability distribution of having sepsis on ECMO and dying | (((0,262)^2)*(1-(0,262))/((0,111157)^2)-(0,262)) | ((1-(0,262))*((1-(0,262))*(0,262))/((0,111157)^2)-1)) |
| Beta | Probability distribution of having sepsis on ECMO and surviving | (((0,186)^2)*(1-(0,186))/((0,078913)^2)-(0,186)) | ((1-(0,186))*((1-(0,186))*(0,186))/((0,078913)^2)-1)) |
| Beta | Probability distribution of having sepsis on mechanical ventilation | (((0,82165)^2)*(1-(0,82165))/((0,25)^2)-(0,82165)) | ((1-(0,82165))*((1-(0,82165))*(0,82165))/((0,25)^2)-1)) |
| Beta | Probability distribution of having sepsis on mechanical ventilation and dying | (((0,5)^2)*(1-(0,5))/((0,212132)^2)-(0,5)) | ((1-(0,5))*((1-(0,5))*(0,5))/((0,212132)^2)-1)) |
| Beta | Probability distribution of surviving on mechanical ventilation | (((0,298)^2)*(1-(0,298))/((0,126431)^2)-(0,298)) | ((1-(0,298))*((1-(0,298))*(0,298))/((0,126431)^2)-1)) |
| Beta | Probability distribution of dying on mechanical ventilation | (((0,408)^2)*(1-(0,408))/((0,1731)^2)-(0,408)) | ((1-(0,408))*((1-(0,408))*(0,408))/((0,1731)^2)-1)) |
| Normal | Utility distribution in post-discharge COVID | 0,663 | 0,192333 |
Table 7: Distribution, values and parameters. The author (2023). Nota: Distribuição Gama: parâmetro 1= alfa e 2= lambda ; Distrib
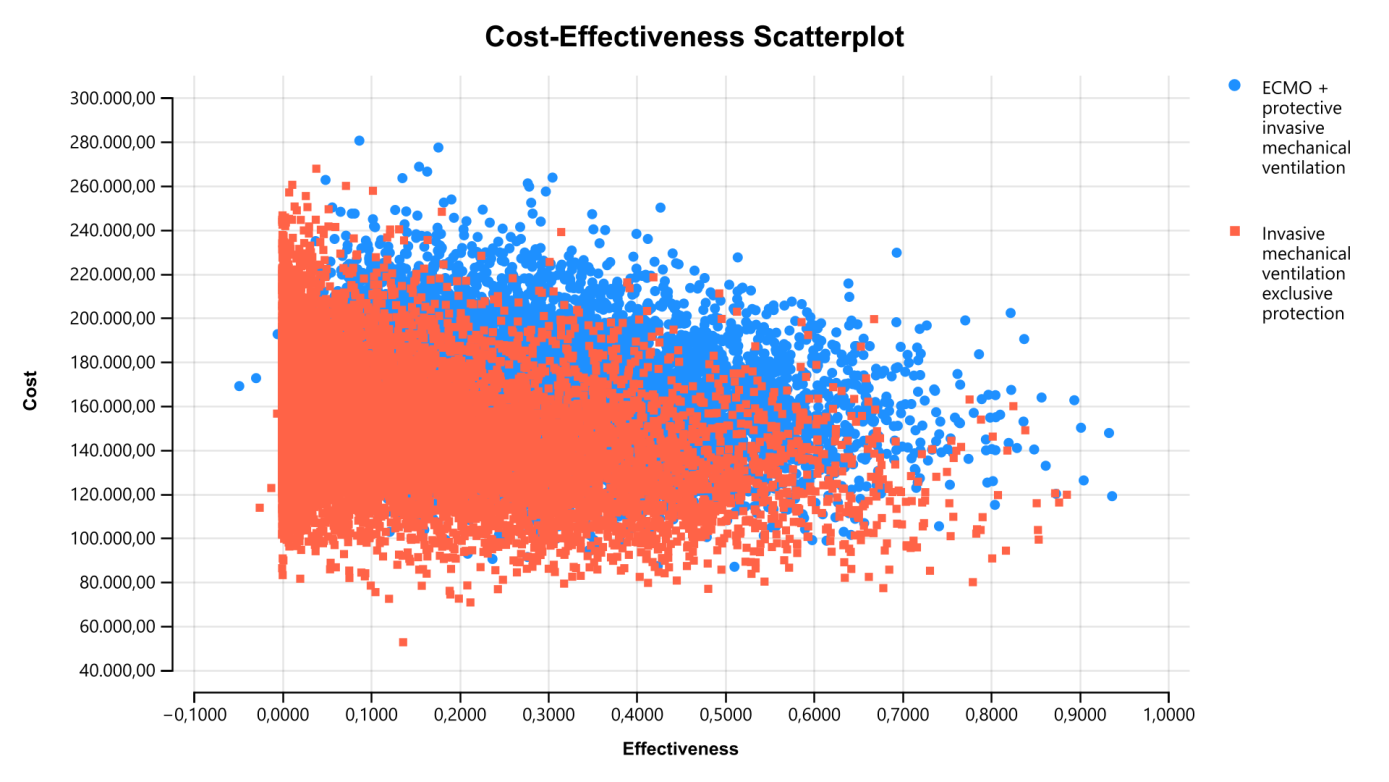
The cost-utility scatter plot (Figure 7) suggests greater dispersion of costs with the use of ECMO+VMI compared to VMI. There does not seem to be much difference in relation to the dispersion of the utility parameters. Greater dispersion suggests greater uncertainty around the parameters, in view of greater imprecision in terms of estimates.
The 10.000 Monte Carlo simulations show that at least 50% of the iterations are favorable to ECMO, considering the willingness to pay R$ 120,000.00. The summary of the proportions of interactions in the quadrants and respective components is shown in Table 7 below.
| Quadrant | Efe Incr | Custo Incr | Incr RCEI | Frequency | Proportion | |
|---|---|---|---|---|---|---|
| C1 | IV | IE>0 | IC<0 | Superior | 2908 | 0,2908 |
| C2 | Eu | IE>0 | IC>0 | RCEI<120000.0 | 2040 | 0,204 |
| C3 | III | IE<0 | IC<0 | RCEI>120000.0 | 171 | 0,0171 |
| C4 | Eu | IE>0 | IC>0 | RCEI>120000.0 | 2764 | 0,2764 |
| C5 | III | IE<0 | IC<0 | RCEI<120000.0 | 149 | 0,0149 |
| C6 | II | IE<0 | IC>0 | Inferior | 1968 | 0,1968 |
Table 8: RCEI Scatterplot Scatterplot Table Comparing ECMO+VMI and Exclusive VMI. Note: Incr= incremental; Efe= effectiveness. So
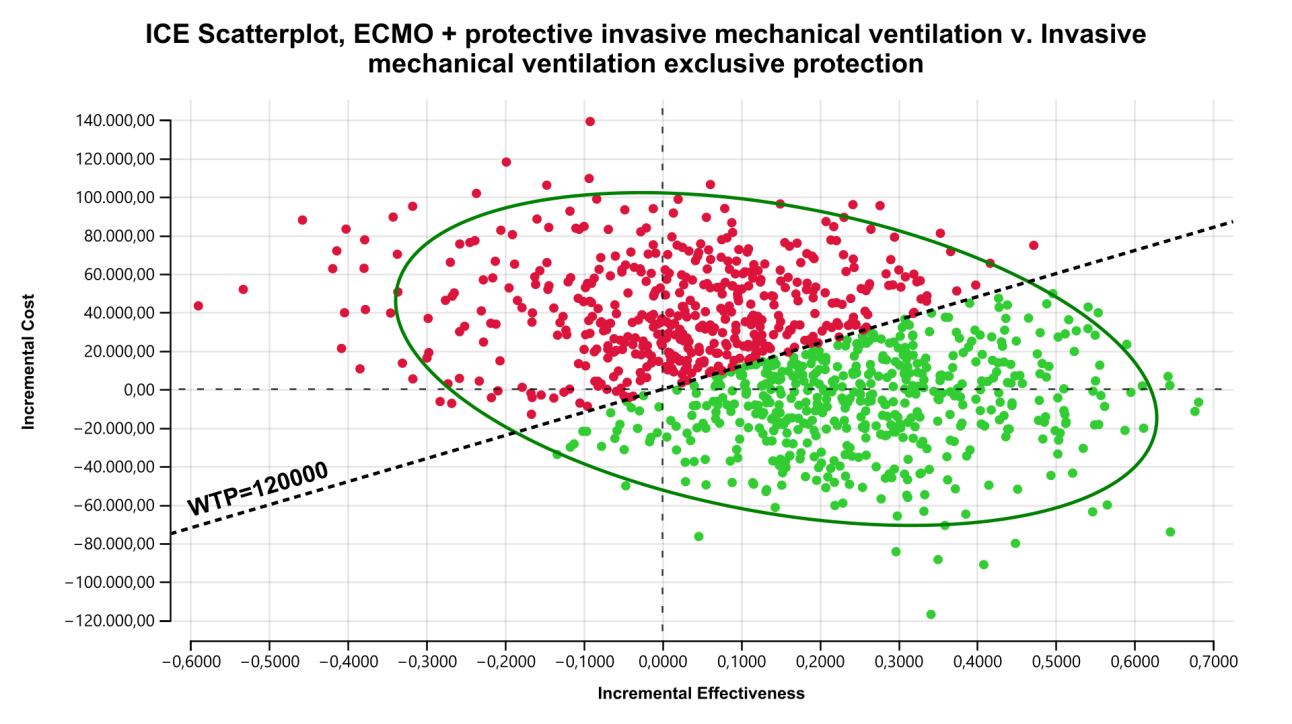
Table 7: RCEI Scatterplot Scatterplot Table Comparing ECMO+VMI and Exclusive VMI. Note: Incr= incremental; Efe= effectiveness. Source: The author, 2023 From the distributions attributed to the parameters of the model’s variables, and the proportions of iterations in each component of the quadrants, an ICE scatter plot was plotted (Figure 8). In the graph, the distribution of iterations between the quadrants should be interpreted as follows:
- The iterations that fell in component 1/quadrant IV represent a greater increase in effectiveness and a smaller increase in cost and an RCEI below R$ 12.000,00;
- The iterations that fell in component 2/quadrant I represent a greater increase in effectiveness and a greater increase in cost, with an RCEI lower than R$ 120.000,00;
- The iterations that fell in component 3/quadrant III represent a smaller increase in effectiveness and a smaller increase in cost, with an ICER greater than R$ 120.000,00;
- The iterations that fell in component 4/quadrant I represent a greater increase in effectiveness and a greater increase in cost, with an ICER greater than R$ 120.000,00;
- The iterations that fell in component 5/quadrant III offer a smaller increase in effectiveness and a smaller increase in cost, with an RCEI lower than R$ 120.000,00;
- The interactions that fell into component 6/quadrant II offer a smaller increase in effectiveness and a greater increase in cost, with an RCEI greater than R$ 120.000.00.
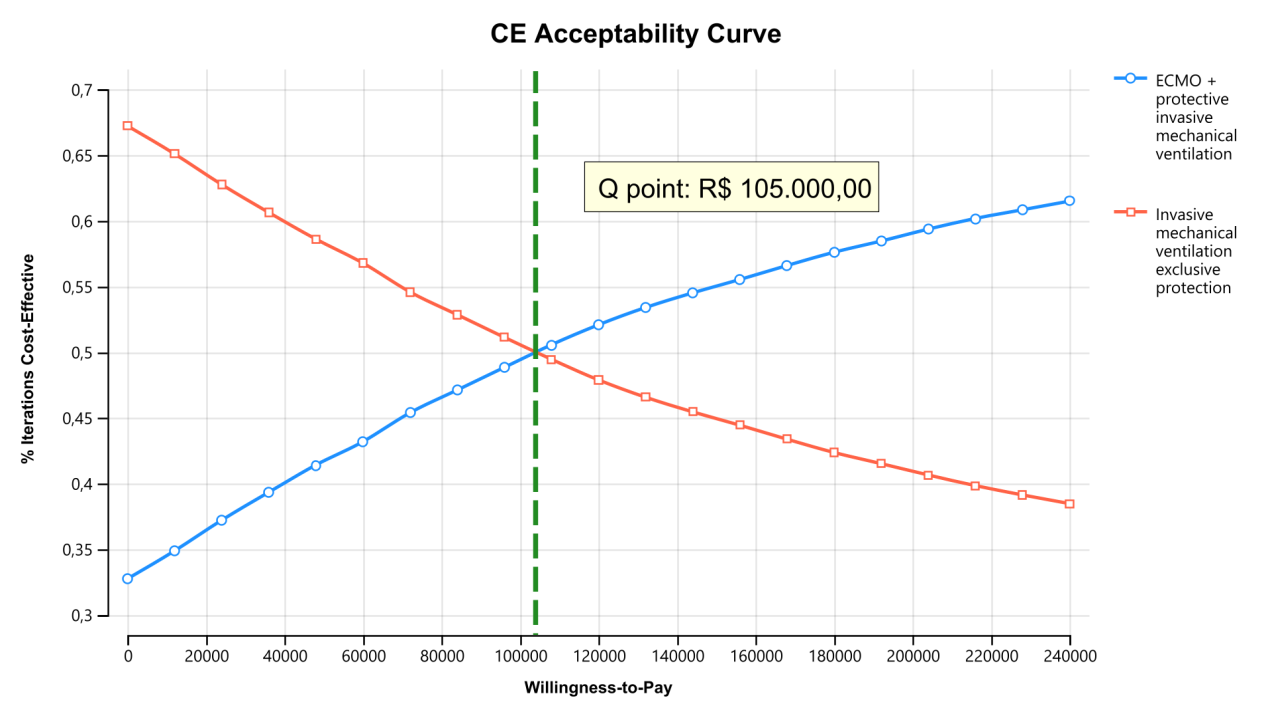
The acceptability curve shown in Figure 9 suggests that, starting from a disposition of R$ 105.000,00, the use of ECMO+ VMI is more likely to be cost-effective. Below this value, the use of exclusive VMI becomes the alternative most likely to be cost-effective. As the willingness to pay increases, the use of ECMO+VMI can reach a 65% probability of being the cost-effective alternative.
Discussion
Debates about the use of ECMO in patients with SDRA occurred on a large scale during the Pandemic period, with pressure exerted by the media and society on the acquisition of technology in the SUS for these cases, given the dissemination of information regarding the benefits of the its use. However, all acquisition of new technologies must follow a rigorous economic analysis in order to assess whether it is cost-effective for the SUS. That is, not only the possible benefits can be considered, but also the cost. In the case of ECMO, whether it is advantageous not only for the population, but also for the SUS, considering its additional cost for QALYs with its use.
The SDRA caused by COVID-19 causes inflammation of the lung parenchyma, making oxygenation difficult and leading the patient to hypoxemia. In this situation, there are two possible alternatives for rescue/treatment therapies, exclusive invasive mechanical ventilation and extracorporeal membrane oxygenation associated with mechanical ventilation. One of the criteria for ECMO contraindication is the risk of bleeding due to heparinization. Therefore, the choice of treatment depends on several clinical factors that need to be carefully evaluated by the medical team.
The effectiveness of ECMO in the treatment of patients with COVID-19 has been much questioned by health managers. Studies such as Peek’s, 2009, point out that the mortality of patients on MV in less than 6 months or before hospital discharge was 45%, while on ECMO it was 37%, suggesting a survival rate on ECMO of 63%. Most deaths of patients on MV were due to respiratory failure, while ECMO was due to multiple organ failure, in addition to leaving patients longer in intensive care. This study was included in CONITEC Report nº 636 of 2021, carried out precisely to answer health managers whether ECMO is cost-effective in the treatment of patients with SDRA.
The report pointed out that the mortality rate in patients with COVID-19 was 87,5% in patients with ECMO and 69,2% in patients with conventional therapy. The pooled odds of mortality on ECMO compared to conventional therapy were not significantly different (Estimate=0,273, 95%IC, 0,06 to 1,111; I2=0%, Cochran’s Q, p-value=0,57). Furthermore, due to the fact that the prices of equipment and inputs were higher during the Pandemic, and that there were few ECMO treatment centers in Brazil, it was not an opportune moment to include the technology in the SUS.
In the literature review of this dissertation, the 11
studies found evaluated mortality in patients with ARDS due to COVID-19 treated with VM and ECMO, but did not evaluate the costs and benefits of these technologies. Therefore, these data were extracted from the CONITEC report and the study by Conde, et al. [16].
According to the calculated variables in Table 4, the probability of a patient dying on MV was 0,408 while on ECMO it was 0,35 (DOMECQ, 2021). One of the unwanted effects of both technologies that may occur is sepsis, after all, both are composed of invasive devices, one for the pulmonary system (VM) and the other for the circulatory system (ECMO). In the study by Contrin, et al. [18], which evaluated the quality of life of patients who survived sepsis, the mortality rate was higher in patients with sepsis who were discharged from the hospital within one year, compared to those who were critically ill, however, no sepsis. A significantly higher prevalence of problems was also observed in older patients over 60 years of age with sepsis. And in this dissertation, the risks of developing sepsis and dying from sepsis in both technologies were analyzed.
According to the calculated variables in Table 4, the probability of a patient having sepsis on MV was 0,821 while on ECMO it was 0,448 [17]. Regarding quality of life, the report pointed to a trend in favor of ECMO. In the study by Nandasena [19], patients of advanced age, those with comorbidities, those admitted to the UTI, those who stayed in the UTI for a long time and those who were mechanically ventilated had a higher risk of poor quality of life after COVID-19.
Health professionals involved in this context need to be aware of economic evaluation methods and health technologies as a management tool for these technologies, so that it is possible to identify, among the available alternatives, the treatment that presents the best cost-effectiveness.
In this study, it was possible to demonstrate that both exclusive protective mechanical ventilation and ECMO associated with protective mechanical ventilation can be cost-effective alternatives for the treatment of SDRA, depending on the willingness to pay.
The results showed that there was no absolute dominance of one technology over the other, since, based on the estimated costs in the base case scenarios, as well as the probabilities of the clinical effects arising from the interventions and transition in the proposed analytical model, the results of the cost-utility analysis (Figure 5) showed that both exclusive VM and ECMO associated with protective VM could be cost-effective. From this perspective, considering the economic and financial condition of the SUS manager, a willingness-to-pay threshold is considered as a criterion for deciding on the best alternative. In this study, the amount of R$ 120.000,00 was considered as the willingness- to-pay threshold.
The analytical model proposed for the analysis of scenarios in the base case suggested that ECMO associated with protective VM in the SUS may result in an additional cost increase per AVAQ (effectiveness unit) of R$ 12.519,94 (Table 5). Since the willingness to pay threshold was approximately R$ 120,000.00, deciding to incorporate ECMO instead of exclusive VMI is supported by the argument that the greater the willingness to pay, the greater the effectiveness of ECMO. According to the acceptability curve chart (Figure 9), up to a limit of R$ 105,000.00 exclusive VMI is the most cost-effective alternative. And as the willingness to pay increases, that is, above R$ 105.000,00, ECMO associated with protective VM becomes the alternative most likely to be more cost-effective, considering a time horizon of 2 months with two Markov cycles lasting 30 days.
The model looks robust. Confidence in their results was attested by the deterministic multivariate sensitivity analysis and by the probabilistic sensitivity analysis, using 10.000 second-order Monte Carlo simulations, based on the acceptability curve and the incremental cost-effectiveness Scatterplot, which took into account consideration of the uncertainties of the values (parameters), demonstrating dispersion of both cost and effectiveness for each of the evaluated interventions.
Limitations
The proposed model was not concerned with knowing what happens to the patient after he is discharged, that is, the health status associated with this condition was also considered as an absorber, as well as death, which could impact the results found.
Conclusion
The analytical model suggested that ECMO associated with protective mechanical ventilation is more likely to be the most cost-effective alternative for treating patients with SDRA due to COVID-19 in the SUS, depending on willingness to pay. That is, if the manager is willing to pay for these patients to gain one more year of quality-adjusted life, an amount of R$ 68.902,92 (sixty-eight thousand, nine hundred and two reais and ninety-two cents), ECMO becomes more cost-effective, increasing the advantage over exclusive protective mechanical ventilation in terms of the probability of being cost-effective, the greater the willingness to pay, from R$ 120.000,00 (one hundred and twenty thousand reais).
References
-
(2020) Como estimar a mortalidade pela doença do novo coronavírus (COVID-19), Informe científico
-
4 de agosto de, Disponível, OPAS.
-
WHO. Coronavirus disease (COVID-19).
-
Nishiura H, Jung SM, Linton NM, Kinoshita R, Yang Y, et al. (2020) A extensão da transmissão do novo coronavírus em Wuhan, China, 2020. J Clin Med 9: 2-5.
-
Levi M, Ccomeu H (1999) Disseminated intravascular coagulation. N Engl J Med 341(8): 586-592 .
-
Pinheiro BV, Pinheiro GSM, Mendes MM (2015) Entendendo melhor a Insuficiência Respiratória Aguda. A better understanding of acute respiratory failurePulmão RJ 24(3): 3-8.
-
DATA SUS (2019) TabNet Win32 3.0: Morbidade Hospitalar do SUS. Internações por doenças do aparelho respiratório.
-
DATA SUS (2020) TabNet Win32 3.0: Morbidade Hospitalar do SUS. Internações por doenças do aparelho respiratório.
-
DATA SUS (2021) TabNet Win32 3.0: Morbidade Hospitalar do SUS. Internações por doenças do aparelho respiratório.
-
Ranzani OT, Bastos LSL, Gelli JGM, Marchesi JF, Baião F, et al. (2021) Caracterização das primeiras 250 000 internações hospitalares por covid-19 em brasaB: uma análise retrospectiva de dados de abrangência nacional. A lanceta medicina respiratória 9: 407-418.
-
Dondorp AM, Hayat M, Aryal D, Beane A, Schultz MJ (2020) Suporte respiratório em pacientes com COVID-19, com foco em configurações com recursos limitados. A revista americana de medicina tropical e higiene 102(6): 1191-1197.
-
Lind, Jolline (2021) Oxigenação por Membrana Extracorpórea no Tratamento de Pacientes com COVID-19: Revisão Integrativa. Revista Paranaense de Enfermagem 4: 42-50.
-
(2021) Brasila. Oxigenação extracorpórea (ECMO) para apoiar pacientes com insuficiência respiratória grave e refratária. Brasília. Ministério da Saúde. Relatório de Recomendação nº 636.
-
Morris AH, Wallace CJ, Menlove RL, Clemmer TP, Orme JF, et al. (1994) Ensaio clínico randomizado de ventilação da razão inversa controlada por pressão e remoção extracorpórea de CO2 para síndrome do desconforto respiratório do adulto. Am J Respir Crit Care Med 149: 295-305.
-
Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, et al. (2009) Eficácia e avaliação econômica do suporte ventilatório convencional versus oxigenação por membrana extracorpórea para insuficiência respiratória grave em adultos (CESAR): um ensaio clínico randomizado e controlado multicêntrico. Lanceta 374: 1351-1363.
-
Domecq JP, Lal A, Sheldrick CR, Kumar VK, Boman K, et al. (2021) Society of Critical Care Medicine Discovery Viral Infection and Respiratory Illness Universal Study (VIRUS): COVID-19 Registry Investigator Group. Resultados de pacientes com doença por coronavírus 2019 recebendo terapias de suporte a órgãos: o registro internacional de estudo universal de infecção viral e doenças respiratórias. Crit Care Med 49: 437-448.
-
Conde KAP, Silva E, Silva CO, Ferreira E, Freitas FGR, et al. (2013) Diferenças no Tratamento da Sepse e Resultados entre Hospitais Públicos e Privados no Brasil: Um Estudo Observacional Multicêntrico. PLoS ONE 6: 1-11.
-
Allyn J, Ferdynus C, Lo Pinto H, Bouchet B, Persichini R, et al. (2018) Padrões de complicações em pacientes submetidos à oxigenação por membrana extracorpórea venoarterial em unidade de terapia intensiva: análise de correspondência múltipla e classificação ascendente hierárquica. PLoS One 13: 1-9.
-
Contrin LM, Paschoal VD, Beccaria LM, Cesarino CB, Lobo SMA (2013) Qualidade de vida de sobreviventes de sepse grave após alta hospitalar. Rev. Latino-Am. Enfermagem 3: 1-8.
-
Nandasena HMRKG, Pathirathna ML, Atapattu AMMP, Prasanga PTS (2022) Qualidade de vida de pacientes com COVID 19 após a alta: Revisão sistemática. PLoS ONE 2: 1-12.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City