Promoting Transfer of Learning Using the ‘Window of Opportunity’ in Emergency Nursing Education
Emergency nurses in training struggled to transfer their classroom learning into practice regarding traumatic brain injury (TBI). Consequently, secondary brain injury could occur. In this conceptual paper, we combined Tanner’s model of clinical judgement in nursing, the conceptual framework for educational design at the modular level, and knowledge levels to devise a strategy to promote the transfer of learning among emergency nursing students regarding the management of TBIs. Through a guided process, the students first learned the process of analytical clinical reasoning and practiced the process in class and then under supervision in the ED. Finally, they demonstrated their competence and transferal of their knowledge into a realworld environment during a summative assessment task.
Introduction
Globally, emergency nurses have to provide increasingly complex care resulting in greater cognitive demands. Emergency nurses play a pivotal role in providing quality care and improving patient outcomes [1]. Consequently, they need a broad range of knowledge and skills to care for health care issues ranging from non-urgent to life-threatening conditions affecting people of all age groups [2]. In particular, emergency nurses have to be able to manage patients presenting with traumatic brain injuries (TBIs), which are a leading cause of long-term disability and death Conceptual Paper across all ages across the globe [3, 4]. In the United States America, the Centers for Disease Control and Prevention recorded almost 223,135 TBI-related hospitalizations and approximately 64,362 TBI-related deaths in 2020 [5]. In South Africa, 89,000 new cases of TBI are reported annually [6].
TBI patients are initially managed in the Emergency Department (ED) and may present with either primary or secondary brain injuries. Primary brain injuries occur at the moment of the injury when the physical structures of the brain are displaced causing irreversible damage. Secondary brain injuries occur minutes to hours after primary injury and can result from insults such as ischemia, cerebral hypoxia, hypercapnia, hypotension, cerebral edema, and changes in blood flow to the brain, which raise intracranial pressure (ICP) and the likelihood of adverse outcomes [7]. During initial resuscitation, patients with TBI in the ED should be stabilized, and raised ICP should be managed to minimize secondary brain injuries and improve patient outcomes [6, 7, 8].
As educators, we observed that emergency nursing students struggled to notice and interpret warning signs of raised ICP. Consequently, students could not implement interventions to prevent secondary brain injuries [9]. This implies that emergency nursing students will not be able to transfer learning to clinical settings, which will have negative consequences for patient outcomes.
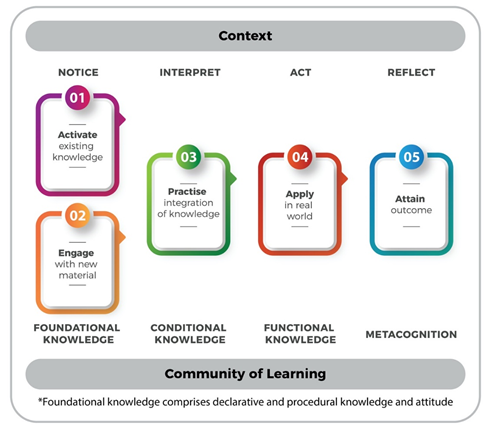
We thus recognized a need to promote transfer of learning for emergency nursing students regarding TBIs. We also recognized that outdated teaching strategies cannot adequately prepare emergency nurses in the 21st century [10]. We thus combined Tanner’s model [11] of clinical judgement in nursing, the conceptual framework for educational design at the modular level, [12] and knowledge levels to devise a strategy [13] to promote the transfer of learning among emergency nursing students regarding the management of TBIs (Figure 1).
Approach
We based our strategy on the conceptual framework developed by Botma and Heyns used to promote transfer of learning (Figure 1), which is nested in the constructivist learning theory. Although the conceptual framework is presented linearly, transfer of learning is an iterative cyclic process, cycling through four levels of knowledge. The four levels of knowledge include foundational, conditional, functional, and metacognitive knowledge (Figure 1). A community of learning can be defined as the environment where students interact in class and in practice to attain learning outcomes, starting with foundational knowledge and aiming for metacognition [12]. Educators should guide students to apply their foundational knowledge in a specific context, [12] for example, in the emergency department. Foundational knowledge includes knowing “what is” and “how to do things” [13] and can help students to identify and explain deviations from the norm [11]. To expand foundational knowledge, students must recall existing knowledge while actively engaging with new material [12].
Conditional knowledge or “knowing when to do things” [13] promotes clinical reasoning and enables the student to interpret data, recognize patterns, and formulate differential diagnoses [11]. Interpreting data is vital for planning and implementing interventions, and evaluating patients’ responses. Conditional knowledge can be fostered in the classroom or at the bedside. Finally, functional knowledge promotes clinical judgment and enables students to apply all levels of knowledge [13] to solve patient specific problems and function as competent professionals aiming to improve patient outcomes [11]. According to Botma Y, et al. students should establish reflective practices to evaluate their own competence and thinking processes. Through metacognitive processes, students should be able to determine whether they have attained learning and patient outcomes.
Step 1: Activate Existing Knowledge By the time nursing students specialize in emergency nursing, they should have a certain level of competence about how to manage TBIs and raised ICP. This knowledge is learnt during their undergraduate studies and from clinical ED experience. To activate their existing knowledge, we asked students to think to a patient presenting with a TBI being managed in the ED. Students then had to test their foundational knowledge by explaining the assessment findings that confirmed raised ICP; they then had to explain the interventions for managing raised ICP (Figure 1).
Step 2: Engage with New Material In this step, students engaged with new information including current literature, videos, evidence-based care bundles, and guidelines. The students were divided into small groups and tasked with organizing the management of patients with raised ICP using the template in Figure 2 as a guide. The educator and clinical facilitator briefly explained the layout of the template, which the students referred to as the “Window of Opportunity.” Table 1 was added as an addendum to the template explaining the “ABCDEFG” mnemonic used in the ED with related prompts. Students were encouraged to discuss their understanding of the literature and share their own ideas and experiences within their community of learning, once again applying their foundational knowledge.
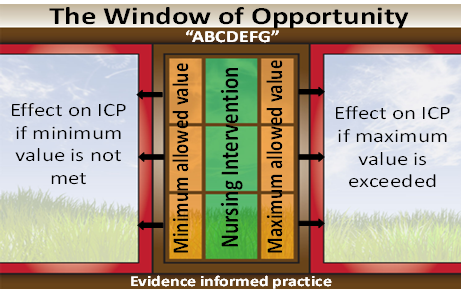
Each group then presented their collaboratively compiled “Window of Opportunity” to the entire community of learning. The facilitators documented the content presented by each group on a flip chart until no new information emerged. The task aimed to strengthen and expand declarative knowledge regarding the management of patients with TBI presenting with raised ICP. The practice of integrating knowledge expanded conditional knowledge, which is essential for noticing and interpreting deviations from the norm, to explain the phenomenon, plan interventions, and understand consequences [13].
| Components | Prompts |
|---|---|
| Airway | Open (O), maintained (M), and protected (P); endotracheal suctioning; head elevation (keeping the Glascow Coma Scale (GCS) in mind as it effects the patient’s ability to OMP his/her airway) |
| Atlas & Axis | Neck position, neck collar |
| Breathing | Respiratory rate |
| Arterial blood gas monitoring: SaO , pO and pCO 2 2 2 | |
| Mechanical ventilation: Tidal volume (VTi), respiratory rate, and positive end-expiratory pressure (PEEP) | |
| Circulation | Hemodynamic monitoring: Heart rate, systolic blood pressure, pulse pressure, mean arterial pressure, cerebral perfusion pressure, temperature, central venous pressure and urine output |
| Laboratory monitoring: Serum-Osmol, sodium (Na+) and hemoglobin (Hb) | |
| Disability | Glasgow Coma Scale, pupil size and reaction to light, and intracranial pressure monitoring |
| Drugs | Rapid sequence intubation (RIS), sedatives, analgesia, barbiturates, neuro-muscular blockade agents, anti- convulsants, and hyperosmolar therapy |
| Environment | Controlled: Dark and quiet |
| Safe: Alarm limits | |
| Fitting | Seizures |
| Family | Informed and involved |
| Glucose | Serum-glucose |
Table 1: The ABCDEFG mnemonic adapted for patients presenting with a traumatic brain injury to the emergency department.
Step 3: Practice Integration of Knowledge During this step, students were given a paper-based and real-life case and asked to record any deviations and interpret these deviations using their conditional knowledge summarized in the Window of Opportunity (Table 1). The activity can be done individually or collaboratively. Students presented their interpretations of the cases and received feedback from the community of learning, which promoted clinical reasoning. After agreement had been reached on all deviations and interpretations, evidence-based interventions were collectively planned.
Apply in Real World
In the ED where the students practiced, the mean overall length of stay (from reporting to reception to being transferred) for critically ill or injured patients (such as those with TBI) was 3.04 days, which was defined as a prolonged length of stay [14]. Students then had the opportunity to demonstrate their procedural and functional knowledge (notice, interpret, and act) in a real-world setting under the supervision of a clinical facilitator. The clinical facilitator guided the student’s in- and on-action reflection, fostering metacognition.
Attain Outcome
Students were assessed to confirm their competency and attainment of learning outcomes in a real-world setting by an educator and clinical facilitator. Students had to notice, interpret, act, and reflect on their knowledge. Students were expected to reflect on-action to indicate what was done well, what could be done differently, and identify knowledge shortfalls, testing their functional knowledge and level of metacognition.
Conclusion
Emergency nurses need to deliver quality care to patients in EDs. Nurses in ED should be able to manage patients presenting with TBIs to prevent severe secondary brain injuries. As educators, we recognized that emergency nursing students were not confident when they had to manage patients presenting with TBI, and we consequently combined various learning models/conceptual frameworks to create an integrated learning and teaching framework suitable for the 21st century. Here, we described the step- by-step application of the integrated conceptual framework to promote transfer of learning. We encourage testing the “Window of Opportunity” for other urgent and non-urgent conditions on patients of all ages to test its applicability in other EDs. Using the process described in this toolbox article, educators could educate competent emergency nurses, which will promote positive patient outcomes.
Acknowledgements
Cheryl Tosh for editing the manuscript, and Marizanne Booysen for graphically designing the ‘Window of Opportunity’ image.
References
-
Brim CB (2022) Emergency nurse certification. J Emerg Nurs 48(3): 299-302.
-
Zaleski ME (2019) Emergency nurse orientation. J Emerg Nurs 45(5): 551-555.
-
Foks KA, Cnossen MC, Dippel DWJ, Maas Andrew IR, Menon David, et al. (2017) Management of mild traumatic brain injury at the emergency department and hospital admission in Europe: a survey of 71 neurotrauma centers participating in the CENTER-TBI study. J Neurotrauma 34(17): 2529-2535.
-
Rakhit S, Nordness MF, Lombardo SR, Cook M, Smith L, et al. (2021) Management and challenges of severe traumatic brain injury. Semin Respir Crit Care Med 42(1): 127-144.
-
Centers for Disease Control and Prevention. National Center for Health Statistics: mortality data on CDC WONDER.
-
Gxolo N (2023) A leading cause of death in SA, head trauma is under-researched.
-
Lund SB, Gjeilo KH, Moen KG, Schirmer MK, Skandsen T, et al. (2016) Moderate traumatic brain injury, acute phase course and deviations in physiological variables: an observational study. Scand J Trauma Resusc Emerg Med 24: 77.
-
Awad SM, Ahmed HH, Kandeel N (2022) Integration of evidence-based care bundle in traumatic brain injury patients’ care. Am J Nurs Res 10(1): 34-40.
-
El Hussein MT, Zettel S, Suykens AM (2016) The ABCs of managing increased intracranial pressure. J Nurs Educ Pract 7(4): 6-14.
-
Banerjee S, Kumar S, Dzousa C (2022) Effectiveness of concept mapping versus traditional approach as a teaching method on knowledge regarding selected topics among nursing students. Int J Nurs Educ 14(1): 1-8.
-
Tanner CA (2006) Thinking like a nurse: A research- based model of clinical judgment in nursing. J Nurs Educ 45(6): 204-211.
-
Botma Y, Brysiewicz P, Chipps J, Mthembu S, Phillips M (2013) Creating Stimulating Learning Opportunities.
-
Biggs J (1999) what the student does: teaching for enhanced learning. Higher Educ Res Dev 18(1): 57-75.
-
Mashao K, Heyns T, White Z (2021) Areas of delay related to prolonged length of stay in an emergency department of an academic hospital in South Africa. Afr J Emerg Med 11(2): 237-241.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City