Progeria
Progeria is a rare genetic disease with striking features that resemble accelerated aging. The inheritance pattern, paternal age effect, and lack of consanguinity argue that it is due to a sporadic dominant mutation. We have observed elevated levels of hyaluronic acid (HA) excretion in progeria patients.
Introduction
The word Progeria comes from the Greek rogeros meaning ‘prematurely old’. It was first described in an academic journal by Dr. Jonathan Hutchinson in 1886 and Dr. Hastings Gilford in 1897-both in England. The condition was later named Hutchinson-Gilford Progeria Syndrome (HGPS). It is currently hypothesized to result from a gene mutation arising around the time of conception or shortly thereafter [1, 2].
Definition
Progeria is an extremely rare, fatal genetic condition that affects children and gives them an appearance of accelerated aging [3].
Prevalence
• Progeria is listed as a “rare disease” by the Office of Rare Diseases (ORD) of the National Institutes of Health (NIH) [4].
- HGPS prevalence is reported to be 1 in 8 million births [5].
- The true prevalence, however, has been suggested to be closer to 1 in 4 million births because many cases likely go undiagnosed or are misdiagnosed [6].
Progeria, or Hutchinson-Gilford progeria syndrome (HGPS), is an extremely rare genetic disorder, and its prevalence across different populations is generally consistent with its overall rarity. However, there may be slight variations in prevalence due to factors such as genetic diversity, geographic location, and access to healthcare. Here’s a general overview: Global Prevalence: Progeria is estimated to occur in about 1 in 4 to 8 million live births worldwide. This means that on average, there might be just a few hundred cases worldwide at any given time. Ethnic and Racial Groups: Progeria has been reported in various ethnic and racial groups, including Caucasians, African-Americans, Hispanics, and Asians. While there may be some differences in prevalence among these groups, the overall rarity of the condition remains consistent. Geographic Distribution: Progeria has been documented in many countries around the world, including the United States, Europe, Asia, and Africa. However, due to its rarity, the number of reported cases may vary from region to region. Consistency of Prevalence: Despite variations in population demographics and geographic locations, the prevalence of progeria remains low and relatively consistent across different populations. Research and Awareness: Research efforts and increased awareness of progeria have led to more accurate diagnosis and reporting of cases worldwide. This ongoing research may provide further insights into the prevalence and distribution of progeria in different populations.
Overall, while progeria can affect individuals from diverse backgrounds, its rarity means that it is consistently uncommon across different populations [7].
The prevalence of progeria in India, like in most countries, is extremely low due to the rare nature of the condition. Progeria affects approximately 1 in 4 to 8 million live births worldwide, and this prevalence is generally consistent across different populations, including those in India [8].
Fertility
In general, people with progeria have such severe failure to thrive (poor growth from the time of childhood) that it prevents fertility.
- The absence of complete sexual maturation has been considered characteristic of the syndrome.
- Yet a case described and published at 1989 by endocrinologists in Spain reported that a 32-year-old woman with progeria had delivered a child at age 23 which means that she must have been sexually mature to deliver the child.
- However sexual maturity is rare in these patients [3].
Prognosis
- As there is no known cure, the average life expectancy for a patient with HGPS is 13 years, with an age range of 7-27 years.
- At least 90% of patients die from complications of atherosclerosis, such as heart attack or stroke.
- Mental development is not adversely affected; in fact, intelligence tends to be above average.
- With respect to the features of aging that progeria appears to manifest, the development of symptoms is comparable to aging at a rate eight to ten times faster than normal.
- With respect to features of aging that progeria does not exhibit, patients show no neuro degeneration or cancer predisposition.
- They also do not develop the so-called “wear and tear” conditions commonly associated with aging, such as cataracts (caused by UV exposure) and osteoarthritis (caused by mechanical wear) [7].
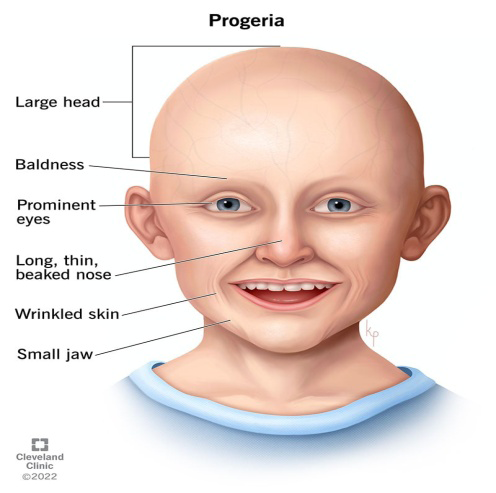
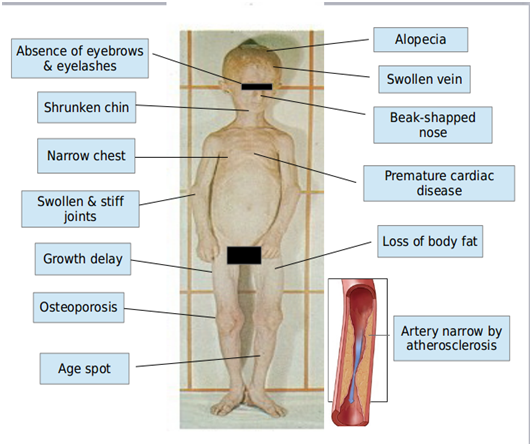
Symptoms
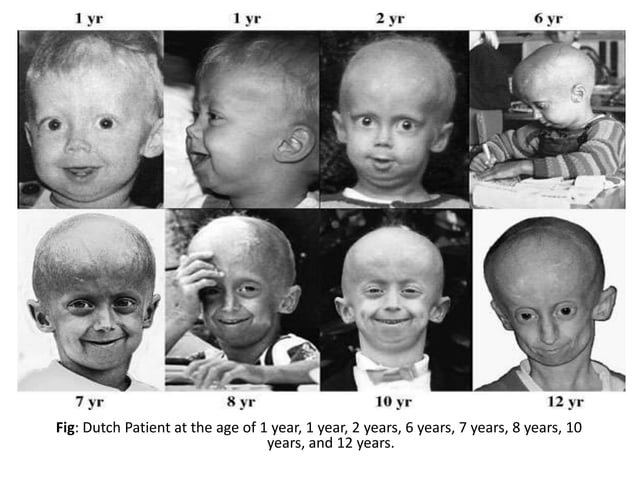
Although they are born looking healthy, children with Progeria begin to display many characteristics of accelerated aging at around 18-24 months of age. The children have a remarkably similar appearance, despite differing ethnic backgrounds [3]. Most of the following features are manifested after the age of three years in children with Hutchinson-Gilford Progeria Syndrome (Figures 1-3).
Types of Progeria
Classical HGPS
Classically affected patients strongly resemble one another.
Non Classical-Atypical-HGPS
A group of patients with progeria that show a definite overlap with patients with other syndromes“e.g. [9] mandibulo-acral dysostosis (MAD)” (Table 1).
| Classical HGPS | Non-classical progeria | |
|---|---|---|
| Growth Deficiency | ||
| Prenatal | Mild | Mild |
| Post natal | Severe | Mild |
| Lipid dystrophy | Expressed | Slower but in the end expressed everywhere exceptcheeks, submandibular, and suprapubic region |
| Hair loss | Expressed | Variable , Minimal to severe |
| Scleroderma | Moderate | Moderate |
| Osteolysis | ||
| Acra | Moderate | Expressed |
| Clavicles | Mild | Expressed |
| Mandible | Moderate | Expressed |
| Viscerocranium | Moderate/ Severe | Mild, Slowly progressive |
| Neurocranium | Mild | Expressed |
| Fractures | Late; Head | Early ; Humeri, Ribs |
| Vascular problems | Early ; Expressed | Often late, but sometimes early |
Table 1: Differences between Classical Hutchinson-Gilford Progeria Syndrome and Non-Classical Progeria.
Genetic Causes
• Mutations in the LMNA gene cause Hutchinson-Gilford progeria syndrome.
- LMNA gene is located on chromosome 1q22 and is composed of 12 exons.
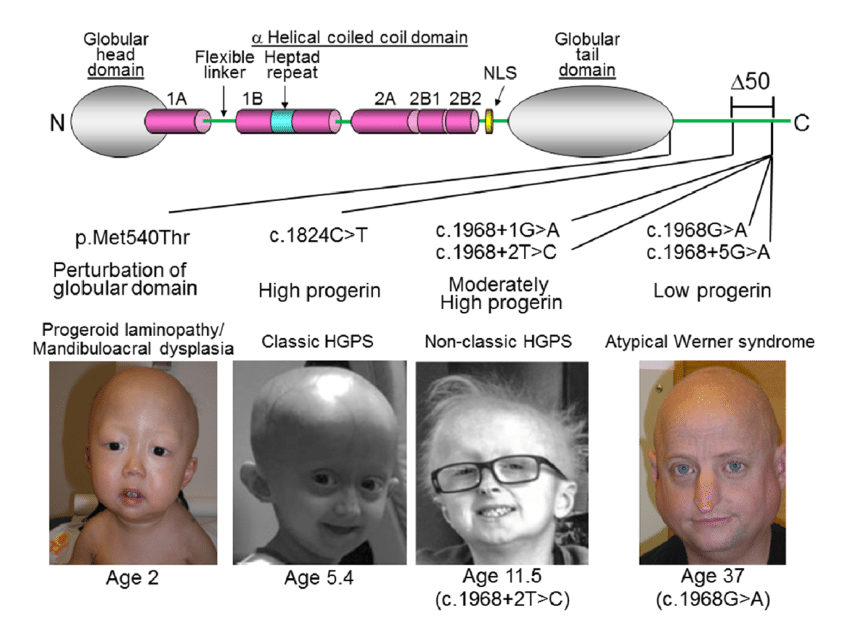
- Only four causative heterozygous mutations for [10] HGPS in LMNA are recognized (Figure 4).
Genetic Causes Classic HGPS
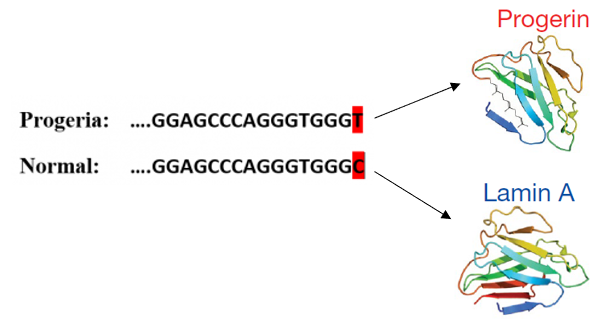
- c.1824C>T transition in exon 11 results in a silent Gly-to- Gly change at codon 608 (p.Gly608Gly).
- This silent change results in increased usage of an internal cryptic spice site resulting in an in-frame deletion of 150 nucleotides and50 amino acids from the lamin A protein [11].
Atypical HGPS • 1822G>A (p.Gly608Ser), c.1821G>A (p.Val607Val), or c.1968+1G>A 11 (Figure 5)
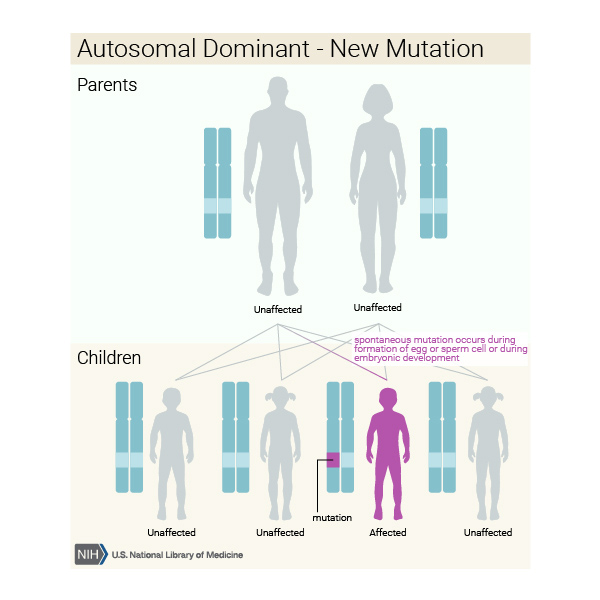
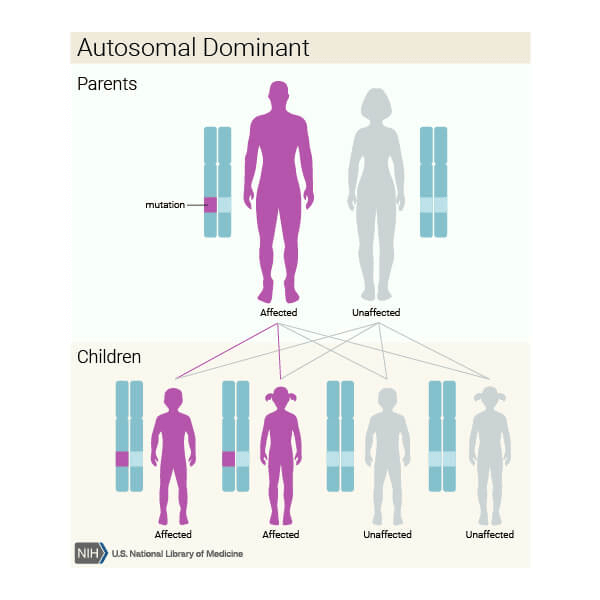
Mode of Inheritance
- HGPS is not usually passed down in families.
- The gene change is almost always a chance occurrence that is extremely rare.
- However, HGPS is considered [12] a “sporadic auto somal dominant” mutation (Figure 6).
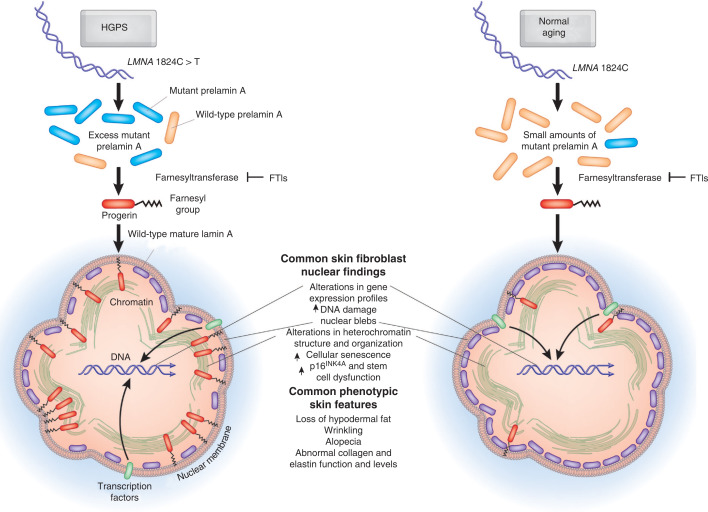
Molecular Basis of Disease
- Lamin A is an inner nuclear membrane protein with both structural and cell signaling effects.
- The single C to T transition at nucleotide 1824 of LMNA does not change the translated amino acid (Gly608Gly), but activates a cryptic splice site, resulting in the deletion of 150base pairs in the 3’ portion of exon 11.
- Translation followed by post-translational processing of this altered mRNA produces a shortened abnormal pre lamin A protein with a 50 amino-acid deletion, hence forth called “progerin”.
- A key to disease in HGPS is the presumably persistent farnesylation of progerin, which renders it permanently intercalated into the inner nuclear membrane where it can accumulate and exert progressively more damage to cells as they age.
- The inability to release progerin from the nuclear Figure 7 membrane results in structural stress on the nucleus.
- It is hypothesized that this permanently farnesylated mutant form of pre lamin A (progerin) [13] leads to the progressive defects in nuclear architecture that are seen in HGPS (Table 2).
| Steps In Norm Al Cell | Steps In Progeria Cell |
| The gene LMNA encodes a protein called prelamin A | The gene LMNA encodes a protein called prelamin A |
| Prelamin A has a farnesyl group attached to its end | Prelamin A has a farnesyl group attached to its end |
| Farnesyl group is removed from prelamin | Farnesyl group remains attached to prelamin A |
| Abnormal form called PRELAMIN A | Abnormal form of prelamin A called PROGERIN |
| Prelamin A is not anchored to the nuclear rim | Progerin is anchored to the nuclear rim |
| Normal state of the nucleus | Abnormally shaped nudeus |
Table 2: above diagram shows, Steps in Norm Al & Progeria Cell’s.
Outcome of Disease
The outcomes for individuals with progeria can vary, but the condition typically leads to a shortened lifespan and various health complications. Here are some key aspects of the outcome of progeria: Shortened Lifespan: Most individuals with progeria have a significantly shortened lifespan compared to the general population. The average life expectancy for individuals with progeria is around 14 years, although some individuals may live into their late teens or early twenties. Cardiovascular Complications: Progeria primarily affects the cardiovascular system, leading to various complications such as atherosclerosis (hardening and narrowing of the arteries), cardiovascular disease, and stroke. These complications significantly contribute to the shortened lifespan of individuals with progeria. Physical Characteristics: Progeria causes characteristic physical features associated with premature aging, including growth failure, loss of subcutaneous fat, joint stiffness, hair loss, and skeletal abnormalities. These physical changes can impact mobility and quality of life. Other Health Issues: In addition to cardiovascular complications, individuals with progeria may experience other health problems such as skeletal abnormalities, dental issues, hearing loss, and vision problems [14].
Diagnosis
The diagnosis is based on recognition of common clinical features and Molecular genetic testing of LMNA, the only gene known to be associated with HGPS [14]. Molecular Genetic Testing
- Targeted Mutation Analysis can be used to identify the pathologic variant c.1824C>T (p.Gly608Gly), the common recurrent de novo LMNA mutation in exon 11 that defines classic HGPS.
- Sequence Analysis of the entire coding region and associated splice junctions identifies:
- c.1824C>T, the common mutation that defines classic HGPS
- c.1822G>A (p.Gly608Ser), c.1821G>A (p.val607Val), andc.1968+1G>A, the other three mutations that define atypical HGPS
- Other sequence variants in the gene that may be associated with other progeroid syndromes.
- Urinary Hyaluronic Acid is not a valid test for the diagnosis of HGPS. Although urinary hyaluronic acid has been reported to be increased in children with HGPS, the measurement is now regarded as unreliable [15]. Prenatal Diagnosis and Pre Implantation Genetic Diagnosis (PGD)
- Parental diagnosis and PGD for at-risk pregnancies require prior identification of the disease-causing mutation in the family.
- Of note, recurrence within a family is rare given that most mutations are de novo and germ line mosaicism is rare [16].
Treatments
- There’s no cure for progeria.
- Regular monitoring for cardiovascular disease may help with managing the child’s condition.
- Some children undergo coronary artery bypass surgery or dilation of cardiac arteries (angioplasty) to slow the progression of cardiovascular disease.
- Certain therapies may ease or delay some of the signs and symptoms. They include:
- Low-dose aspirin. A daily dose may help prevent heart attacks and stroke.
- Other medications. Depending on the child’s condition, doctor may prescribe other medications, anticoagulants to help prevent blood clots.
- The use of growth hormone may help increase height and weight.
- Physical and occupational therapy. These may help with joint stiffness and hip problems and may allow the child to remain active.
- Extraction of primary teeth. Extraction may help prevent problems associated with the delayed loss of baby teeth [14].
Life Style and Home Remedies
- Some steps you can take at home that may help progeria child include:
- Make sure the child stays well hydrated. Dehydration can be more serious in children with progeria. Be sure the child gets enough to drink, especially during an illness or in hot weather.
- Provide frequent, small meals. Because nutrition and growth can be an issue for children with progeria, giving the child smaller meals more often may help to increase his or her caloric intake.
- Provide opportunities for regular physical activity. Check with the child’s doctor to learn which activities are right for the child.
- Get cushioned shoes or shoe inserts for the child. The loss of body fat in the feet can cause discomfort.
- Make sure the child is up to date on childhood immunizations. A child with progeria isn’t at increased risk of infection, but like all children is at risk if exposed to infectious diseases. Provide learning opportunities: Progeria won’t affect the child’s intellect, so he or she can attend school at an age- appropriate level [13]. Therapies under Investigation
- FTIs-a potential drug treatment for children with Progeria:
- Drugs known as Farnesyl Transferase Iinhibitors (FTIs), which were developed for treating cancer, have shown promise in laboratory studies in correcting the cell defects that cause progeria.
- FTIs are currently being studied in human clinical trials for treatment of progeria.
- Progeria research foundation (PRF)-funded study Identifies Rapamycin as Possible Treatment for Progeria:
- Researchers at the National Institutes of Health and Massachusetts General Hospital in Boston, MA published anew study in Science, Translational Medicine that may lead to a new drug treatment for children with Progeria.
- Rapamycin is an FDA approved drug that has previously been shown to extend the lives of non-progeria mouse models.
- This new study demonstrates that rapamycin decreases the amount of the disease-causing protein progerin by 50%, improves the abnormal nuclear shape, and extends the lifespan of progeria cells.
- This study provides the first evidence that rapamycin may be able to decrease progerin’s damaging effects in children with progeria [16].
Progeria Research Foundation
The Progeria Research Foundation (PRF) was established in the United States in 1999 by the parents of a child with Progeria, Drs. Leslie Gordon and Scott Berns, and many dedicated friends and family who saw the need for a medical resource for the doctors, patients, and families [17] of those with Progeria and for funding of Progeria research (Figures 8-10).

Sampson Gordon Berns (October 23, 1996-January 10, 2014) was an American activist with progeria, an extremely rare and fatal disease that causes the body to age rapidly. Berns helped raise awareness about the disease and he was the subject of the HBO documentary Life According to Sam, which was first screened in January 2013 [18].
Since that time, PRF has become a driving force for promoting advances in the field, including the 2003 historic discovery of the Progeria gene, and has developed a comprehensive network of to aid those affected by Progeria and those researchers who want to conduct Progeria research. PREF is the only non-profit organization worldwide solely dedicated to finding treatments and the cure for Progeria [17].
Measures to Decline the Disease Progress
Efforts to slow down the progression of progeria and improve the quality of life for affected individuals primarily focus on supportive care and potential therapeutic interventions. Here are some measures that may help in managing progeria:
Cardiovascular Monitoring and Management: Regular monitoring of cardiovascular health is essential for individuals with progeria due to the high risk of cardiovascular complications such as atherosclerosis and cardiovascular disease. This may include regular check-ups with a cardiologist, monitoring blood pressure and cholesterol levels, and implementing lifestyle modifications such as a heart-healthy diet and regular exercise (as tolerated). Medications: Some medications may be prescribed to manage specific symptoms or complications associated with progeria. For example, individuals may be prescribed aspirin or statins to help reduce the risk of cardiovascular events, and pain management medications may be used to alleviate joint stiffness and discomfort. Physical Therapy: Physical therapy can help improve mobility, flexibility, and strength in individuals with progeria. Therapists can provide exercises and techniques to help maintain range of motion, prevent contractures, and manage musculoskeletal issues. Nutritional Support: Proper nutrition is important for overall health and well-being. A balanced diet rich in nutrients can help support growth, development, and overall health in individuals with progeria. Nutritional supplements may also be recommended if dietary intake is inadequate. Research and Clinical Trials: Ongoing research into the genetics and biology of progeria has led to the identification of potential therapeutic targets. Clinical trials are underway to evaluate new treatment approaches aimed at slowing down the progression of the disease and improving outcomes for affected individuals. This may include experimental drugs targeting the underlying genetic mutation or pathways involved in progeria. Psychosocial Support: Living with progeria can present unique challenges for affected individuals and their families. Psychosocial support, including counseling and support groups, can help individuals and families cope with the emotional and psychological aspects of the condition and improve overall quality of life [14].
While there is currently no cure for progeria, these measures can help manage symptoms, reduce complications, and improve the overall well-being of individuals affected by the condition. Additionally, continued research and advancements in medical science offer hope for future treatments that may further slowdown the progression of progeria.
PRF Programs and Services
- International Patient Registry
- Diagnostic Testing Program
- Medical & Research
- Database Cell & Tissue Bank
- Progeria Family Network
- Research funding
- Scientific workshops
- Public awareness
- Volunteers & fundraising [13].
Conclusion
The term progeria applies to all diseases characterized by premature aging symptoms, it is often applied specifically in reference to Hutchinson-Gilford Progeria Syndrome. Progeria disease provides medical researchers a window to better understand how the body works and to explain some of the mysteries of the aging process [8, 19].
References
-
Mariados NF, Orio P, Schiffman Z, Van TJ, Engelman A, et al. (2023) Hyaluronic Acid Spacer for Hypofractionated Prostate Radiation Therapy. JAMA Oncology 9(4): 511- 518.
-
Wheaton K (2020) Hutchinson-Gilford Progeria Syndrome. National Library of Medicine.
-
Mendiratta G, Ke E, Aziz M, Liarakos D, Tong M, et al. (2021) Cancer Gene Mutation Frequencies for the U.S. Population. Nature Communications 12(1): 5961.
-
Batista N, Desai S, Perez AM, Finkelstein AL, Radigan R, et al. (2023) The Molecular and Cellular Basis of Hutchinson-Gilford Progeria Syndrome and Potential Treatments. Genes (Basel) 14(3): 602.
-
Gold NB, Adelson SM, Shah N, Williams S, Bick SL, et al. (2023) Perspectives of Rare Disease Experts on Newborn Genome Sequencing. JAMA Network Open 6(5): e2312231.
-
Harhouri K, Cau P, Casey F, Guedenon K, Doubaj Y, et al. (2022) MG132 Induces Progerin Clearance and Improves Disease Phenotypes in HGPS-like Patients’ Cells. Cells 11(4): 610.
-
Hayes DE, Rhee DW, Hisamoto K, Smith D, Ro R, et al. (2021) Two Cases of Acute Endocarditis Misdiagnosed as COVID‐19 Infection. Echocardiography 38(5): 798- 804.
-
Priyanka R, Ram BN, Kumar KP, Chayan B, Raju DK, et al. (2022) Optimal Parameter Allocation in Renewable Energy Sources Integrated Fast Charging EV Station considering hGPS Algorithm. Journal of Engineering Research 11(1A): 198.
-
Koblan LW, Erdos MR, Wilson C, Cabral WA, Levy JM, et al. (2020) In Vivo Base Editing Rescues Hutchinson-Gilford Progeria Syndrome in Mice. Nature 589(7843): 608-614.
-
Toni L, Dusatkova P, Novotna D, Zemkova D, Pruhova S, et al. (2019) Short Stature in a Boy with Atypical Progeria Syndrome due to LMNA c.433G>A [p.(Glu145Lys)]: Apparent Growth Hormone Deficiency but Poor Response to Growth Hormone Therapy. Journal of Pediatric Endocrinology and Metabolism 32(7): 775- 779.
-
Chatzifrangkeskou M, Dour CL, Muchir A (2023) Modulation of Cytoskeleton in Cardiomyopathy Caused by Mutation in LMNA Gene. American Journal of Physiology Cell Physiology 324(6): C1223-C1235.
-
Kalidas RM, Raja S, Mydeen SAKNM, Samuel S, Durairaj S, et al. (2015) Conserved Lamin A Protein Expression in Differentiated Cells in the Earthworm Eudrilus Eugeniae. Cell Biology International 39(9): 1036-1043.
-
Wong S (2016) Gene Change Should Prevent GM Escapees. New Scientist 229: 14.
-
Gordon L, Norris W, Hamren S, Goodson R, Clair J, et al. (2023) Plasma Progerin in Patients With Hutchinson- Gilford Progeria Syndrome: Immunoassay Development and Clinical Evaluation. Circulation 1479230: 1734- 1744.
-
Brown WT (2007) Progeria. In: KliegmanRM, et al. (Eds.). Nelson Textbook of pediatrics. 18th (Edn.), philadelphia, pa:Saunders Elsevier; chapter 90.
-
Keil L, Berisha F, Knappe D, Kubisch C, Shoukier M, et al. (2022) LMNA Mutation in a Family with a Strong History of Sudden Cardiac Death. Genes 13(2): 169.
-
http://www.ncbi.nlm.nih.gov/Pubmedhealth.
-
Gordon L, Tuminelli K, Andres V, Campisi J, Kieran M, et al. (2021) The Progeria Research Foundation 10th International Scientific Workshop; Researching Possibilities, ExTENding Lives-Webinar Version Scientific Summary. Aging (Albany NY) 13(6): 9143- 9151.
-
Lowery M (2015) Pharmacist Featured in HBO Documentary on Heroin Addiction.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City