First Impressions of the Bedside Nurse: A Grounded Theory Study
This study explored the first impressions of bedside nurses from the patient perspective, cultivating a grounded theory process. A qualitative grounded theory design emphasizing constructivist underpinnings was used. Individual interviews were conducted with 20 adult inpatients on Medical-Surgical units at a community hospital in the Midwestern United States. Five major themes emerged: 1) demeanor is the prevailing characteristic of the first impression 2) nonverbal communication is the most important influence in first impression formation, 3) first impressions are instantaneous, 4) first impressions spark the direction of the nurse-patient relationship, 5) first impressions are powerful. Findings reveal that first impressions of nurses have a significant impact on the nurse-patient relationship and the patient’s hospital experience. A unique conceptual model and process was created based on these findings, illustrating the significance of the first impression on the nurse-patient relationship and the patient’s perception of their care. Recognizing the influence of first impressions of nurses could provide a new innovative approach to impact the nurse-patient relationship, the patient’s experience and perceptions of their care, as well as patient satisfaction. First impressions are largely underestimated in nursing yet they have important implications for nurses, nurse educators, and nursing leadership.
Abbreviations
HCAHPS: Hospital Consumer Assessment of Healthcare Providers and Systems; LPN: Licensed Practical Nurse; RNs: Registered Nurses.
Introduction
In the constantly changing landscape of healthcare, patient perceptions of care and satisfaction have gained tremendous momentum over the last few decades. Recognizing that perceptions begin with first impressions is crucial to this discussion. According to Spitzberg BH [1], healthcare experiences and outcomes are related to first impressions of healthcare providers. Nurses are the cornerstone of healthcare making the nurse-patient relationship vitally important to a patient’s perception of their healthcare experience as it lays the foundation for therapeutic communication [2]. Patient perceptions about experiences with nurses are also very important influences of patient satisfaction and consumer decision to return [3]. Specifically, research suggests that nurse communication has an impact on overall patient satisfaction [4]. Patients’ perceptions of nursing care are directly connected to hospital reimbursement from the Centers for Medicare and Medicaid Services [3, 4]. Furthermore, the survey that measures patient satisfaction, the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) Survey, fuels incentive payments to hospitals that perform well, placing additional pressure on nurses to create positive perceptions for their patients [5].
The existing evidence about first impressions of nurses and the potential effects on patient perception of care is limited and conceptualized. The only study found that is specifically aimed at first impressions in nursing dates back to the 1990’s [6, 7]. However, the study focuses on physical appearance alone leading to perceptions and judgments about competency and professionalism [6, 7]. None of the studies currently found examine first impressions comprehensively. Furthermore, most studies found are quantitative and descriptive, survey-type in nature.
Appearance plays a major role in first impressions [8] including uniform, tattoos and piercings, and physical attributes. Numerous studies about perceptions of nursing image are based on the impact of uniform only, recognizing the influence of uniform on patient’s perceptions about nursing image [9], trust and competence [10, 11, 12]. Physical embellishments such as tattoos and piercings have also been investigated as a facet influencing patient perception of care, competency, anxiety, and comfort level [8], [13]. Aspects of physical appearance such as a smile are found to affect perceptions of personality, and promote trust and presence [14].
Recognizing that communication competence is paramount to developing healthcare relationships is well documented in the literature [1]. Nonverbal communication accounts for as much as 93% of the total impact of a message, with physical appearance being the most important nonverbal characteristic noted by listeners [15]. Facets of nonverbal communication have been discussed in multiple studies, including those mentioned previously about uniform and physical appearance. There is also evidence that shows that nonverbal communication affects perceptions of trust [1]. Additional research shows us that communication is also bioactive, meaning it could have an effect on another human being. Communication between nurses and patients creates neural firing, prompting the ability to create, change, and shape how the brain functions [16]. As nurses communicate with patients both verbally and nonverbally, they create a shared external environment that can lead to newly generated ideas and behaviors. Examples of this include studies about vaccines being found more effective when a positive mood is created at the time of administration [17], and positive communication and expression of emotions improving long- term cardiovascular risk [18].
Peplau’s Theory of Interpersonal Relations is the only nursing theory that identifies first impressions. Peplau’s work discusses three phases of the nurse-patient relationship: orientation, working, and resolution, and focuses on the transformative power of the nurse-patient relationship [19]. Peplau describes the relationship as key to the healing process [20], and identifies the first encounter as a key component of the orientation phase that influences the direction of the nurse-patient relationship, trust, and ultimately expectations of care [21]. However, the orientation phase of Peplau’s Theory is the most under-developed and least well understood, yet potentially the most impactful when discussing first impressions and the nurse-patient relationship. Our research aims to fill the gap with further knowledge about what the first impression means to the patient.
For the purposes of our research, the definition of first impression is adopted from Todorov A, et al. [22] “studies on first impressions are studies on judgments of strangers.” It would be remiss not to acknowledge the mutuality of the first impression, however the aims of this study focus on the viewpoint from the patient only.
Our study was designed to explore first impressions of the bedside nurse from the patient perspective. Specifically, the aims of this study were: 1) From the patient’s perspective and based on the patient’s experience, identify characteristics of the bedside nurse that are important in forming first impressions, and 2) Describe the influence and process of the first impression on the patient’s perception of nursing care received.
Methods
We used a grounded theory approach aimed to gain a full understanding of the interaction between the nurse and the patient at the time of the first impression. Individual, semi- structured, voluntary participant interviews were conducted using audio recordings to gather qualitative data about the first impression of the bedside nurse from the patient perspective.
Participants
We used convenience sampling to recruit inpatients on four traditional Medical-Surgical units at a moderate-sized community hospital in the Midwestern United States. The study’s inclusion criteria were that participants were 18 years of age or older, able to communicate in English, and able to provide informed consent. Patients were excluded if they had any neurological or psychological deficit or cognitive impairment, unable to provide informed consent, if they were in isolation, hospice or terminal care, pregnant, or a prisoner.
The recruitment process included a designated hospital representative from each of the Medical-Surgical units who conducted an initial screening of participants utilizing information available to them in the course of their normal workday, and referred potential participants to the PI by room number. The PI verified inclusion and exclusion criteria, met with the participant, provided an explanation of research, obtained consent, and conducted the interview.
Privacy and Ethical Considerations
Both the Institutional Research Board at the University of Central Florida and the healthcare organization where the study took place approved the study. The PI ensured that all interviews took place in the patient’s private room, and the nursing staff was not aware of who participated in the study. All participants were informed about the purpose, data, and confidentiality of the research using the explanation of research document, and a copy of the document was provided. Data was de-identified using a randomly assigned Please tell me about a time when you were in the hospital and had a nurse care for you who you had not seen before.
Please tell me about a time when you had the opposite impression than what we just discussed the first time you met a nurse.
Please describe for me how you know if someone is a good nurse?
- What does an ideal nurse look like?
- How quickly do you know if someone is a good nurse?
participant number and no names or health information were discussed or used throughout the study. Minimal demographic information was collected for descriptive purposes only. Participants were assured that their decision to participate would not influence the care they received, and that they could terminate the interview at any time for any reason.
Data Collection
Using a semi-structured interview guide Table 1, individual interviews were conducted to gain a comprehensive understanding of the patient’s experiences with first impressions of nurses and how that affected their feelings or their care. We also sought insight into how this initial impression of the bedside nurse influenced their feelings about the care they anticipated receiving. The interviews were conducted and recorded by the PI.
- What was that experience like when the nurse approached the bedside for the first time?
- What were you thinking when the nurse approached the bedside for the first time?
- What did you notice first?
- How would you describe your first impression?
- How did your first impression make you feel?
- How accurate was your first impression?
- What were you thinking when the nurse approached the bedside for the first time?
- What did you notice first?
- How would you describe your first impression?
- How did your first impression make you feel?
- How accurate was your first impression?
- •
- What additional information do you think is important for me to consider about first impressions in nursing or your relationship with nurses?
Table 1: Sample Interview Guide.
Data Analysis
The interviews were transcribed verbatim in a Microsoft Word document and verified for accuracy by the PI. Primary analysis consisted of complete reading of transcripts and notations of broad possible coding categories. Inductive grounded theory methods in thematic analysis using manual color-coding and constant comparison techniques following each interview served to identify and develop major themes as they emerged [23]. Weekly consultation with expert qualitative researchers assisted with analysis of data before proceeding to further interviews. A systematic open coding and thematic analysis approach followed by axial coding cultivated identification and development of major themes and a grounded theory process.
Rigor
Multiple strategies were implemented to ascertain rigor [24]. Pilot testing, member checking, and triangulation served to achieve credibility. Negative case inquiry and analysis was used with each participant. Drafts of preliminary models and findings were shared with participants who were asked to review the developing process and contribute any ideas about their experiences that were not already captured. Weekly meetings with two experienced, doctoral-prepared researchers assisted to review analytical thoughts and ideas for ongoing interviews. An audit trail was kept that included ongoing field notes and investigative thoughts, ideas and questions. The use of thick, rich, descriptive narrative data allows the reader to determine transferability. Attempts to mitigate researcher bias included ongoing journaling, reflection, and reflexivity.
Results
A total of 20 hospitalized adults participated in this study, 11 females and 9 males. The participants ranged in age from 44-80 years old, with the average participant age being 61. The majority of participants, 80%, identified as white (n=16), while 20% identified as African Americans (n=4). All but one of the participants (n=19) had a High School/GED or higher level of education. Among them, six individuals (30%) were college educated. The sample included a wide variety of employment backgrounds including retail, truck driving, education, restaurant serving, sales, and one participant was a licensed practical nurse (LPN). Only 3 (15%) of the participants worked in healthcare, and none were Registered Nurses (RNs). Interviews continued until the aims of the study were met, and the average interview was just a little more than 20 minutes.
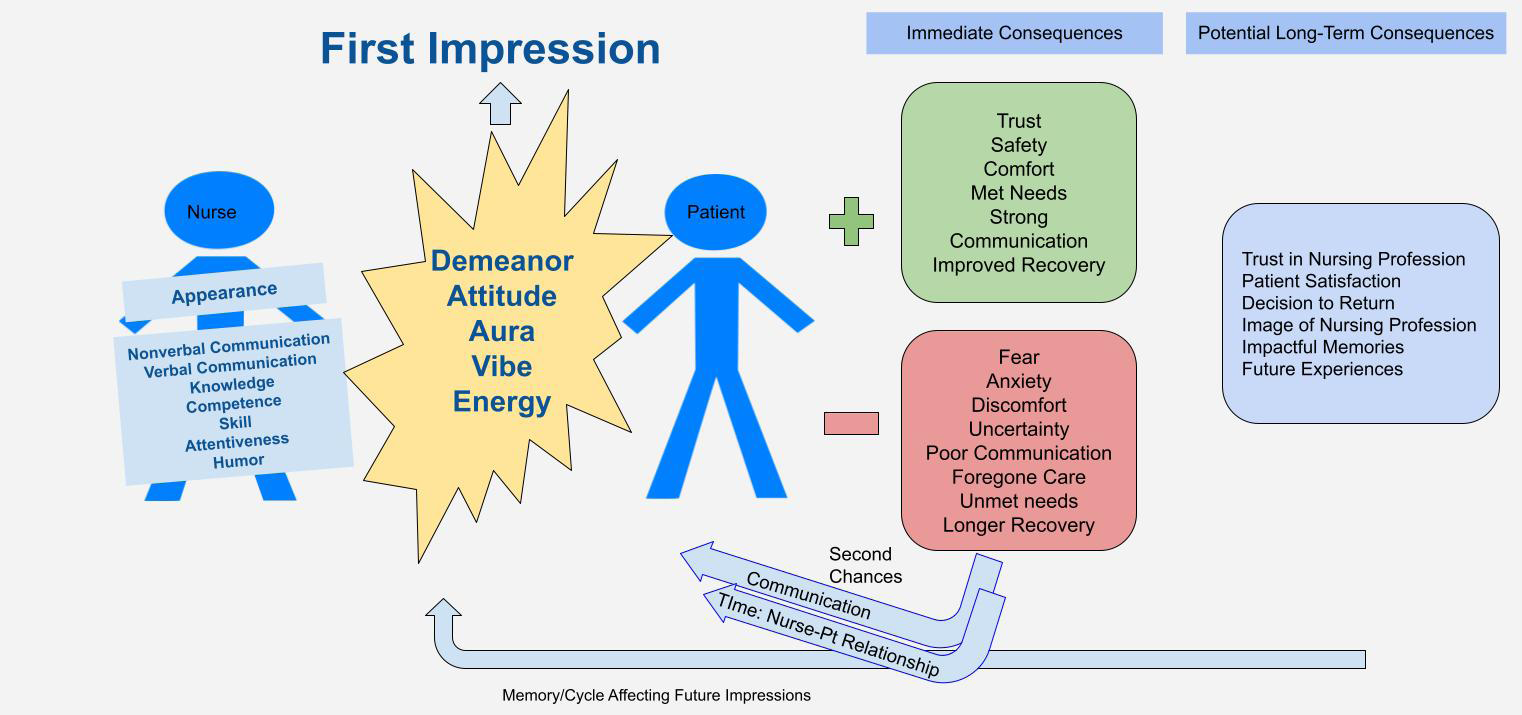
The results of our study identified a distinct process and grounded theory of first impressions of the bedside nurse from the patient perspective (Figure 1). Five major themes emerged from the data. Supplemental Table 2 is included with additional data related to major themes and accompanying quotes. The findings indicated the process began when the patient formed an immediate perception of the nurse’s demeanor and sensed their energy or vibe as soon as the nurse entered the room, often before the nurse reached the bedside and before any verbal communication had taken place. For some patients, this impression occurred as the nurse walked through the door. The nurse’s demeanor set the tone of the interaction, sparked the nurse-patient relationship, and consequently triggered the patient’s expectations of care, either positively or negatively. Patients described many possible outcomes stemming from the initial “vibe” perceived. Some of the outcomes were short- term including fear, trust, anxiety and unmet or foregone needs. Other outcomes described were long-term, including the patient’s perceptions about the nursing profession, satisfaction with the hospital experience, and the patient’s decision to return to that hospital for care. Participants shared very vivid and emotional experiences indicating that the first impression of the bedside nurse was a profoundly impactful moment that set the tone for the nurse-patient relationship.
Major Themes Exemplary Quotes
Demeanor: The prevailing characteristic of the first impression of the nurse identified by patients.
Nonverbal communication: Noted before verbal communication.
“You just get a vibe from somebody… You can just kind of tell their vibe…You know it’s gonna be good, you know” “The mood…. Makes you feel like you’re gonna get good treatment, for sure. You feel like you’re going to get good treatment.” “Because when they walk in it’s like…. It’s like they have that like…just that look like I’m here to help. You know, what can I do for you without saying a word.” “I guess if somebody come in and smile everything’s gonna be good. Because you know it means they’re happy with what they’re doing and that makes a difference.” “As soon as they come in you got that vibe down.” “I can tell if they’re a good nurse by the time they hit the curtain just by their attitude walking in.” “You have to be responsible with putting your care in somebody else’s hands. It’s best to try to cooperate, as much as possible. Make the process you know go easy you know like as much as possible because that’s going to determine the effort that you’re going to get out of your caregiver.” “When I showed kindness she showed kindness.”
- Nurse-Patient Relationship: First impressions spark the direction of the nurse patient relationship.
- “I just wish that it could just all be people like that, because I think you can get better faster.”
- “I couldn’t wait for her shift to be over. I would always try not to ask for anything. I would try not to, you know.”
- Impact & Consequences: First impressions are powerful and lead to important consequences.
Table 2: Supplemental Table of Findings.
Major Themes Revealed
Demeanor: Participants decisively emphasized demeanor as the most prominent characteristic of the first impression of the bedside nurse. Although demeanor is a facet of nonverbal communication, the significance warranted distinct recognition. While demeanor was the word used most often by participants, they also used other synonymous expressions such as vibe, aura, energy, personality, attitude, and mood. Participants described this as a feeling, indicating their senses played a role in their perception. For example, one patient stated: “There’s just an aura around them you can just sense… not see physically.” Another patient stated: “I believe it is so like the energy. The vibe that they’re giving off…it’s their behavior, their posture, you know, and their energy. .. just just just…. their demeanor.” Participants conveyed that the nurse’s demeanor played a pivotal role in setting the tone for their expectations about the nurse-patient relationship, both positively and negatively. One patient expressed: “It’s just their whole demeanor. It’s like, yeah this is gonna be a good day.” In another example, a participant described a nurse’s immediate “surly” attitude as “contagious”. Numerous patients reported that their initial perception of the nurse’s attitude significantly influenced their overall experience throughout the shift and their anticipation of the quality of care provided. A patient stated: “I can tell if they’re a good nurse by the time they hit the curtain by their attitude walking in.” Nonverbal Communication More Important than Verbal Communication: The findings of our study indicated that nonverbal communication, with a particular emphasis on demeanor, was the predominant factor influencing the first impression of the bedside nurse. Some of the other nonverbal influences that were highlighted in addition to demeanor included: physical appearance, identification badge, a smile, uniforms, caring behaviors, listening, attentiveness, and mannerism. Patients also noted the way a nurse physically approached the bedside influenced their perception of the nurse.
Physical appearance emerged as the second most prominent characteristic noted in the formation of the first impression. Specifically, patients identified neatness and hygiene as being important: “Just clean, you know overall- the hygiene. You know she’s on top of her game. You don’t want to look all rough now you’re gonna take care of me, umm because I’m already feeling and looking rough myself so you know, just nice appearance, and of course clean.” Personal physical characteristics, including weight, gender, hairstyle, tattoos, or piercings, were generally regarded by the patients as unimportant in the first impression. However, a few patients did mention noticing whether the nurse appeared to live a healthy or unhealthy lifestyle. One participant stated: “…it shows that they’re trying to live healthy also.” When asked, participants denied that a nurse’s ethnicity or cultural background had any impact on their perception of the first impression.
Other nonverbal points of discussion included uniform color and nametags. Patients’ expressed increased satisfaction with being able to recognize whom each caregiver was based on the color scrubs worn. A few participants described the name badge as being important in identifying the caregiver’s role as well as the patient’s expectations: “I’m looking for their name tag. And then I don’t really much care anymore because if they got hospital credentials and I can see them that’s usually good enough for me.” While some participants discussed the importance of a greeting and introduction, it was notably given less emphasis when compared to nonverbal influences. The role of verbal communication was acknowledged as contributing to the vibe and later nurse-patient relationship through further interactions, but its impact was primarily noted in further interactions only after the initial impression was established.
First Impressions are Formed Instantaneously: This study revealed that first impressions are formed immediately. All participants reported forming an initial perception or judgment about the nurse very quickly, often before the nurse reached the bedside and before any verbal interaction. One patient stated: “I can usually tell right away… Usually before they even say anything, like when they walk in the room…” A few of the participants described an initial impression occurring immediately, but added that additional formation continued over the next few minutes as they sensed and observed more about the nurse: “Umm I think I can pretty much judge how good a nurse is at the 75% correct level right when they walk in the room… by the time they walk out of the room, I’ve got the other 25%.” A single participant in the study was identified as an outlier, reporting that it took them approximately 1-2 hours to form an impression.
Nurse-Patient Relationship Begins with the First Impression: Patients shared feelings about sensing a connection with the first impression, triggering the nurse-patient relationship. Some patients referred to the manner in which the nurse gave care, emphasizing that their mannerisms contributed to building the nurse- patient relationship, further highlighting the significance of demeanor as a prevailing characteristic from the beginning and continuing throughout. Participants described that the nurse-patient relationship started with sensing a vibe or aura, and its progression was dependent on further interactions. Some patients also reported feeling that the relationship was mutual, and required them to make contributions as well. Patients shared feelings of vulnerability, stating they felt prompted to contribute to the relationship or else the nurse might “just do the bare minimum and provide average care”. One participant stated: “You get more bees with honey.”
Impact and Consequences
The last major theme revealed is that patients discussed first impressions of their bedside nurse having an impact on their stay, with either positive or negative consequences. One patient shared feelings of confidence based on their first impression: “I knew very quickly she was doing this because this is what she’s called to do. This is what she was meant to do and she loves what she does… it makes me feel confident in the care that I’m getting when she’s here.” When patients stated that they perceived the first impression as negative, they revealed that they would not use their call light, they would not communicate as they normally would, and they would forego their needs to avoid further interactions with the nurse, thus leading to a poor nurse- patient relationship. For example, a participant disclosed: “I didn’t want to ask her for nothing.” In addition, patients stated that if they had a positive relationship with the nurse they perceived that they received better care, which helped them to heal faster and have a speedier rate of recovery. One participant stated: “So I think that like, nurses can hold back your healing.” Patients also discussed perceptions about competency, both positive and negative, as an effect of the first impression. One participant shared her misperception about a nurse’s competencies based on the nurse’s tattoos and physical limitations, and how the nurse’s demeanor and skill changed her perception. This patient stated: “I’m a hard IV stick…and then they send this guy in… he had like, like the full tattoo arms and … like he had like, just these two um fingers. And like, when he started, once he started, I calmed down because the way he presented himself. So I felt bad. Because when I first looked at him, I was like, no. And then he got it on the first try.” Patients were able to recall momentous experiences even from long ago that continue to impact their perception of nurses and/or healthcare organizations. Multiple participants revealed that their choices for particular nurses, and decisions to return to a certain hospital were influenced by first impressions formed during past experiences.
Discussion
The findings from our study support the work of others in several ways, yet also offer a novel lens exclusive to nursing. Our findings support research indicating that the first impression is a dynamic, instantaneous interaction that leads to expectations of care, trust, and potentially patient satisfaction [7, 25, 26]. Outcomes from this study are congruent with research findings regarding nonverbal communication being more powerful than verbal communication [1, 15], as well as studies indicating inferences from facial appearances are very quick and intuitive [27]. Participants discussed the importance of consistent color-coded uniforms in identifying caregivers consistent with the work of Fogle C, et al. [12].
Participants generally denied that physical embellishments had any influence on their perception of their first impression. Results of this study support the work of Caldeira S, et al. [28] who noted tattoos are a primary form of communication that may actually build at trusting relationship, depending on the artwork. In this study, physical appearance was reported as generally not important in regard to culture, race, and background. However, they emphasized that cleanliness, neatness, and a generally healthy appearance were very important.
However, our study is unique in pointing out a major difference about first impressions related to nurses. Unlike previous studies, demeanor was discussed explicitly in our study. When asked about what an ideal nurse looks like, patients denied that there was such a person based on physical attributes and circled back to demeanor. Furthermore, demeanor influenced perceptions about the type of nurse the patient perceived the nurse to be. The identification of demeanor as the major influence of a first impression is new to the literature. Additionally, patients discussed senses and intuition related to first impression formation- an idea also not found in previous nursing studies. Perceived competency is a consequence of the first impression that should be strongly considered by the nursing profession, even if the perception proves incorrect as was shared in this study.
Participants resonated experiences that aligned with principles of bioactive communication and relationship building. The neural firing that occurs in the first few milliseconds has been shown to have bioactive outcomes in other studies previously discussed, hence the consequences noted in this study should also potentially be considered bioactive. Consequences such as fear, anxiety, and trust likely provoke strong bioactive neural patterns that point the patient in a direction of either positive or negative healing patterns. The pivotal moment of the first impression may serve as a decision point that is critical to the patient’s subsequent healing and health status. Based on the results of this study, this critical moment also serves as the defining moment for the nurse-patient relationship, thus creating bioactive effects for both the nurse and the patient. Feelings ensue for both parties that could affect health outcomes. The consequences of the first impression of the nurse are important in a different way in our study compared to other disciplines because human lives are at stake. If the patient perceives the first impression negatively, the remainder of the visit (including recovery and outcomes) could be influenced [6]. While some of the other studies about first impressions are healthcare based, none reveal that patients forego needs based on the initial interaction with a nurse. Withholding information from nurses has the potential to affect the patient’s health status, healing, and the patient’s satisfaction with care received.
We recognized a few limitations with our study. The major limitation is that only a single site was used. Despite the fact that the study was conducted at a single site with limited ethnic and cultural variability, 20 participants is believed to be an adequate sample size for a qualitative grounded theory study [29], data saturation was achieved, and meaningful data was obtained.
Conclusion
This study provides an innovative approach to improving patient’s perceptions and satisfaction. Based on the results of this study, nurses can intentionally plan for positive first impressions, aiming for positive relationships from the onset. Understanding the importance and the impact of the first impression from the patient perspective can help both nursing educators and nursing administrators raise awareness among nurses. If nurses are not mindful of the impact of the first impression, it remains instantaneous. By raising the cognizance of the first impression, nurses can practice making the first impression intentional. Our study serves to launch a trajectory of warranted research about first impressions in nursing. Based on our findings, further investigation about demeanor as a concept is needed. Additional research is suggested to assess education about first impressions among nursing faculty and students, as well as the first impression from the mutual standpoint of both the nurse and the patient. Bioactive communication as a concept remains largely unexplored in nursing science and warrants further study. The results of our study are also important to inform future research aimed at connecting first impressions directly to patient satisfaction scores. Long- term, the goal is ultimately to improve patients’ perceptions of their nursing care.
In summary, our study is a novel approach to exploring the meaning of the first impression of the bedside nurse from the patient perspective. Our study emphasizes that a nurse’s demeanor is vitally important to the first impression, nurse-patient relationship, patient satisfaction, and decision to return. Furthermore, the potential impact of the first impression of the nurse is highly under-recognized by nurses, nursing educators, and nurse administrators. Understanding the meaning and importance of the first impression from the patient perspective can be a huge asset to the nursing profession, whereas a lack of understanding poses great risk.
Disclosure Statement
The authors declare no conflict of interest.
Funding
There was no funding for this research.
References
-
Spitzberg BH (2013) (Re) Introducing Communication Competence to the Health Professions. J Public Health Res 2(3): e23.
-
Natalie C, Christopher R, Tanya P, Caryn W (2022) Nurses Hold the Key to Improving Outcomes for People who Present with Self-Harm. Australian Nursing and Midwifery Journal 27(8): 50.
-
Park S, Xu J, Smith FS, Otani K (2020) What Factors Affect Patient Perceptions on Their Hospital Experience?. Hosp Top 98(3): 127-134.
-
Trotta RL, Rao AD, McHugh MD, Yoho M, Cunningham RS (2020) Moving Beyond the Measure: Understanding Patients’ Experiences of Communication with Nurses. Res Nurs Health 43(6): 568-578.
-
Dempsey C, Reilly B, Buhlman N (2014) Improving the Patient Experience: Real-World Strategies for Engaging Nurses. J Nurs Adm 44(3): 142-151.
-
Mangum S, Garrison C, Lind C, Thackeray R, Wyatt M (1991) Perceptions of Nurses’ Uniforms. Image J Nurs Sch 23(2): 127-130.
-
Mangum S, Garrison C, Lind C, Hilton HG (1997) First Impressions of the Nurse and Nursing Care. J Nurs Care Qual 11(5): 39-47.
-
Nease B, Heaster SW, Cassada AM, Stowers C, Fisher G (2021) Patients’ Perceptions of Care Provided by Nurses with Visible Tattoos. Nurs Manage 52(3): 44-50.
-
Daigle A (2018) Professional Image and the Nursing Uniform. J Contin Educ Nurs 49(12): 555-557.
-
Kucuk L, Comez T, Kacar S, Sumeli F, Taskiran O (2015) Psychiatric Patients’ Perspective: Nursing Uniforms. Arch Psychiatr Nurs 29(6): 383-87.
-
Pawlowski P, Maxurek P, Zych M, Zun K, Dobrowolska B (2019) Nursing Dress Code and Perception of a Nurse by Patients. Nursing in the 21st Century 18(1): 60-67.
-
Fogle C, Reams P (2014) Taking a Uniform Approach to Nursing Attire. Nursing 44(6): 50-54.
-
Wildeman A, Reisdorfer E (2023) Client Perceptions of Healthcare Professionals (HCP) who have Visible Body Art: A Scoping Review. International Journal of Nursing Student Scholarship 10: 2291-6679.
-
Bladh ML, Leeuwen AMV (2017) Nurse-to-Patient Etiquette: It’s more than Good Manners. Nursing 47(8): 52-56.
-
Schuster PM, Philadelphia NL (2010) Communication for Nurses : How to Prevent Harmful Events and Promote Patient Safety. FA Davis.
-
Ivey AE, Daniels T (2016) Systematic Interviewing Microskills and Neuroscience: Developing Bridges between the Fields of Communication and Counseling Psychology. International Journal of Listening 30(3): 99- 119.
-
Ayling K, Fairclough L, Tighe P, Todd I, Halliday V, et al. (2018) Positive Mood on the Day of Influenza Vaccination Predicts Vaccine Effectiveness: A Prospective Observational Cohort Study. Brain Behav Immun 67: 314-323.
-
Haase CM, Holley SR, Bloch L, Verstaen A, Levenson RW (2016) Interpersonal Emotional Behaviours and Physical Health: A 20-Year Longitudinal Study of Long- Term Married Couples. Emotion 16(7): 965-977.
-
Peplau HE (1997) Peplau’s Theory of Interpersonal Relations. Nurs Sci Q 10(4): 162-167.
-
Sharma NP, Gupta V (2024) Therapeutic Communication. In: StatPearls [Internet], Treasure Island (FL): StatPearls.
-
Hagerty TA, Samuels W, Pala AN, Gigliotti E (2017) Peplau’s Theory of Interpersonal Relations: an Alternate Factor Structure for Patient Experience Data?. Nursing Science Quarterly 30(2): 160-167.
-
Todorov A, Porter JM (2014) Misleading First Impressions: Different for Different Facial Images of the Same Person. Psychological Science 25(7): 1404-1417.
-
Polit DF, Beck CT (2017) Nursing Research: Generating and Assessing Evidence for Nursing Practice. 10th (Edn.), Wolters Kluwer Health, Philadelphia pp: 784.
-
Morse JM (2015) Critical Analysis of Strategies for Determining Rigor in Qualitative Inquiry. Qual Health Res 25(9): 1212-1222.
-
Holtz BC (2014) From First Impression to Fairness Perception: Investigating the Impact of Initial Trustworthiness Beliefs. Personnel Psychology 68(3): 499-546.
-
Mattarozzi K, Colonnello V, Gioia FD, Todorov A (2017) I Care, Even After the First Impression: Facial Appearance- Based Evaluations in Healthcare Context. Social Science & Medicine 182: 68-72.
-
Grayling AC (2016) Judgement and Prejudice: A Fine Line. Prospect 239: 21.
-
Caldeira S, Lourenco M, Vidal T, Figueiredo AS (2017) Tattoo or No Tattoo? A Contemporary Ethical Issue in Nursing Education. Nurs Ethics 24(5): 626-628.
-
Creswell JW, Poth CN (2018) Qualitative Inquiry and Research Design: Choosing among Five Approaches. 4th (Edn.), Sage Publications, USA.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City