Micro Needling: A Review of the Literature, A Novel Treatment Strategy for Androgenetic Alopecia
The inherited condition known as androgenetic alopecia (AGA) causes hair to become thinner. In both men and women, it is the most prevalent kind of alopecia. Numerous therapy techniques have been researched in recent years, but only topical minoxidil and finasteride have received US Food and Drug Administration approval. A minimally invasive procedure called microneedling (MN) promotes the creation of growth factors, neovascularization, and collagen. In spite of MN hasn't been the subject of many studies in alopecia, but it's still a promising treatment therapeutic option, but there isn't a standardised strategy treating MN hair loss not yet proposed. The evidence available now is insufficient to provide a direct comparison with Despite showing potential to improve hair quality, thickness, and density in comparison to alternative treatments of hair, especially when used as a medication or in conjunction with other therapies delivery mechanism. The purpose of this article is to review the literature that is currently accessible on use of MN either by itself or in combination with other treatments to treat androgenetic alopecia.
Introduction
The most prevalent condition that causes hair loss in both sexes is androgenetic alopecia. It may happen to anybody at any age, mainly after puberty, with the prevalence rising with time. AGA is characterised by increasing hair follicle miniaturisation that results in terminal hair becoming vellus and causing pattern-specific hair loss [1, 2]. This illness is not only an aesthetic issue; it frequently affects patients’ quality life and is associated with a significant risk of feeling depressed, anxious, and even suicide [3, 4]. Inhibiting hair miniaturisation and stabilising hair loss are the two main goals of therapy for AGA [5, 6]. Although the United States Food and Drug Administration (FDA) has only approved finasteride and minoxidil as treatments for hair loss, other non-surgical treatments such as dutasteride, spironolactone, platelet-rich plasma (PRP), microneedling, and low-level laser therapy (LLLT) have also been used [7, 8]. A minimally invasive procedure called MN involves repeatedly puncturing the skin with sterilised microneedles [9, 10]. In 1995, Orentreich and Orentreich proposed the so- called “Subcutaneous incisionless (subcision) surgery” for skin depressions (wrinkles and scars), introducing the initial notion of MN [11]. Nearly two decades later, the first modern MN gadget was on the market [12]. Following these repeated microtraumas, the method is based on “collagen induction” [10]. Microneedling is thought to promote hair regeneration because the damage caused by the needling causes platelets and neutrophils to produce growth factors including TGF- alpha, TGF-beta, and platelet-derived growth factor (PDGF) [11]. Fibroblasts then contribute to the papillary dermis’ synthesis of collagen and elastin [13]. In particular when paired with other therapies, this method has been effective in treating hair loss [9, 10]. This review’s objective is to give a comprehensive overview of skin needling as an alternative therapy for AGA, whether it is used alone or in conjunction with other therapies.
Androgenetic alopecia is primarily driven by the hormonal imbalance of androgens, particularly dihydrotestosterone (DHT), and genetic predisposition. This condition leads to the progressive miniaturization of hair follicles, resulting in thinner and shorter hair until they cease to grow altogether. Conventional treatments, such as topical minoxidil and oral finasteride, have limitations in terms of efficacy and side effects. Hence, the quest for more advanced and efficient solutions has been ongoing.
The Promise of Nanotechnology
Nanotechnology, the manipulation of materials and structures at the nanoscale (1 to 100 nanometres), has shown immense promise in various fields, including medicine. In the context of androgenetic alopecia, nanotechnology offers several avenues for exploration: Enhanced Drug Delivery: Nanoparticles can be engineered to encapsulate hair growth-promoting agents, such as minoxidil or finasteride. These nanoparticles are so small that they can penetrate the scalp & barrier more effectively, delivering the active ingredients directly to hair follicles. This targeted approach reduces systemic exposure and minimizes side effects, enhancing the treatment & safety and efficacy. Sustained Release Systems: Nanoparticles can be designed to release their payload slowly and consistently over time. This sustained release system ensures a continuous supply of therapeutic agents to hair follicles, promoting longer- lasting and more consistent hair regrowth compared to conventional treatments. Improved Bioavailability: Nanotechnology can increase the solubility and bioavailability of active ingredients. This means that lower doses of drugs can be used, reducing the risk of adverse effects while maintaining or even improving therapeutic outcomes. Nutrient Delivery: Nutrient deficiencies are often associated with hair loss. Nanotechnology can facilitate the delivery of essential nutrients, vitamins, and minerals directly to hair follicles, promoting healthier hair growth from the root. Stem Cell Therapy: Nanotechnology enables the precise manipulation and delivery of stem cells to damaged hair follicles. Stem cell-based therapies hold significant potential for hair regeneration by rejuvenating and repairing miniaturized follicles. Diagnostic Tools: Nanosensors and nanomaterials can be employed for the early detection of androgenetic alopecia. These tools can provide valuable insights into the progression of the condition, enabling timely intervention.
Microneedle Devices and Types
Microneedles, which typically have a length of 25 to 2000 m, are tiny needles that may be used to puncture the corneum layer of the skin and distribute medications through tiny channels [14]. Microneedles are able to penetrate the skin 70 to 200 mm deep. The two main devices, the Dermaroller (Dermaroller Deutschland GmbH, Wolfenbuettel, Germany) [11] and the Dermapen (Dermapen, Salt Lake City, UT), are where the majority of MN devices are derived from. The first is a 12-cm long portable device made up of a cylindrical roller with 192 tiny needles arranged in 8 rows and 24 circular arrays [13]. The needles are typically constructed of silicon or medical-grade stainless steel using reactive ion etching processes, and they range in size from 0.5 to 3 mm in length and 0.1 to 0.25 mm in diameter. Nearly 250 holes per cm2 are produced in the papillary dermis when 2-mm long and 0.07-mm large microneedles are used 15 times on the same location [15]. There were also variants made specifically for home usage, including the Beauty Mouse (Dermaroller Deutschland GmbH).10 A “pen-like” electrically driven handling device with 9 to 12 needles and two speed settings (high: 700 cycles/min; low: 412/min) is known as a “Dermapen” [10, 16].
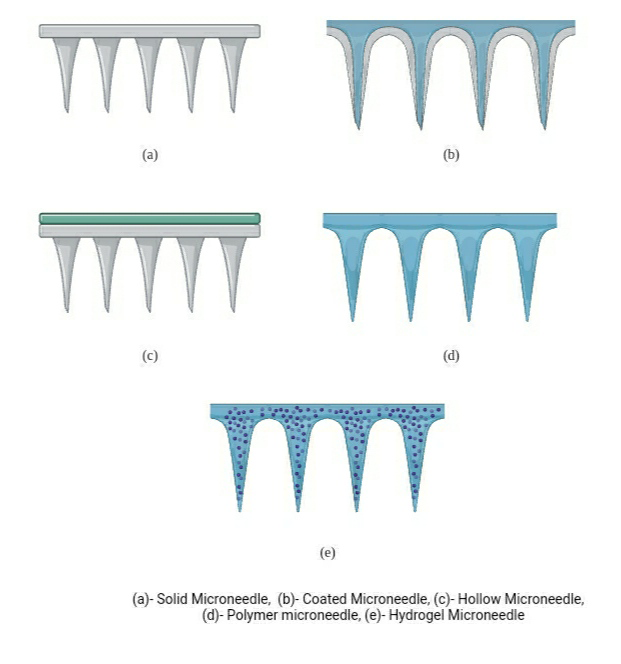
Recent innovations in MN integrate mechanical puncturing with other modern technologies. For instance, in fractional radiofrequency MN (FRM), radiofrequency is released from the tip of the needle, altering the structure of the dermal components. Others combine dermal serum infusion and microdermabrasion with light-emitting diode (LED) light (DermaFrac, Genesis Biosystems, Lewisville, TX), or LED light alone (LED MN devices). Last but not least, MN has also been employed as a transdermal delivery system for topical medications as they may be injected into the skin after skin puncturing or using hollow needles. According on the kind of microneedle used, many methods of drug delivery have been developed: solid ones for the “poke and patch” method, coated solid ones for the “coat and poke” method, polymeric microneedles for the “poke and release” method, and hollow ones for the “poke and flow” method (Table 1; Figures 1 & 2).
| Type of Microneedles | Advantages | Disadvantages | |
|---|---|---|---|
| 1 | Solid | Mechanical strength Physical stability Reasonable drug loading | Poor dose accuracy Potential for infection due to reuse |
| 2 | Coated | Mechanical strength | Peeling during insertion Poor biocompatibility Dose limitation |
| 3 | Dissolving | Low cost manufacturing Easy of manufacturing One step application | Poor Mechanical strength, physical stability and biocompatibility |
| 4 | Hollow | Dose accuracy Reasonable drug loading | Clogging Requirement of prefilled syringe Poor Mechanical strength Poor biocompatibility Potential for infection due to reuse |
| 5 | Hydrdrogel- foaming | Easy to manufacture Controlled drug release profile Reasonable drug loading | Poor Mechanical strength and physical stability Ingressing body fluid |
Table 1: Microneedles with their advantages and disadvantages.
Alopecia’s Microneedling Procedure
Depending on the doctor’s experience and skill, the surgery usually takes within 10 and 25 minutes. The following procedure is often used for Norwood Hamilton 5 to 7 alopecia or patchy alopecia. Usually 15 to 45 minutes before the procedure, a topical anaesthetic cream with lidocaine and prilocaine/tetracaine is given [17]. The region should be cleansed with an ethanol or beta-dine solutions for aseptic purposes once the anaesthetic cream has taken effect. You may use a pen or a roller. If a pen is employed, the needles should be set at the appropriate level. Lifting the pen after each linear pass should be used to treat the region. The same region may be passed over three times. If a roller is utilised, the doctor should move between 15 and 20 times in vertical, horizontal, and diagonal passes over the treated region. Minimal erythema or pinpoint bleeding are the preferred endpoints.
A topical antibiotic should be used following blood wash- off with saline solution. If treated together with minoxidil, the patient is advised to wait 24 hours before administering a topical treatment that promotes hair growth once the operation is complete [18]. The process can be repeated every two to four weeks [17]. The aforementioned method, however, is not recommended for patients with other types of alopecia or long-haired female patients of Ludwig 1 FPHL. Since no standardised technique has been established as of yet, therapeutic success may be hampered [18].
The anticipated erythema or pinpoint bleeding, seborrheic dermatitis, itching, infections, granulomatous responses, or lymph node enlargement are the most frequent adverse effects.
Case Studies and Advances
Several studies and developments highlight the transformative potential of nanotechnology in androgenetic alopecia treatment:
Nanoparticle-Encapsulated Minoxidil: Researchers have successfully encapsulated minoxidil within biocompatible nanoparticles. This approach enhances drug penetration and maintains a sustained release, resulting in improved hair regrowth rates and reduced side effects.
Dermal Nanopatches: Nanopatches containing hair growth- promoting agents can be applied directly to the scalp. These patches adhere to the skin, ensuring precise drug delivery to the targeted areas, simplifying the application process, and enhancing patient compliance.
Nanotechnology in Hair Transplantation: Nanoscale
materials have been employed in hair transplantation procedures to optimize graft survival rates and improve the overall outcome of the surgery. Nanotechnology contributes to better wound healing and reduced scarring.
Challenges and Future Prospects While nanotechnology holds immense promise, its integration into androgenetic alopecia.
Treatment is Not Without Challenges
Safety Concerns: The long-term safety of nanomaterials and nanoparticles must be thoroughly studied to ensure they do not pose health risks.
Regulatory Approval: Developing and gaining regulatory approval for nanotechnology-based treatments is a complex and time-consuming process.
Cost and Accessibility: Nanotechnology-based treatments may initially be costly and less accessible to all patients.
Individual Variability: Response to nanotechnology-based treatments may vary among individuals, necessitating personalized approaches.
Microneedling for Pattern Hair Loss
When treating AGA, microneedling has been used alone, 20 with saline solution, as a medication delivery method with minoxidil or with growth factors and PRP [19, 20, 21, 22, 23, 24].
Microneedling: In 2020, Starace, et al. [10] included 50 patients, including 14 men with AGA and 36 females (30 with AGA and 8 with telogen effluvium) [20]. Over the course of six months, three microneedling procedures with a four-week break between them were performed. All patients reported less hair loss, improved hair density, and thicker hair shafts after the six-month mark. Vertex median density improved by 35.1%, while frontal median density increased by 36.64% across the board for all patients. The medium hair diameter grew in the frontal and vertex regions (9.75% and 9.08%, respectively), but the vellus relative change decreased in both regions.
Microneedling and Minoxidil: In a research conducted by Dhurat and colleagues, the use of microneedling together with minoxidil cream on males with mild to moderate (Norwood- Hamilton III vertex or IV grade) AGA was examined [23]. For a period of 12 weeks, 94 patients were randomly assigned to receive either weekly microneedling together with twice- daily 1 ml 5% minoxidil lotion (treatment group) or only minoxidil lotion itself (1 ml, 5%, twice-daily; control group). The 1.5 mm-needles dermaroller was used on the scalp, which had previously had betadine and normal saline solution treatment, as part of the microneedling protocol, following several movement trajectories (longitudinal, vertical, and diagonal) until the skin began to display moderate erythema [23]. It was advised against using topical minoxidil the day of microneedling and for 24 hours thereafter. Hair counts, patient and researcher assessments, and other effectiveness outcomes all revealed statistically significant superior results for the therapy group. The mean change in hair count at week 12 was the most eye-catching statistic, with patients who had microneedling having 91.4 vs. 22.2 in the control group.
Microneedling+Growth Factors and PRP: In a grade I of Ludwig, et al. revealed the findings of a research on women who had female pattern hair loss (FPHL). The 11 participants had Growth Factor Solution (SGF57; Mediway, Seoul, Korea) applied to one side of their scalps and plain normal saline applied to the other. Following that, microneedling was used to treat both sides for a total of five times each week. The nine 33-G microneedles had a speed of 1500 rpm and could penetrate to a depth of 0.5 mm. The authors observed variations in the hair shafts on the two sides, with a statistically significant rise of more than 10% on the treated side from week two to week five. Additionally, there was an increase in patient satisfaction for the treated side but not for the control. There were no negative effects noted. Other later research concentrated on the use of microneedling and platelet-rich plasma (PRP) [24]. Platelet-derived growth factors are generated from active platelets and combined with calcium chloride or thrombin before or after PRP injection to create PRP [25] (Figure 3).
Conclusion
Microneedling has several benefits; it is a quick, simple, and affordable technique. Topical anaesthesia can be used to do it with minimum discomfort, allowing patients to carry on with their daily activities.
Nanotechnology is poised to revolutionize the treatment of androgenetic alopecia by offering targeted, efficient, and safe solutions. The enhanced drug delivery, sustained release systems, and nutrient delivery systems offered by nanotechnology hold the potential to provide long- lasting results for individuals suffering from hair loss. While challenges exist, ongoing research and development efforts are likely to pave the way for innovative and effective nanotechnology-based therapies for androgenetic alopecia.
As this technology continues to advance, a future where baldness is no longer an irreversible condition may be on the horizon, bringing hope to those in search of a permanent solution for their hair loss woes. Additionally, MN can be used with other treatments or medications and when paired with minoxidil, growth factors, or PRP, it has been shown to be helpful for individuals with AGA. Patients who have not responded to prior treatments or may not wish to use systemic medications can benefit from MN.
MN was successful in producing outcomes that may supplement or, in some circumstances, even completely replace more intrusive or time-consuming therapy regimens with few or no adverse effects.
Future research should take into account a number of factors. While there is no set standard for needle length, it should be long enough to pierce the skin’s barrier in order to enhance medication delivery or stimulation while being brief enough to cause little discomfort and skin damage.
Studies employing shorter needles often produced less encouraging findings than those using longer ones. To identify a standard methodology, including frequency of therapy, depth of penetration, and best time for medication administration following MN, more qualitative randomised controlled trials with a bigger sample population should be conducted.
References
-
Orentreich D, Orentreich N (1995) Subcutaneous Incisionless (Subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg 21(6): 543-549.
-
Fernandes D (2005) Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am 17(1): 51-63.
-
Doddaballapur S (2009) Microneedling with dermaroller. J Cutan Aesthet Surg 2(2): 110-111.
-
Ma G, Microneedle WC (2017) Bio-microneedle and bio- inspired microneedle: a review. J Control Release 251: 11-23.
-
Singh A, Yadav S (2016) Microneedling: advances and widening horizons. Indian Dermatol Online J 7(4): 244- 254.
-
Arora S, Bhandaree GP (2012) Automated microneedling device - a new tool in dermatologist’s kit—a review. J Pakistan Assoc Dermatol 22: 354-357.
-
Alster TS, Graham PM (2018) Microneedling: a review and practical guide. Dermatol Surg 44(3): 397-404.
-
Fertig RM, Gamret AC, Cervantes J, Tosti A (2018) Microneedling for the treatment of hair loss?. J Eur Acad Dermatol Venereol 32(4): 564-569.
-
Bao L, Gong L, Guo M, Taoming Liu, Anyu Shi, et al. (2020) Randomized trial of electrodynamic microneedle combined with 5% minoxidil topical solution for the treatment of Chinese male Androgenetic alopecia. J Cosmet Laser Ther 22(1): 1-7.
-
Starace M, Alessandrini A, Brandi N, Piraccini BM (2020) Preliminary results of the use of scalp microneedling in different types of alopecia. J Cosmet Dermatol 19(3): 646-650.
-
Dhurat R, Sukesh M (2015) Response to microneedling treatment in men with androgenetic alopecia who failed to respond to conventional therapy. Indian J Dermatol 60(3): 260-263.
-
Nilforooshzadeh MA, Lotfi E, Heidari Kharaji M, Zolghadr S, Mansouri P (2020) Effective combination therapy with high concentration of Minoxidil and Carboxygas in resistant Androgenetic alopecia: report of nine cases. J Cosmet Dermatol 19(11): 295-2957.
-
Dhurat R, Sukesh M, Ganesh A, Ameet D, Anjali P, et al. (2013) A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. Int J Trichology 5(1): 6-11.
-
Yu AJ, Luo YJ, Xu XG, Bao LL, Tian T, et al. (2018) A pilot split-scalp study of combined fractional radiofrequency microneedling and 5% topical minoxidil in treating male pattern hair loss. Clin Exp Dermatol 43(7): 775-781.
-
Farid CI, Abdelmaksoud RA (2016) Platelet-rich plasma microneedling versus 5% topical minoxidil in the treatment of patterned hair loss. J Egypt Women’s Dermatol Soc 13(1): 29-36.
-
Kanti V, Messenger A, Dobos G, Reygagne P, Finner A, et al. (2018) S3—European Dermatology Forum Guideline for the Treatment of Androgenetic Alopecia in Women and in Men. European Dermatology Forum pp: 1-59.
-
Sinclair R, Torkamani N, Jones L (2015) Androgenetic alopecia: new insights into the pathogenesis and mechanism of hair loss. F1000Res 4: 585.
-
Saed S, Ibrahim O, Bergfeld WF (2017) Hair camouflage: a comprehensive review. Int J Womens Dermatol 3(1): 75-80.
-
Alfonso M, Richter Appelt H, Tosti A, Viera MS, García M (2015) The psychosocial impact of hair loss among men: a multinational European study. Curr Med Res Opin 21(11): 1829-1836.
-
Manabe M, Tsuboi R, Itami S, Shin-Ichi Osada, Yasuyuki Amoh, et al. (2018) Guidelines for the diagnosis and treatment of male-pattern and female-pattern hair loss, 2017 version. J Dermatol 45(9): 1031-1043.
-
Gupta AK, Mays RR, Dotzert MS, Versteeg SG, Shear NH, et al. (2018) Efficacy of non-surgical treatments for androgenetic alopecia: a systematic review and network meta-analysis. J Eur Acad Dermatol Venereol 32(12): 2112-2125.
-
Mori O, Uno H (1990) The effect of topical minoxidil on hair follicular cycles of rats. J Dermatol 17(5): 276-281.
-
Rittmaster R (1994) Finasteride. N Engl J Med 330(2): 120-125.
-
Nazarian RS, Farberg AS, Hashim PW, Goldenberg G (2019) Nonsurgical hair restoration treatment. Cutis 104: 17-24.
-
Iriarte C, Awosika O, Rengifo Pardo M, Ehrlich A (2017) Review of applications of microneedling in dermatology. Clin Cosmet Investig Dermatol 10: 289-298.
- Solution-Processed Chiral Perovskites for Biomedical Applications
- Nanotechnology in Health Chemistry and Medicine: Current Challenges and Future Directions
- Human Exposure to Micro- and Nanoplastics: Pathways, Toxicity, and Intervention Strategies
- Exosome Nanomedicine for Cancer Therapy
- Micro and Nanoplastics–Plastisphere, Biotoxicity, Impact on Human Health, and Mitigation Strategies
- Process Validation of Cefixime Powder for Suspension Dosage Form, 50 mL