A Brief Conceptual Approach to Inner Ear Drug Delivery System
The inner ear, a delicate and intricate organ responsible for auditory and vestibular functions, poses unique challenges for drug delivery due to its isolation and complex anatomy. This paper provides a concise overview of a conceptual approach to inner ear drug delivery systems, exploring the current landscape and emerging technologies in this specialized field. We delve into the anatomical and physiological considerations that influence drug delivery to the inner ear and discuss various strategies to overcome barriers, including the blood-labyrinth barrier. Furthermore, the review highlights recent advancements in nanotechnology, targeted drug delivery, and innovative formulations designed to optimize therapeutic outcomes while minimizing systemic side effects. By understanding the nuances of inner ear drug delivery, this conceptual approach aims to contribute to the development of novel strategies that hold promise for improved treatments of inner ear disorders, fostering advancements in auditory and vestibular healthcare.
Introduction
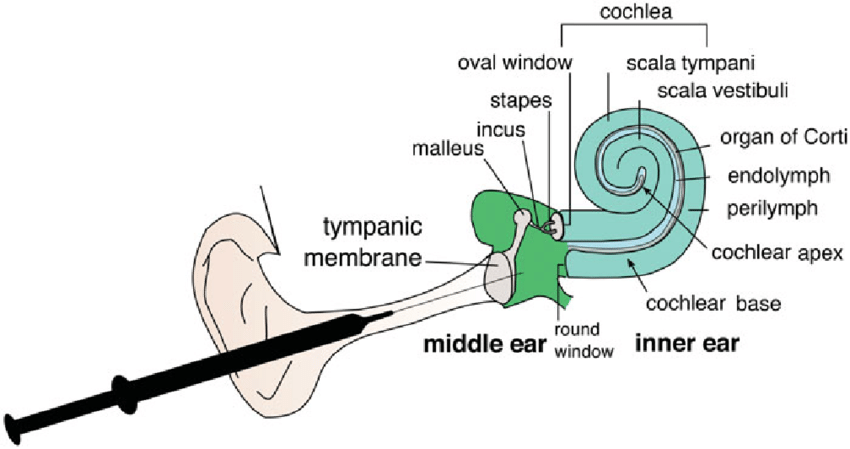
The factors like, environmental pollution, increasingly aging population, overexposure to noise in the youth and exposure to ototoxic but lifesaving drugs such as amino glycoside antibiotics and platinum-based chemotherapy, amplifying the spreading of hearing loss disability [1]. Inner ear drug delivery has been a challenge to physicians in the treatment of inner ear disorders. In the past few decades, new biomaterials and drug delivery technologies have been developed for inner ear delivery [2]. In last two decades, huge progress had been achieved in understanding and underlying mechanisms of hearing loss at the cellular and molecular level. A number of favourable attempts toward hearing restoration are focusing in establishing regeneration of the cells and cochlear nerve endings. The objective of the current chapter is to provide an updated general overview of inner ear drug delivery and discussing their potential in recent advances in biomaterials, bio-technological methods and delivery technologies [3]. Figure 1 indicates the anatomy of inner ear.
Administration Routes for Inner Ear Drug Delivery
Systemic Route: Usually, drugs are delivered to the inner ear via the systemic route, but only a few drugs can reach the target site of action at therapeutic concentrations in the inner ear because of the presence of BLB (Blood Labyrinth Barrier) is a major barrier separating the inner ear from systemic circulation with tight junctions, made up of capillary endothelial cells that line blood vessels located in the stria vascularis) [4]. In order to achieve therapeutic levels of drugs in the inner ear high systemic doses are required, which are often associated with undesirable side effects. Such systemic toxicities and side effects can range from minor nuisances to potentially life- threatening situations. Despite these adverse effects, systemic delivery through oral, intravenous, and intramuscular routes is still considered as the most convenient method of drug administration to the inner ear and is currently accepted as the first line approach in the treatment of inner ear disorders [5]. Intra-Tympanic Route: The topic of treating inner-ear disorders by local drug delivery has attracted considerable interest [6]. Intra tympanic delivery to the inner ear was performed via the injection or perfusion of the drug to the middle ear with the aim of drug diffusion through the RWM (Round Window Membrane which is a soft tissue barrier separating the middle ear from the inner ear) into the inner ear [7]. This route of drug delivery was introduced more than half a century ago for the treatment of Meniere’s disease (it is a disorder of the inner ear that can lead to dizzy spells and hearing loss) with local anaesthetics and antibiotics and has been widely used in clinics since 1990s [8]. This approach possesses several advantages over systemic drug delivery as this local drug delivery method can bypass the BLB, and therefore result in higher drug concentrations in the inner ear fluids and avoid undesired systemic exposure. Effective drug delivery to the inner ear via the intra-tympanic route also relies on the contact time of the drug solution (or drug delivery system) with the RWM. Unfortunately, large portions of the administered drugs are usually eliminated through the Eustachian tube following intra tympanic drug delivery [9]. There have been efforts to overcome this limitation through the development of devices and sustained-release drug delivery systems. Intra-Cochlear Route: Like intra-tympanic delivery, the intra-cochlear delivery approach provides an alternative to systemic drug delivery to the inner ear [10]. Direct intra- cochlear drug delivery can bypass the middle ear and allow drugs to get to their intended sites directly. Intra-cochlear delivery can substantially increase drug bioavailability in the inner ear and has the highest efficiency among the inner ear delivery methods discussed in this review [11]. Numerous intra-cochlear delivery technologies are being developed to improve the efficiency of drug delivery to the inner ear [12].
They include direct injections, cochlear implants, osmotic mini-pumps, as well as reciprocating perfusion Objectives of drug application in combination with drug- device combination [13, 14].
- Bypassing of the blood–brain barrier (the target organ is directly reached)
- Higher drug concentration in the inner ear
- Avoiding “first-pass” effects
- Reduction of adverse systemic effects
- Lower drug doses are necessary
- General reduction of insertion trauma
- Reduction of immune reaction
- Reduction of infection
- Reduction of loss of auditory neurons and spiral ganglion cells
- Reduction of fibrosis and ossification
- Reduction of stimulation of non-auditory neural structures
- Reduction of channel interaction
Drug Delivery Technologies for Inner Ears
Cannula-Based Delivery Systems: Several cannula-based delivery systems are available commercially for sustained delivery of drugs to the middle ear. These devices include Silverstein Microwick and Round Window Microcatheter. Potential problems and adverse effects of these devices include the persistent perforation of the tympanic membrane, risk of infection in the middle ear or external ear, and tissue growth in the middle ear either in the form of fibrosis or epithelial in growth leading to cholesteatoma [15]. Hydrogels: The biodegradable gelatine polymer named Gelfoams was first introduced in the surgery of inner ear. The Gelfoams when soaked in gentamicin and placed on RWM proved to give improved outcome in the treatment Meniere’s disease as it is helpful to eliminate vertigo and tinnitus in 75% and 48% patints respectively. . In another study, Gelfoam infiltrated with brain-derived neurotrophic factor (BDNF) on to the RWM of deafened guinea pigs and evaluated the effect of this treatment by structural and functional measures. In the 2weeks of Gel- foams BDNF treatment ,survival of spiral ganglion neurons (SGNs) in the inner ear was observed in the low turn of the cochlea, but no significant improvement was observed in the apical turn of the cochlea, probably due to the small amount of drug reaching the apical turn. This suggests that local delivery of BDNF using Gelfoams can protect the parts of the spiral ganglion neurons (SGNs) of cochlea [16]. Stabilizing Matrices: The stabilizing matrices possesses several benefits on middle ear perfusions. Unless using stabilizing matrices the drugs delivered to the middle ear got dispel out either by the absorption through the mucosal layer of middle ear or by drainage by the Eustachian tube. It’s a great matter of concern while using toxic agents for targeting them to the targeted tissues which allows superior control of dosing profiles suggests future trans-tympanic delivery methodologies and gives focus on sustained release by using various techniques utilizing stabilizing gel matrices. A good example is Chitosan-glycerophosphate hydrogel, which is liquid at room temperature and a biodegradable gel at body temperature allows the drug to come in contact between the matrix and membrane of the inner ear i.e. round window membrane. The above material has successfully delivered dexamethasone to the inner ear through round widow membrane which has been proved by various studies carried out in mice [17]. Cochlear Implants: Intra-cochlear drug delivery has greater efficacy in comparision to cochlear implants in persons with deafness. Hearing can be restored by direct scala tympani delivery of dexamethasone for eight days which has loss due to insertion of electrode in the guinea pig...) (basal turn, scala tympani with The brain-derived neurotrophic factor and fibroblast growth factor were infused into the guinea pig cochlea (basal turn, scala tympani) following deafening via a systemic amino glycoside and diuretic treatment. Both spiral ganglion neurons and peripheral process re growth were enhanced with the treatment. The inclusion of fluidic channels within cochlear implant electrode provides the opportunity to chronically infuse neurotrophic factors and pharmacological agents to enhance efficacy of cochlear implants. Scientists describes a drug delivery system integrated into a scala tympani electrode which has designed for use in guinea pigs with demonstrated delivery of neomycin [18]. Nano Particles: The delivery system of super paramagnetic iron oxide nano particles (SPIONs) through a three cellular layers RWM model in vitro showed that SPIONs distributed throughout the model membranes under an external magnetic field. In another study it has been investigated that the capability of ferro gel which consist of SPIONs and Pluronic with an imaging tag for the delivery of many therapeutic agents across the RWM of human temporal bones as well as in organo- typic explants cultures of rat’s inner ears [19]. It has been found that the SPIONs were in the cytoplasmin organ which is suggesting that the nanoparticle system can be a suitable for cell targeted drug delivery system which prevents drug degradation in the cellendo lysosomal compartment. Some researchers has been showed that the cell targeting ability and toxicity of nerve growth factor-derived ligand functionalized with specific polymers and omenano- particles for specific cell targeting to SGNs in mouse cochlear organo typic culture and observed specific drug targeting various tissues [20]. Stem Cell Therapy: The hearing loss can be restored by using the stem cell therapy, which has the potential to protect the hair cells and spiral ganglion neurons (SLNs).The stem cell therapy has been proved to be a prominent method to treat the inner ear disorders by replacing hair cells. It has been also suggested that the implantation of embriyonic stem cells, foetal root ganglions and otocyst cells in the inner ear to restore the damaged hair cells [21].
Limitations To Intratympanic Route and Intracochlear Route
Limited Drug Distribution: The distribution of drugs within the cochlea is not uniform, leading to uneven drug levels in different regions of the inner ear. Diffusion from the middle ear to the cochlea is hindered by anatomical barriers, such as the round window membrane [3]. Variable Absorption: Absorption of drugs through the round window membrane can vary among individuals, affecting the efficacy and consistency of drug delivery [5]. Tympanic Membrane Permeability: The permeability of the tympanic membrane can limit the amount of drug that can pass through, affecting the overall drug delivery efficiency. Patient Compliance: Intratympanic drug delivery often requires multiple administrations, and patient compliance can be challenging, affecting the effectiveness of the treatment. Risk of Middle Ear Infection: Repeated injections can increase the risk of middle ear infections, which may limit the frequency of intratympanic drug administrations [7].
Intracochlear Route
Invasive Nature: Intracochlear drug delivery methods often involve invasive procedures, such as cochlear implantation or direct injection, which can pose risks and complications. Tissue Damage: Invasive procedures may cause tissue damage or inflammation, potentially leading to adverse effects on hearing function. Limited Drug Residence Time: Rapid clearance of drugs from the cochlea can limit the time during which therapeutic concentrations are maintained [8]. Risk of Infection: Invasive procedures increase the risk of infection, which can have serious consequences in the delicate structures of the inner ear. Difficulty in Targeting Specific Cells: Achieving precise targeting of specific cells within the cochlea is challenging, and non-specific drug distribution may lead to suboptimal therapeutic outcomes. Biocompatibility Issues: Some drug delivery materials or devices may pose biocompatibility concerns, leading to tissue reactions or inflammatory responses [9].
Conclusion
Hearing loss represents one of the most prevalent unmet needs in all of medicine, and bringing new treatments to market will require concerted advances along multiple fronts, due to the major challenges presented by the nature of the inner ear as a target for therapy. Challenges in achieving safety and efficacy faced by clinicians treating inner ear diseases are similar to the difficulties encountered during preclinical drug development, and delivery remains the central barrier to progress. Current preclinical models require very large numbers of animals due to significant variability and relatively small responses in hearing function, and this is largely related to difficulties in delivery rather than limitations of the compounds themselves. Without reliable delivery systems capable of maintaining control over drug concentrations within the therapeutic window for extended periods, it is difficult to assess efficacy, and functional assays for drug-treated groups often fall short of expected results for this reason.
References
-
Peppi M, Marie A, Belline C, Borenstein JT (2018) Intracochlear drug delivery systems: a novel approach whose time has come. Expert Opinion on Drug Delivery 15(4): 319-324.
-
Liu H, Hao J, Kevin Li S (2013) Current strategies for drug delivery to the inner ear. Acta Pharmaceutica Sinica B 3(2): 86-96.
-
Ayoob AM, Borenstein JT (2015) The role of intracochlear drug delivery devices in the management of inner ear disease. Expert Opin Drug Deliv 12(3): 465-479.
-
Holley MC (2005) Keynote review: the auditory system, hearing loss and potential targets for drug development. Drug Discov Today 10(19): 1269-1282.
-
Plontke SK, Siedow N, Wegener R, Hans Peter Z, Alec NS (2007) Cochlear pharmacokinetics with local inner ear drug delivery using a three-dimensional finiteelement computer model. Audiol Neurootol 12(1): 37-48.
-
Breglio AM, Rusheen AE, Shide ED, Fernandez KA, Spielbauer KK, et al. (2017) Cisplatin is retained in the cochlea indefinitely following chemotherapy. Nat Commun 8 (1): 1654.
-
Crowson MG, Hertzano R, Tucci DL (2017) Emerging therapies for sensorineural hearing loss. Otol Neurotol 38(6): 792-803.
-
Suckfuell M, Lisowska G, Domka W, Kienle Gogolok A, Krzyzaniak A, et al. (2014) Efficacy and safety of AM-111 in the treatment of acute sensorineural hearing loss: a doubleblind, randomized, placebo-controlled phase II study. Otol Neurotol 35(8): 1317-1326.
-
Oishi N, Schacht J (2011) Emerging treatments for noise- induced hearing loss. Exp Opin Emerg Drugs 16(2): 235-
-
Mizutari K, Fujioka M, Hosoya M, Bramhall N, Okano HJ, et al. (2013) Notch inhibition induces cochlear hair cell regeneration and recovery of hearing after acoustic trauma. Neuron 77(1): 58-69.
-
McLean WJ, Yin X, Lu L, DR, Mc Lean D, et al. (2017) Clonal expansion of Lgr5-positive cells from mammalian cochlea and high-purity generation of sensory hair cells. Cell Rep 18(8): 1917-1929.
-
Suzuki J, Corfas G, Liberman MC (2016) Round-window delivery of neurotrophin 3 regenerates cochlear synapses after acoustic overexposure. Sci Rep 6: 24907.
-
Swan EE, MescherMJ, Sewell WF, Tao L, Borenstein JT (2008) Inner ear drug delivery for auditory applications. Adv Drug Deliv Rev 60: 1583-1599.
-
Borkholder DA (2008) State-of-the-art mechanisms of intra cochlear drug delivery. Curr Opin Otolaryngol Head Neck Surg 16(5): 472-477.
-
Salt AN, Plontke SK (2009) Principles of local drug delivery to the inner ear. Audiol Neurootol 14(6): 350- 360.
-
McCall AA, Swan EE, Borenstein JT, Sewell WF, Kujawa SG, et al. (2010) Drug delivery for treatment of inner ear disease: current state of knowledge. Ear Hear 31(2): 156-165.
-
Jackson LE, Silverstein H (2002) Chemical perfusion of the inner ear. Otolaryngologic Clinics of North America 35(3): 639-653.
-
Light JP, Silverstein H (2004) Trans tympanic perfusion: indications and limitations. Curr Opin Otolaryngol Head Neck Surg 12: 378-383.
-
Hoffer ME, Balough BJ, Gottshall KR (2008) Delivery of drugs to the inner ear. Curr Opin Otolaryngol Head Neck Surg 14(5): 329-331.
-
Darlington CL, Smith PF (2007) Drug treatments for tinnitus. Prog Brain Res 166: 249-262.
-
Plontke SKR, Wood AW, Salt AN (2002) Analysis of gentamicin kinetics in fluids of the inner ear with round window administration. Otol Neurotol 23(6): 967-974.
- Solution-Processed Chiral Perovskites for Biomedical Applications
- Nanotechnology in Health Chemistry and Medicine: Current Challenges and Future Directions
- Human Exposure to Micro- and Nanoplastics: Pathways, Toxicity, and Intervention Strategies
- Exosome Nanomedicine for Cancer Therapy
- Micro and Nanoplastics–Plastisphere, Biotoxicity, Impact on Human Health, and Mitigation Strategies
- Process Validation of Cefixime Powder for Suspension Dosage Form, 50 mL