MicroRNAs as Biomarker of Alzheimer’s Disease: Promises and Future Prospect
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder occurring in the elderly population. Millions of people in the age group of 60 and above are affected by Alzheimer’s disease worldwide. Damage caused by disease is currently irreversible and incurable. Early-onset and diagnosis of AD could help in delaying the progression of the disease. Earlier AD was diagnosed by clinical assessment and postmortem brain pathology. Therefore, improved approaches are required to sensitively track disease development and therapeutic efficacy. The pathological presence of ß amyloid plaques and Tau neurofibrillary tangles in cerebrospinal fluid (CSF) is the hallmark of detection. MicroRNAs (miRNAs), a 19-22 nucleotide noncoding RNAs circulating in the blood, regulates gene expression by protein repression. miRNAs are key regulators of gene expression in various biological processes and is emerging as a novel prognostic biomarker in various diseases. Recent evidence suggests the role of miRNAs in disease progression and pathogenesis of AD. Five databases, PubMed” MEDLINE, EMBASE, Web of Sciences, and Cochrane Library, were searched, using a combination of Mesh database or Emtree headings and free-text terms, to identify literature relating to miRNAs in Alzheimer’s disease. The comprehensive online electronic databases, only peer-reviewed, full-text original research articles including English literature, were included in the current review. The studies followed the inclusion criteria were critically assessed and checked using the PRISMA tool. In this review role of miRNAs as potential biomarkers in AD progression and pathogenesis will be covered with its elaborative function as a novel prognostic biomarker and its future prospects in the clinical implication of the same.
Introduction
Alzheimer’s disease (AD) is a global epidemic public health priority for the 21st century. It is growing in incidence due to enhanced human longevity and is now considered a leading cause of death, Alzheimer’s disease is a progressive, deterioration in cognitive function, an irreversible brain disorder that slowly destroys memory, thinking, and skills and, ultimately, the ability to carry out the simplest task [1].
Alzheimer’s disease involves the loss of neurons and synapses in the cerebral cortex and certain subcortical regions [2]. This loss results in gross atrophy of the affected regions, with degeneration in the parietal lobe and temporal lobe and parts of the frontal cortex and cingulate gyrus [3]. The increasing rate of people suffering from Alzheimer’s disease worldwide is alarming; the number of people affected is predicted to be increased by more than 75.63 million in 2030 and 135.46 million in 2050 [4]. The cause and molecular mechanism of Alzheimer’s disease pathogenesis remain largely unclear due to AD being one of the most complicated and complex age-related diseases [5]. Thus, a reliable biomarker for early diagnosis is extremely pivotal for the prevention of the AD process. To date, there is no effective cure for Alzheimer’s disease (AD), so the identification of fast and effective prognostic disease markers is warranted to improve the process of diagnosis and disease progression. Therefore, identification of a novel panel of biomarkers that accurately reflect Alzheimer’s disease pathology is a priority.
Emerging studies in recent years have revealed that the deregulation of epigenetic mechanisms could be a potential contributor to the pathogenesis of AD [6]. Hence identification of epigenetic regulators and their target genes contributing to the pathobiology of AD could prove potential biomarkers for the diagnosis and cure of AD [7]. Among the main epigenetic mechanisms linked with AD includes DNA methylation, histone modifications, and differential expression of long noncoding RNAs (lncRNAs), micro RNAs (miRNAs), circular RNA (circRNAs) and other noncoding RNAs [8]. The effects of these epigenetic mechanisms are closely related, since, for example, DNA methylation can control the expression of miRNA, and vice versa—miRNA can regulate the expression of methylation enzymes [9]. Furthermore, there is also a complex temporal and spatial cross-talk or endogenous competition between long noncoding RNA (lncRNA), circular RNA (circRNA), micro (miRNA), messenger RNA (mRNA) and other RNAs, which form RNA networks and shape the phenotypic disease outcomes [8]. Recent research has placed increasing importance on discovering RNAs networks for both understanding molecular mechanisms and developing novel diagnostic and prognostic markers as well as therapeutic targets [10]. In this review, we summarize the emerging preclinical and clinical evidence on the role of microRNAs (miRNAs), long noncoding RNAs (lncRNAs) in circulatory fluid, and AD pathogenesis, and discuss their potential usage as biomarker candidates for AD along with possible limitations.
Methods
Search Strategy
The initial literature searches were conducted on the comprehensive online electronic database, including English literature, research articles published till 31 march 2020. The search was conducted using “Scopus” “PubMed” MEDLINE, EMBASE, Web of Sciences, and Cochrane Library. The keywords and text used for search include: “Alzheimer’s disease,” “Confounding factors,” “risk factors,” “biomarker,” “Alzheimer’s and miRNA,” “Alzheimer’s disease, and miRNA profiling,” and “Alzheimer’s disease and neurodegenerative disease “.. Expanding these search terms on PubMed, relevant articles were selected for a comprehensive review, and investigation of literature was further supplemented by searching the reference articles created by the original investigators. A total of 10 studies were included in this systematic review (PRISMA guidelines; Moher, 2009), as outlined in Figure 1 [11].
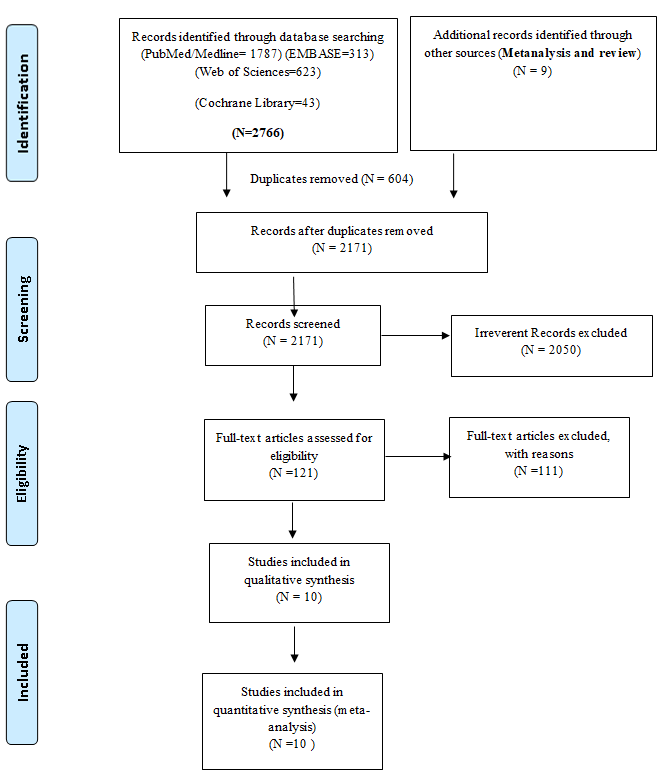
Figure1: Flow diagram expanding the relevant search terms related articles were selected, for a comprehensive systematic review (PRISMA protocol 2009).
Pathology of Alzheimer Disease
95% cases of AD are late-onset and sporadic, while around 5% of AD cases are early-onset and associated with genetic mutations in some proteins (e.g., presenilin 1, presenilin 2, amyloid precursor protein), which is known as familial AD [12]. Interestingly, biochemical changes produced in familial AD seem similar to those in sporadic AD [13]. In general, the physiopathology of AD is characterized by a loss of synapses mainly related to the extracellular deposition of the β-amyloid peptide in the form of senile plaques, one of the classic histological marks of AD [14]. This β-amyloid substance comes from the cleavage of the amyloid precursor protein (APP) by the beta-site APP- cleaving enzyme 1(BACE1). Another histological mark of the disease is tau protein intracellular accumulation [15]. This protein is involved in the maintenance of the cellular cytoskeleton microtubule network, and its function is enzymatically regulated by different phosphorylation degree. In fact, this hyperphosphorylated protein is less functional and forms oligomers that tend to autoaggregation and sedimentation, resulting in the formation of neurofibrillary tangles. Also, chronic inflammation could be an important physiopathological mechanism, contributing to the metabolism and accumulation of β-amyloid peptide [16]. Both amyloid and tau pathologies usually spread from medial temporal lobe grey matter to the rest of cortical grey matter in a relatively predictable pattern [17]. Initial involvement in medial temporal lobe structures that are involved in the correct episodic memory working explains the memory impairment as the first disease symptom [18]. Nevertheless, variations in pathology spreading would explain the different damage degrees in the brain cortex among patients, involving in some cases also language disturbance, frontal lobe dysfunction, and even agnostic or apraxia syndromes. Moreover, advanced-age patients show concurrent brain comorbidities (e.g., depression, psychiatric disorders). However, the prevalent vision of the physiopathological mechanisms of AD is considered incomplete, and it could be the cause of an inability to develop effective therapeutic targets based on the AD molecular pathogenesis [19]. Recent studies suggest that MCI due to AD is the result of an imbalance in the interactions among different brain cell types, pathogenic forms of tau and amyloid proteins, and the brain signaling pathways impairment [20]. In this way, the neurodegenerative process would affect each cell type at multiple levels (epigenomic, transcriptomic, metabolomic/ lipidomic, proteomic) [21]. Therefore, complete knowledge of the AD mechanisms could be achieved from a multi-omic approach applied to different biological samples. In this sense, the omic tools would contribute importantly to the knowledge of the early AD physiopathological mechanisms and develop specific and reliable AD biomarkers in common biological samples.
Current Diagnosis of Alzheimer’s Disease
From a clinical point of view, AD is a pathological condition characterized by specific structural changes in the brain and a characteristic pattern of cognitive and functional abilities [18]. Briefly, its symptomatic development consists of three phases: i) preclinical phase, characterized by a normal cognitive status while ongoing brain pathology is being generated; ii) Mild cognitive impairment (MCI), characterized by the presence of symptoms and signs of cognitive deficit secondary to fully developed brain pathology [22]. The habitual performance on daily life activities, however, is not altered; and iii) dementia, characterized by progressively greater cognitive impairment affecting the ability to carry out everyday activities. Cognitive markers are altered at the MCI phase, while image and cerebrospinal fluid (CSF) markers start to get alter from the preclinical phase [23]. Current research diagnostic criteria from the National Institute on Aging and the Alzheimer’s Association (NIA- AA) propose the simultaneous use of neuropsychological evaluations, neuroimaging techniques, and biomarkers in CSF samples to obtain a reliable and early AD diagnosis [24]. In this sense, the standard diagnosis of MCI due to AD is based on global neuropsychological evaluations (Clinical Dementia Rating, CDR; Global Deterioration Scale, GDS, specific cognitive evaluations (episodic memory, attention, language, recognition, praxis, executive function), structural and functional neuroimaging (Magnetic Resonance Imaging, MRI; positron emission tomography, PET), and CSF biomarkers (β-amyloid, total tau (t-tau), phosphorylated tau (p-tau)) AD diagnostic criteria allow in vivo diagnosis using pathological processes detection; however, they show some limitations to be introduced in clinical practice [25]. In fact, MRI features are relatively not AD specific or sensitive, PET is a costly imaging procedure not available in most hospitals, CSF samples are obtained by an invasive procedure with some contraindications and secondary effects, so it is commonly rejected by patients, and neuropsychological evaluations are time-consuming [26]. A non-invasive and non-expensive diagnostic method is required in the AD research field and in the global dementia assistance network to improve treatment and prognosis management. In the searching for specific and reliable AD biomarkers in non- invasive biological samples, the omics technologies play an important role since they can address the complex diagnosis from different molecular levels [27, 28, 29].
![Figure 2: Role of tau hyperphosphorylation information of hyperphosphorylated neurofibrillary tangles [NFTs], which consequently leads to neurodegeneration and commencement of tauopathies.](/fulltextimages/6972/fig_2.png)
miRNA in Alzheimer’s Disease
A microRNA (miRNA) are endogenous short [19- 22 nt) noncoding RNA molecules that can function in RNA silencing and post-transcriptional regulation of gene expression, reducing the expression of their target mRNAs either by inhibiting its translation or by promoting its degradation [30]. miRNAs usually regulate gene expression post-transcriptionally by binding to the 3’ UTR (untranslated region) for target mRNA [31]. A single miRNA can target several mRNAs and repress protein production by destabilizing the mRNA and translational silencing, increasing the complexity of the regulatory mechanism mediated by these molecules. In malignancies, miRNAs can act as oncogenes, including sustaining proliferative signaling, evading growth or tumor suppressors, under certain conditions [32]. The miRNA expression across human tissues profiles are specific of tissue and cell type. Variations in miRNA levels have been reported for patients’ solid tissues, blood, and other body fluids, making miRNAs promising candidates for markers in a manifold of diseases [33]. The still increasing information density on reference repository 1917 human miRNA precursors, coding for more than 2656 mature miRNAs have been described in humans (Julia Alles) studies about biogenesis, functions, roles, and characterization of the mechanism of action of miRNAs have grown considerably, and nowadays, they are considered as pathophysiological players and excellent biomarkers of Alzheimer’s disease [34].
The Role of miRNA in AD Pathogenesis
The fact that Alzheimer’s disease patients are distinguished by miRNA alteration in the brain and biological fluid changes, including blood, plasma, and cerebrospinal fluid (CSF), inspired the concept of utilizing such noncoding sequences as disease biomarkers [35]. At present, Aβ peptides and tubulin-associated unit (tau) proteins are the only biomarkers currently recognized for AD; however, some CSF and blood tests have certain drawbacks. In addition to the concerns relevant to the standardization of the technique of body fluids, there is inadequate support of modern clinical practice for the acceptance of cut-off values of such biomarkers (alone or in combination) [35]. Therefore, the predictive role of such biomarkers is also debated in individuals with mild cognitive impairment (MCI). Prediction in asymptomatic individuals to develop symptomatic AD (MCI or dementia) is important. Furthermore, there is currently no therapeutic agent capable of curing or preventing AD [36]. Biomarkers may also be used to determine the efficacy of therapeutic agents under study in clinical trials and thereby speed the phase of therapeutic development. MiRNAs, unlike mRNAs, are stable enough in biological fluids, including CSF, plasma, and serum. Besides, many of them target genes directly involved in AD pathophysiologies such as presenilins, BACE- 1, APP, TOMM40, and BDNF [37]. Moreover, there is evidence that, in APOE4 mice, the association between certain miRNAs (miR-146a) and inflammatory mediators (NFκB) seems to be even greater. Analysis of miRNAs in body fluids is a relatively simple procedure Angelucci F, et al. [35], and a non-invasive approach. If we compare miRNAs to conventional protein- based biomarkers of AD, the level of sensitivity achieved for miRNAs due to amplification by PCR is far superior to what is currently available for proteins [38]. Besides, the cost of miRNA quantification is far lower than that of established biomarkers, such as structural magnetic resonance imaging (MRI) and molecular neuroimaging with positron emission tomography (PET). For this purpose, many miRNAs appear to be promising [39].
miRNAs as Candidate Biomarkers
Several studies have found miRNA as a signature representative of diseases. Serum, plasma, and other body fluids have varying expression of miRNA in numerous pathologies, making them an appropriate candidate for biomarkers [40]. As many miRNAs are tissue-specific, their systemic dysregulation in peripheral blood points towards a distinct pathology. miRNAs are now emanating as leading biomarkers, not only for diagnostic purposes but also for disease stratification and therapeutics [41]. It has also been observed that detecting a small number of miRNAs gives more information about the disease than studying the expression of several mRNAs. An ideal biomarker is one that is specific to the disorder, can be detected early in the disease process, accessible from peripheral tissue (non- invasive), stable, reproducible, and associated with a known mechanism [42]. There are many challenges to identify new protein-based biomarkers due to the complexity of the structure of a protein and various post-translational modifications [43]. miRNAs may be more attractive as biomarkers due to their lower complexity, tissue specificity, and no known post-translational modifications. They are stable in blood, urine, and tissues, and can, therefore, serve as potential biomarkers for many conditions, including AD [39]. However, the precision and accuracy of miRNA measurements are challenging. A miRNA is a short sequence of nucleotides with highly variable GC content, which leads to different hybridization properties and makes its detection difficult. Furthermore, their minuscule amount present in serum or urine requires further advancements in technology to develop robust, precise, and highly sensitive techniques for miRNA detection [43]. Despite the limitations, the discovery of miRNAs has opened new horizons in the unraveling of the pathomechanisms of various diseases and has given a whole new dimension to the field of biomarkers [44].
Various Techniques of miRNA Profiling
Various techniques can study the relative expression of miRNAs. miRNA profiling typically includes three main phases: the process of exploration, the process of validation, and the functional study [45]. The miRNA expression profile is evaluated for differentially expressed miRNAs between cases and controls in the discovery process, to allow for maximal potential targets [46]. This is followed by a validation step, in which the findings of the first step are corroborated employing more sensitive techniques. Finally, the functional relevance of miRNAs and the mRNA–miRNA relationship is explored utilizing in silico analysis [47]. Usually, hybridization-based methods, like microarrays, are used as an initial approach to finding the potential candidate miRNAs; real-time PCR (qRT-PCR) is often used subsequently to validate highly dysregulated miRNAs among the distinct profile obtained using microarrays. qRT-PCR, due to its high precision, accuracy, and vast range, remains the gold standard for miRNA quantification. miRNAs can be sequenced using next-generation sequencing (NGS) platforms, in which after reverse transcription, millions of DNA fragments are sequenced in parallel [48]. A range of platforms can be used for miRNA sequencing, including SOLiD (Applied Biosystems), Solexa, HiSeq, MiSeq, MiniSeq, NextSeq (Illumina), and Ion Torrent (Invitrogen), to name a few. Using bioinformatics, these fragments are aligned and mapped, and their expression levels are analyzed, thus eliminating the need for sequence-specific hybridization probes which are required in a microarray. Moreover, NGS has the advantages of high sensitivity and resolution, and excellent reproducibility, though considerable computational support is required. The biggest drawback is that there is a great variation in the performance among the different platforms [49]. hybridization-based platforms exhibit lower sensitivity, irrespective of input RNA amount, while sequencing-based platforms display high sensitivity in the presence of ample of RNA, and the sensitivity is lost, if the amount of RNA is limiting. Thus, there are considerable interplatform differences, with different pros and cons for each technique [50].
Discussion
A total of ten peer-reviewed studies were included, and comprehensively reviewed in this analysis. All of them were multi-institutional. The study characteristics, like the country, mean age of the participants, study cohort, sample type, are described in Table 1.The ten studies included analyzed 771 patients with Alzheimer’s disease and 458 with healthy control in total. The controls were from patients undergoing (Mini-mental State Examination (MMSE) score≥27);for various neurological indications. After evaluating each study, using the PRISMA tool (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) tool, the score ranged from moderate to high for all the included studies. Four were from China, two from the United States, one from Brazil, Ireland, Spain, and one from Iran. The sample type was CSF in four studies, and plasma in the three and remaining one obtained from the brain post-mortem banked human skin fibroblasts and lymphoblasts. The baseline characteristics of all the studies are listed in Table2. Total RNA was extracted in all the manuscripts using various kits, as described in Table3. All except two used global miRNA profiling by microarray, followed by validation by qRT-PCR. The remaining two research studies analyzed the expression of several chosen miRNAs using qPCR. Different normalization controls for qRT-PCR were utilized in the various studies; most common was U6snRNA.
| S. No | Author | Country | Sample Size | Sample Type | Mean Age (Years) | Characteristics of Controls | ||
|---|---|---|---|---|---|---|---|---|
| Cases | Controls | |||||||
| 1 | [51] | China | Case-80 Control-40 | RT-qPCR | CSF | 70.3±6.8 | 69.3±9.4 | (1) no dementia symptoms (Mini-mental State Examination (MMSE) score≥27); (2) no significant psychiatric symptoms; (3) no history of stroke, epilepsy, Parkinson’s disease or another severe neurological disease; (4) age≥40 years; (5) willingness to receive CSF examination;(6) With normal CSF biomarkers (Aβ42, t-tau, and p-tau) |
| Case-8 Control-8 | Microarray | CSF | 69.3±7.5 | 67.9±7.9 | ||||
| 2 | [52] | Brazil | Case-36 Control-38 | Whole blood | 79.5 + 6.0 | 76.4 + 9.2 | Patients without dementia | |
| 3 | [53] | USA | Case-27 Control-15 | Frontal cortex Broadmann’s area 10 dissected from brain obtained at post-mortem banked human skin fibroblasts and lymphoblasts. | NA | NA | Healthy controls were obtained from three NIH NeuroBioBanks. | |
| 4 | [54] | China | Case- (17 AD and 35 with MCI) Control-41 | CSF | (72.4±3.1 MCI) (74.1±3.2AD) | NA | Healthy Control | |
| 5 | [55] | Ireland | Case MCI (n = 30)AD (n = 25) Control (n = 31) | Plasma | (76.8 (4.0) MCI) (84.6 (3.5)AD) | 75.0 (4.7) [69–86] | Healthy Control | |
| 6 | [56] | Iran | Case 56 Control 50 | Serum | 73.90 ± 8.95 | 71.36 ± 7.4 | Healthy controls | |
| 7 | [57] | China | Case 120 Control 120 | Plasma | 72.5 ± 7.7 | 71.2 ± 10.8 | Healthy controls | |
| 8 | [58] | China | Case (101 MCI) Dementia of Alzheimer type (DAT) 107 Control 30 | Serum | (MCI 61.63 ± 7.32) DAT (74.15 ± 7.93) | NA | Healthy controls | |
| 9 | [59] | Spain | Case 26 MCI And 56 AD Control 14 | Plasma | 72.0 ± 8.49 MCI 77.77 ± 6.69 AD | 68.29 ± 8.99 | Healthy controls | |
| 10 | [60] | USA | Case 47 AD | CSF | 73.13 ± 9.22 | 72.72 ± | Controls were in good health with | |
| Controls 71 | 5.91 | a mean MMSE score of 29.13 ± 1.31 |
Table 1: Research methodologies.
Table1: The study characteristics, like the country, mean age of the participants, study cohort, sample type, are described.
| Methodologic Parameter | Number of Studies (Out of 8 Manuscripts Analyzed) |
| Kits used for RNA extraction | |
|---|---|
| mirVANA PARIS kit | 2 |
| PureZOL RNA isolation reagent | 1 |
| Trizol | 1 |
| Small RNA kit (Qiagen,) | 3 |
| Beyotime small RNA isolation kit | 1 |
| SanPrep Column microRNA Mini-Preps Kit | 1 |
| miRcute miRNA isolation kits | 1 |
| Real-time PCR technique | |
| SYBR Green | 5 |
| TaqMan | 5 |
| Normalization control in qPCR | |
| Internal reference | 6 |
| External reference | 4 |
Table 2: Research methodologies.
We found only a single circulating miRNA dysregulated in a similar direction, across more than one study, miR-20a (Table 3). The various dysregulated miRNAs could not be statistically evaluated due to the lack of consensus among the published literature and the absence of statistical data presented in the manuscripts.
| Author | miRNA detection methods | Normalization Control Used in qRT-PCR | |
|---|---|---|---|
| 1 | [51] | Microarray RT-qPCR | GAPDH |
| 2 | [52] | RT-qPCR | RNU43 |
| 3 | [53] | RT-qPCR | U6snRNA |
| 4 | [54] | RT-qPCR | U6snRNA |
| 5 | [55] | RT-qPCR | 4 internal controls (ath-miR159a (negative control), RNU48, RNU44,and U6 rRNA) |
| 6 | [56] | RT-qPCR | CelmiR-39-3p |
| 7 | [57] | RT-qPCR | U6snRNA |
| 8 | [58] | RT-qPCR | U6snRNA |
| 9 | [59] | RT-qPCR | RNU48 |
| 10 | [60] | RT-qPCR | U6snRNA |
Table 3: List of circulating miRNAs dysregulated in Alzheimer’s disease after validation by qRT-PCR, as found in various studies.
The miR-9 expression is confined to the nervous system and is responsible for controlling neuronal physiology. It regulates the differentiation of neurons from neural progenitor cells. Therefore, the deregulation of miR-9 leads to neurodegenerative disorders by negatively regulating BACE1. Downregulation of miR-9 leads to progression of Aß-42 aggregation and senile plague formation negatively affectingCNS. miR-455-3pis also one of the potential biomarkers, differentially expressed in AD from other neurological disorders. It has a high level of expression in both sporadic and familial AD localized in Brain, fibroblast, and B lymphocytes. miR-455-3p controls a significant number of genes expression such as APP, SMAD2, SMAD4, NGF,USP25,PDRG1, UBQ2N, NRXN1 etc. CSF and blood containingsmiR-let-7band miR206 are upregulated in AD which positively correlates with t-tau and p-tau expression. Kelly et al. state that both are differentially expressed as per the disease severity. It is found the level of miR-let- 7b is comparatively higher than miR-206 in MCI as the disease severity increases the level ofmiR-206 increases. miR106b which is involved in Aß- clearance is found to be downregulated in serum of AD patients. Similarly, miR- 103 and miR-107 are downregulated and are negatively correlated in AD. Both are responsible for silencing BACE1 and RE1; thus, downregulation of miR-103 and miR-107leads to increased susceptibility of AD. Increased level of miR-135a and miR-384 is found in serum of AD patients which control the expression of APP and BACE1 whereas reduced level of miR-193b is observed in the same which controls APP expression. Circular RNA also plays a crucial role in disease pathology of AD. 112 CirRNA were upregulated whereas 51 are downregulated. Circ-LPAR1, AXL-1, and GPHN were significantly upregulated with positive correlation with t-tau and p-tau whereas Cir-PCCA, HAUS-4, K1F18B is downregulated with positive correlation with Aß42 expression.
Conclusion
miRNA and Cir-RNA play a crucial role in disease progression and pathology of Alzheimer’s. Literature reveals that circulating miRNA are potential candidates as a non- invasive biomarker for Alzheimer’s. Studies have identified different miRNA for prognostic purpose but none have done a comparative analysis or have identified the best biomarker for AD of clinical relevance. Therefore more extensive, well- controlled, systematic validation studies need to be carried out involving a larger subset of population with uniformity in research approaches. Furthermore, an elaborated study needs to be carried out to identify more reliable and stably expressed miRNA to identify .a diagnostic panel of differentially regulated miRNA that could be used for detection and progression of AD.
Conflict of Interest
The authors have declared that the research was conducted in the absence of any commercial or financial relationships without any conflict of interest.
Author Contributions
R.S., C.P.C. have participated in the study design, data collection, data evaluation, drafting, and analysis. A.A., A.S.
have contributed to manuscript concept and design. All authors have participated in the protocol development, collection, and analysis of the data, manuscript writing and final approval.
Acknowledgment
This research was Sponsored by Multi-Disciplinary Research Units (MRUs) a grant by ICMR-Department of Health Research
References
-
(2020) What Is Alzheimer’s Disease? National Institute on Aging.
-
Deture MA, Dickson DW (2019) The neuropathological diagnosis of Alzheimer’s disease. Mol Neurodegener 14(1): 32.
-
Schmahmann JD, Smith EE, Eichler FS, Filley CM (2008) Cerebral white matter: Neuroanatomy, clinical neurology, and neurobehavioral correlates. Ann N Y Acad Sci 1142: 266-309.
-
Lai NYY, Mok CCM, Siu AMH (2019) Efficacy of Computer- Assisted Cognitive Training in People with Early Dementia-A Single-Blind Randomized Controlled Trial. J Aging Stud Ther 1(1): 1-6.
-
Chen YG (2018) Research Progress in the Pathogenesis of Alzheimer’s Disease. Chin Med J (Engl) 131(13): 1618-1624.
-
Millan MJ (2014) The epigenetic dimension of Alzheimer’s disease: Causal, consequence, or curiosity? Dialogues Clin Neurosci 16(3): 373-393.
-
Mazzone R, Zwergel C, Artico M, Taurone S, Ralli M, et al. (2019) The emerging role of epigenetics in human autoimmune disorders. Clinical Epigenetics 11(34): 1-15.
-
Liu X, Jiao B, Shen L (2018) The Epigenetics of Alzheimer’s Disease: Factors and Therapeutic Implications. Front Genet 9: 579.
-
Chen S, Yang J, Wei Y, Wei X (2020) Epigenetic regulation of macrophages: from homeostasis maintenance to host defense. Cell Mol Immunol 17(1): 36-49.
-
Madadi S, Schwarzenbach H, Saidijam M, Mahjub R, Soleimani M, et al. (2019) Potential microRNA-related targets in clearance pathways of amyloid-β: novel therapeutic approach for the treatment of Alzheimer’s disease. Cell Biosci 9(91): 1-19.
-
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med 6(7): e1000097.
-
Lanoiselée HM, Nicolas G, Wallon D, Rovelet-Lecrux A, Lacour M, et al. (2017) APP, PSEN1, and PSEN2 mutations in early-onset Alzheimer disease: A genetic screening study of familial and sporadic cases. PLOS Med 14(3): e1002270.
-
Selkoe DJ (2008) Biochemistry and Molecular Biology of Amyloid β-Protein and the Mechanism of Alzheimer’s Disease. Handb Clin Neurol 89: 245-260.
-
Hebert LE, Scherr PA, Bienias JL, Bennett DA, Evans DA et al. (2003) Alzheimer disease in the US population: Prevalence estimates using the 2000 census. Arch Neurol 60(8): 1119-1122.
-
Sun X, Chen WD, Wang YD (2015) β-Amyloid: The key peptide in the pathogenesis of Alzheimer’s disease. Front Pharmacol 6: 221.
-
Currais A, Fischer W, Maher P, Schubert D (2017) Intraneuronal protein aggregation as a trigger for inflammation and neurodegeneration in the aging brain. FASEB J 31(1): 5-10.
-
Pasquini L, Rahmani F, Maleki-Balajoo S, La Joie R, Zarei M, et al. (2019) Medial Temporal Lobe Disconnection and Hyperexcitability Across Alzheimer’s Disease Stages. J Alzheimers Dis Rep 3(1): 103-112.
-
Jahn H (2013) Memory loss in alzheimer’s disease. Dialogues Clin Neurosci 15(4): 445-454.
-
Peña-Bautista C, Baquero M, Vento M, Cháfer-Pericás C (2019) Omics-based Biomarkers for the Early Alzheimer Disease Diagnosis and Reliable Therapeutic Targets Development. Curr Neuropharmacol 17(7): 630-647.
-
Rajmohan R, Reddy PH (2017) Amyloid-Beta and Phosphorylated Tau Accumulations Cause Abnormalities at Synapses of Alzheimer’s disease Neurons. J Alzheimers Dis 57(4): 975-999.
-
Aliyu Musa, Laleh Soltan Ghoraie, Shu-Dong Zhang, Galina Glazko, Olli Yli-Harja, et al. (2018) A review of connectivity map and computational approaches in pharmacogenomics. Brief Bioinform 19(3): 506-523.
-
Tarawneh R, Holtzman DM (2012) The clinical problem of symptomatic Alzheimer disease and mild cognitive impairment. Cold Spring Harb Perspect Med 2(5): a006148.
-
Tautvydaite D, Kukreja D, Antonietti JP, Henry H, Von Gunten A, et al. (2017) Interaction between personality traits and cerebrospinal fluid biomarkers of Alzheimer’s disease pathology modulates cognitive performance. Alzheimer’s Res Ther 9(1): 6.
-
Jack CR, Bennett DA, Blennow K, Carrillo MC, Dunn B, et al. (2018) NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement 14(4): 535-562.
-
Silverberg NB, Ryan LM, Carrillo MC, Sperling R, Petersen RC, et al. (2011) Assessment of cognition in early dementia. Alzheimers Dement 7(3): e60-e76.
-
Segovia F, Bastin C, Salmon E, Górriz JM, Ramírez J, et al. (2014) Combining PET Images and Neuropsychological Test Data for Automatic Diagnosis of Alzheimer’s Disease. PLoS One 9(2): e88687.
-
Hampel H, O’Bryant SE, Molinuevo JL, Zetterberg H, Masters CL, et al. (2018) Blood-based biomarkers for Alzheimer disease: mapping the road to the clinic. Nat Rev Neurol 14(11): 639-652.
-
Bernier F, Kumar P, Sato Y, Oda Y (2015) Recent Progress in the Identification of Non-Invasive Biomarkers to Support the Diagnosis of Alzheimer’s Disease in Clinical Practice and to Assist Human Clinical Trials. Alzheimer’s Disease-Challenges for the Future.
-
Shen L, Xia S, Zhang H, Yao F, Liu X, et al. (2019) Precision Medicine: Role of Biomarkers in Early Prediction and Diagnosis of Alzheimer’s Disease. Molecular Medicine.
-
O’Brien J, Hayder H, Zayed Y, Peng C (2018) Overview of microRNA biogenesis, mechanisms of actions, and circulation. Front Endocrinol (Lausanne) 9: 402.
-
Catalanotto C, Cogoni C, Zardo G (2016) MicroRNA in control of gene expression: An overview of nuclear functions. International Journal of Molecular Sciences 17(10): 1712.
-
Long JM, Maloney B, Rogers JT, Lahiri DK (2019) Novel upregulation of amyloid-β precursor protein (APP) by microRNA-346 via targeting of APP mRNA 5′-untranslated region: Implications in Alzheimer’s disease. Mol Psychiatry 24(3): 345-363.
-
Rhizobium GE (2013) Complete Genome Sequence of the Sesbania Symbiont and Rice. Nucleic Acids Res 1: 13-14.
-
Alles J, Fehlmann T, Fischer U, Backes C, Galata V, et al. (2019) An estimate of the total number of true human miRNAs. Nucleic Acids Res 47(7): 3353-3364.
-
Angelucci F, Cechova K, Valis M, Kuca K, Zhang B, et al. (2019) MicroRNAs in Alzheimer’s disease: Diagnostic markers or therapeutic agents? Front Pharmacol 10: 665.
-
Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, et al. (2011) The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7(3): 270-279.
-
Etheridge A, Lee I, Hood L, Galas D, Wang K et al. (2011) Extracellular microRNA: A new source of biomarkers. Mutat Res 717(1-2): 85-90.
-
Condrat CE, Thompson DC, Barbu MG, Bugnar OL, Boboc A, et al. (2020) miRNAs as Biomarkers in Disease: Latest Findings Regarding Their Role in Diagnosis and Prognosis. Cells 9(2): 276.
-
Young PNE, Estarellas M, Coomans E, Srikrishna M, Beaumont H, et al. (2020) Imaging biomarkers in neurodegeneration: Current and future practices. Alzheimer’s Research and Therapy 12(49): 1-17.
-
Backes C, Meese E, Keller A (2016) Specific miRNA Disease Biomarkers in Blood, Serum and Plasma: Challenges and Prospects. Mol Diagn Ther 20(6): 509- 518.
-
Watson CN, Belli A, Di Pietro V (2019) Small non-coding RNAs: New class of biomarkers and potential therapeutic targets in neurodegenerative disease. Front Genet 10: 364.
-
Mushtaq G, Greig NH, Anwar F, Zamzami MA, Choudhry H, et al. (2016) miRNAs as Circulating Biomarkers for Alzheimer’s Disease and Parkinson’s Disease. Med Chem 12(3): 217-225.
-
Chandramouli K, Qian PY (2009) Proteomics: Challenges, Techniques and Possibilities to Overcome Biological Sample Complexity. Hum Genomics Proteomics 1(1): 239204
-
Pritchard CC, Cheng HH, Tewari M (2012) MicroRNA profiling: Approaches and considerations. Nat Rev Genet 13(5): 358-369.
-
Walayat A, Yang M, Xiao D (2019) Therapeutic Implication of miRNA in Human Disease. In: Antisense Therapy. Intech Open
-
Liu B, Li J, Cairns MJ (2014) Identifying miRNAs, targets and functions. Brief Bioinform 15(1):1-19.
-
Kuhn DE, Martin MM, Feldman DS, Terry AV, Nuovo GJ, et al. (2008) Experimental validation of miRNA targets. Methods 44(1): 47-54.
-
Zhao Z, Jinde S, Koike S, Tada M, Satomura Y, et al. (2019) Altered expression of microRNA-223 in the plasma of patients with first-episode schizophrenia and its possible relation to neuronal migration-related genes. Transl Psychiatry 9(289): 2-11.
-
Tripathi R, Sharma P, Chakraborty P, Varadwaj PK (2016) Next-generation sequencing revolution through big data analytics. Front Life Sci 9(2): 119-149.
-
Godoy PM, Barczak AJ, DeHoff P, Srinivasan S, Das S, et al. (2019) Comparison of miRNA profiling methods using synthetic miRNA pools and standardized exRNA samples reveals substantial performance differences. bioRxiv
-
Li Y, Fan H, Sun J, Ni M, Zhang L, et al. (2020) Circular RNA expression profile of Alzheimer’s disease and its clinical significance as biomarkers for the disease risk and progression. Int J Biochem Cell Biol 123: 105747.
-
Souza VC, Morais GS, Henriques AD, Machado Silva W, Perez DIV, et al. (2020) Whole-Blood Levels of MicroRNA-9 Are Decreased in Patients With Late-Onset Alzheimer Disease. Am J Alzheimers Dis Other Demen 35: 153331752091157.
-
Kumar S, Reddy PH (2018) MicroRNA-455-3p as a potential biomarker for Alzheimer’s disease: An update. Front Aging Neurosci 10: 41.
-
Liu Y, He X, Li Y, Wang T (2018) Cerebrospinal fluid CD4+ T lymphocyte-derived miRNA-let-7b can enhances the diagnostic performance of Alzheimer’s disease biomarkers. Biochem Biophys Res Commun 495(1): 1144-1150.
-
Kenny A, McArdle H, Calero M, Rabano A, Madden SF, et al. (2019) Elevated plasma microRNA-206 levels predict cognitive decline and progression to dementia from mild cognitive impairment. Biomolecules 9(11): 734.
-
Madadi S, Saidijam M, Yavari B, Soleimani M (2020) Downregulation of serum miR-106b: a potential biomarker for Alzheimer disease. Arch Physiol Biochem, pp: 1-5.
-
Wang J, Chen C, Zhang Y (2020) An investigation of microRNA-103 and microRNA-107 as potential blood- based biomarkers for disease risk and progression of Alzheimer’s disease. J Clin Lab Anal 34(1): e23006.
-
yang TT, Liu CG, Gao SC, Zhang Y, Wang PC, et al. (2018) The Serum Exosome Derived MicroRNA−135a, −193b, and −384 Were Potential Alzheimer’s Disease Biomarkers. Biomed Environ Sci 31(2): 87-96.
-
Siedlecki Wullich D, Català Solsona J, Fábregas C, Hernández I, Clarimon J, et al. (2019) Altered microRNAs related to synaptic function as potential plasma biomarkers for Alzheimer’s disease. Alzheimer’s Res Ther 11(1): 46.
-
Wiedrick JT, Phillips JI, Lusardi TA, McFarland TJ, Lind B, et al. (2019) Validation of MicroRNA Biomarkers for Alzheimer’s Disease in Human Cerebrospinal Fluid. J Alzheimers Dis 67(3): 875-891.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury