Radiological Progression of Pyogenic Brain Abscess with Antibiotics uses Compared to Surgical Intervention
Background: Brain abscess is a worldwide health problem with a high morbidity and mortality rate. It begins as a localized area of cerebritis and develops into an encapsulated will-formed abscess. The Pyogenic brain abscess formation starts when bacteria enter cerebral tissues as with trauma, or contiguous spread from a suppurative focus or through hematogenous dissemination from a distant infection. Methods: The study analyses the effect of antibiotics versus the surgical intervention in the curative treatment of pyogenic brain abscess. It is a retrospective analysis study conducted on a series of 25 patients having various stages of pyogenic brain abscess (BA) diagnosed between January 2018 and January 2023 in our institution. All the patients conducted a standard data collection including clinical assessment, radiological and laboratory investigations, medical treatment (with triple intravenous antibiotics), and surgical abscess aspiration. The surgical and medical treatments were compared depending on the radiological and the clinical improvement. Results: Clinical improvement was temporary for all patients with continuous medical treatment for a short time, without radiological improvement. While after surgical aspiration all patients had dramatic radiological, clinical, and laboratory improvement. Conclusion: The gold standard treatment of brain abscess is surgical intervention. Medical treatment could reduce the clinical effects of brain abscess, but it is not considered as a definitive cure.
Introduction
Brain abscess is a universal health problem with a high morbidity and mortality rate [1]. It is considered one of the most serious diseases of the CNS, with a higher morbidity rate in the fourth decade of life [1]. It begins as a localized area of cerebritis and develops into an encapsulated will-formed mass-like lesion [2], with non-specific clinical symptoms and signs [3]. The Pyogenic brain abscess formation starts when bacteria enter cerebral tissues as with trauma, or contiguous spread from a suppurative focus, or through hematogenous dissemination from a distant infection [4]. In contrast to a parenchymal brain abscess, a primary intraventricular abscess is a slowly progressing infectious process at which bacteria enter the ventricles through the choroid plexus [5]. Computed Tomography (CT) is used for the diagnosis of brain abscesses as well as for follow-up [6]. In addition to CT, MR imaging has contributed to the differential diagnosis of brain abscesses. Brain abscess surgical aspiration may be performed with the aid of an endoscope, stereotactic aspiration, intraoperative ultrasound guidance and with Neuronavigation uses with satisfactory results than medical treatment alone.
Methods
A retrospective analysis study was conducted on a series of 25 patients having various stages of pyogenic brain abscess (BA) between January 2018 and January 2023 in our institution. All the patients conducted a standard data collection which included: clinical assessment, radiological, laboratory investigations, medical treatment (with antibiotics), and surgical aspiration. The surgical and medical treatment results were compared depending on radiological and clinical findings and improvement of the patient. The study includes all patient’s demographic data, neurological status, clinical presentation, radiological, and laboratory findings in Tables 1 & 2.
| Sex | Age | Headache | Nausea and Vomiting | Fits | Weakness | Fever | CT Brain Abscess Stages | MRI Brain Rule out other Lesion | Lab Examination ESR, C Reactive Protein, WBS Count | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 45 | +ve | +ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 2 | F | 37 | +ve | +ve | +ve | +ve | +ve | Cerebritis | +ve | +ve |
| 3 | M | 31 | +ve | -ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 4 | M | 45 | +ve | -ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 5 | M | 60 | +ve | +ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 6 | F | 56 | +ve | -ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 7 | M | 41 | +ve | -ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 8 | F | 32 | +ve | +ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 9 | M | 31 | +ve | +ve | -ve | +ve | +ve | Cerebritis | +ve | +ve |
| 10 | M | 58 | +ve | +ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 11 | M | 48 | +ve | -ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 12 | F | 59 | +ve | -ve | +ve | -ve | +ve | Cerebritis | +ve | +ve |
| 13 | M | 45 | +ve | -ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 14 | M | 55 | +ve | -ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 15 | M | 39 | +ve | -ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 16 | M | 39 | +ve | -ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 17 | M | 55 | +ve | -ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 18 | M | 60 | +ve | +ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 19 | M | 57 | +ve | -ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 20 | F | 41 | +ve | -ve | -ve | +ve | +ve | Cerebritis | +ve | +ve |
| 21 | M | 43 | +ve | -ve | +ve | +ve | +ve | Cerebritis | +ve | +ve |
| 22 | M | 55 | +ve | +ve | -ve | -ve | +ve | Cerebritis | +ve | +ve |
| 23 | M | 37 | +ve | -ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 24 | M | 55 | +ve | +ve | -ve | -ve | +ve | Capsule | +ve | +ve |
| 25 | M | 49 | +ve | +ve | -ve | -ve | +ve | Capsule | +ve | +ve |
Table 1: Master Table Retrospective Analysis.
| Conservative Treatment Duration Before Surgery in Weeks | MRI\CT Improvement with Conservative Treatment | Clinical and Lab Improvement with Conservative Treatment | Radiological, Clinical, Lab Improvement after Aspiration | In Weeks | |
|---|---|---|---|---|---|
| 1 | 2 | -ve | -ve | +ve | 4 weeks |
| 2 | 6 | -ve | -ve | +ve | 8 w multiple abscess |
| 3 | 2 | -ve | -ve | +ve | 4 w |
| 4 | 2 | -ve | -ve | +ve | 6w |
| 5 | 2 | -ve | -ve | +ve | 6w multiple abscess |
| 6 | 2 | -ve | -ve | +ve | 6w |
| 7 | 4 | -ve | -ve | +ve | 4w |
| 8 | 2 | -ve | -ve | +ve | 6w |
| 9 | 4 | -ve | -ve | +ve | 6w |
| 10 | 4 | -ve | -ve | +ve | 8w multiple abscess |
| 11 | 2 | -ve | -ve | +ve | 6w |
| 12 | 3 | -ve | -ve | +ve | 8w multiple abscess |
| 13 | 2 | -ve | -ve | +ve | 8w multiple abscess |
| 14 | 2 | -ve | -ve | +ve | 8w multiple abscess |
| 15 | 4 | -ve | -ve | +ve | 6w |
| 16 | 2 | -ve | -ve | +ve | 4w |
| 17 | 2 | -ve | -ve | +ve | 6w multiple abscess |
| 18 | 3 | -ve | -ve | +ve | 5w |
| 19 | 4 | -ve | -ve | +ve | 4w |
| 20 | 2 | -ve | -ve | +ve | 4w |
| 21 | 4 | -ve | -ve | +ve | 4w |
| 22 | 3 | -ve | -ve | +ve | 6w |
| 23 | 3 | -ve | -ve | +ve | 6w |
| 24 | 2 | -ve | -ve | +ve | 6w |
| 25 | 2 | -ve | -ve | +ve | 5w |
Table 2: Master Table Surgical and Medical Treatment Results.
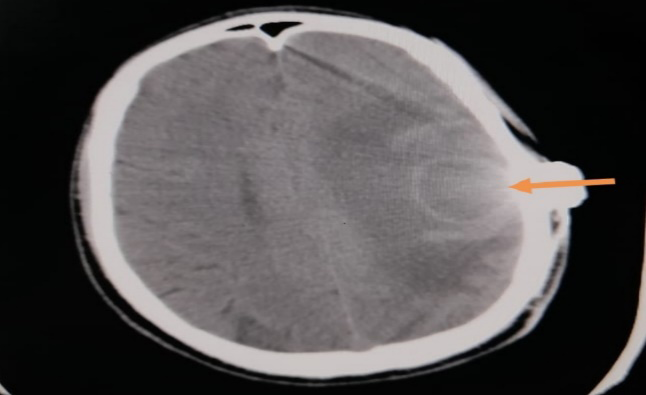
The ages of the patients ranged from 31 years old up to 60 years old. (5 women and 20 men) All patients presented to the outpatient clinic with nonspecific headache, nausea or vomiting, fever, epilepsy, and or cranial nerve affection. Full neurological examinations were conducted on all patients followed by doing CT, and or MRI brain (to rule out space occupying lesions other than brain abscess). Most of the cases diagnosed by CT brain except in patients with other brain lesions confusing with brain abscess like brain tumors, MRI brain was the first choice for differential diagnosis [7]. All diagnosed intraparenchymal pyogenic brain abscesses are included in this study with exclusion of other lesions looks like brain abscess such as: Intracerebral bleed, Ischemic stroke, and Non-infectious space--occupying lesion (e.g., brain tumor). All patients have no immunological diseases except for 3 patients presented by multiples brain abscess and were drugs addict. The existence of perilesional brain edema and its types (minimal, moderate, or severe), with or without midline shift (less than 5 mm, or more), and the brain abscess size in mm or in cm are used as a predictor for radiological measurement and for follow up. In addition, Leukocyte count, serum C-reactive protein level, and erythrocyte sedimentation rate are for laboratory evaluation and follow up. In the earlier phases, a non-contrast CT
may show only low-attenuation abnormalities with a mass effect which confused with other brain lesions [8]. Ring enhancement is virtually always present in late phases [9]. In this study, the same protocols for follow-up as in literature were followed. The most frequently isolated organisms are viridians streptococci and Staphylococcus aureus.
Results
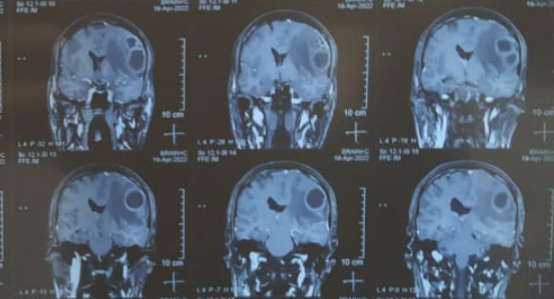
Twenty-five patients were included in this study with various stages of brain abscess from January 2018 to January 2023 in our institution. The patients age ranged from 31 years old up to 60 years old (5 women (20%), and 20 men (80%)). They presented in the outpatient clinic complaining of headache (100%), nausea or vomiting (5%). Fever (10%), epilepsy (5%), and cranial nerves affection (5%). Abscess were diagnosed by CT brain in most cases except in cases confusing with other brain lesions, MRI brain was the first choice for deferential diagnosis especially in the stage of cerebritis. All patients had a CT brain (100%) and (50%) had MRI with CT. The site of brain abscess was different depending on source of infection where (40%) were temporal, (20%) frontal, (20%) parietal, (10%) frontoparietal, (10%) multiple. In 60% of the patients the source of infection was suggested clinically to be an inner ear pathology like otitis media, and the other sources were non-specific. The size of the abscess was different, ranging from few mm in cerebritis stage to more than 2X2 cm in late stages. All the patients had routine laboratory investigations in the form of complete CBC, electrolyte, CRP, ESR. All patients had standard medical treatment with triple intravenous antibiotics therapy, and non-steroidal anti-inflammatory medications in the cerebritis stage and for 4 weeks after surgery. The antibiotics used were broad spectrum antibiotics which changed after culture and sensitivity obtained from the abscess. The empirical antibiotics coverage used were third-generation cephalosporin (Cefotaxime or Ceftriaxone 2gm every 24 hrs.), Metronidazole 500 mg q 8 hrs., plus Vancomycin 15-20

mg/kg (divided Q12H), theses “triple high dose” antibiotics used intravenously for 4 weeks followed by one weeks after aspiration of the abscess followed by oral antibiotics for another 4 weeks. Mature pyogenic brain abscesses are hypointense on T1-weighted, and hyperintense on T2- weighted MR images. While they display an isointense or slightly hyperintense rim on unenhanced T1- weighted images and a hypointense rim on unenhanced T2-weighted images, they show well-defined peripheral rim enhancement on postcontrast T1-weighted images. CT scan was ordered every 2 weeks for one month then followed by monthly CT after discontinuation of antibiotic therapy until the complete resolution of the abscess (2-3 months). An immediate CT scan is ordered if any deterioration is detected or if no clinical improvement despite a full course of therapy. History of middle ear infections, chronic otitis media were found to be the most common causes of brain abscess which are diagnosed clinically. All the patients have temporary clinical improvement with continuous medical treatment with antibiotics and nonsteroid anti-inflammatory, then they deteriorate again even with continuous medications. While after surgical aspiration, all the patients have dramatic radiological, clinical and laboratory improvement (100%) without recurrence of the symptoms, except in cases of multiple brain abscess. No radiological improvement was found during the period of medical treatment.
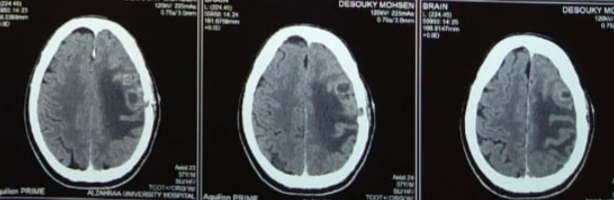
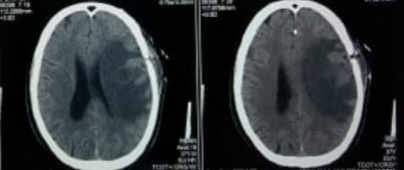
The radiological improvement was detected in the CT, and MRI brain by reduction of size of abscess, and or disappearance of the edema. The duration of disappearance of the abscess and brain oedema after aspiration ranged from 2 to 4 weeks and the hospitalizations time ranged from 4 – 6 weeks according to the patient improvement. The culture of abscesses for aerobic, anaerobic, acid-fast organisms’ fungi, and Gram stain were done where some results show nonspecific organisms (20%) (Figures 1-5).
Discussion
Pyogenic brain abscess is a focal collection of pus within the brain. The incidence of pyogenic brain abscesses is 8% of intracranial masses in the developing countries, whereas in the West the incidence is 1% to 2%, with male predominance [10]. The condition is rare because of the brain natural resistance to infection, its abundant vascular supply, and the relative impermeability of the blood–brain barrier [11]. The source of infection of brain abscess is different it can arise by extension of contiguous infections [12], penetrating head injury [13], neurosurgical procedures, or hematogenous spread from distant extracranial sources. Previous studies in a developing country reported otitis media as the most common source of intracranial suppuration [14]. In our study there were no changes of the source of infection relative to other studies. Gram-positive bacteria (GPB) cause most brain abscesses, specifically, streptococci (aerobic, anaerobic, and microaerophilic) in 30–60% and staphylococci in 10-20% [15]. In comparison, enteric gram-negative bacteria (GNB) account for 23–33% of cases [16]. In our study the most frequently isolated organisms were viridians streptococci and Staphylococcus aureus as found in other literatures [17]. In the pediatric patient group, the most common predisposing factor is congenital heart disease or adjacent cranial infection [18, 19]. While in this study, pediatric patients were not available. The source of infection may be unidentified in 25–38% of cases, with the resulting brain abscesses classified as “cryptic” [20, 21]. In our study 40% of patients were found without finding the source of infection and treated as pyogenic brain abscess.
Regarding the age predilection individuals older than 40 years are more susceptible to brain abscess [22], whereas other studies revealed that brain abscess occurs more often in individuals younger than 40 years [23] Brain abscesses were found in younger patients (less than 35 years old) especially in addict patients in our study.
The penetration of antibiotics from the systemic circulation into brain tissue is complex due to presence of blood–brain barrier and the blood-CSF barrier. Thus, the penetration of drugs into CSF, brain tissue, and other tissues are different. So, concentrations of antibiotics in plasma cannot be used to predict the concentrations of these agents in brain tissue or intracranial pus. One of the factors which limit the penetration of antimicrobial to the brain abscess is that the capillary bed of the choroid plexus, non-fenestrated meninges, and all organic compounds pass through a lipid membrane, this defense mechanism affect antibiotics absorption by the brain. Other factors that give negative effects of antimicrobial prophylaxis are resistant organisms, inadvertent slackening of aseptic discipline, idiosyncratic reactions to the drug [24]. According to the “Infection in Neurosurgery’’ Working Party of The British Society for Antimicrobial Chemotherapy,” the guiding principles for surgical management are: To urgently reduce raised intracranial pressure, to confirm the diagnosis, to obtain pus for microbiological diagnosis, to enhance the efficacy of antibiotic therapy [25]. In our study and other research, brain abscess surgeries are the preferred method of treatment [26], because it provides rapid relief of raised intracranial pressure, easy to perform, and helps to increase the effect and work of antibiotics. And the main disadvantages are repeated procedures for multiple brain abscess [27].
The mortality rates reported have varied between 1% - 32% [28]. The mortality rates reported in recent large case series are in the range of 8%-25% [29, 30, 31] while after aspiration of the abscess the mortality rate was zero in our study.
Limitations
This study has many limitations. First, the sample size was small. Second, it was a retrospective, single-center study. Therefore, multicenter studies with larger samples should be conducted in the future.
Conclusion
The gold standard treatment of pyogenic brain abscess is surgical intervention. Medical treatment in the form of specific or non-specific antibiotics could be helpful for reducing the clinical and laboratory effects of brain abscess, but it is not considered as a definitive cure.
References
-
Menon S, Bharadwaj R, Chowdhary A, Kaundinya DV, Palande DA (2008) Current Epidemiology of Intracranial Abscesses: A Prospective 5-Year Study. J Med Microbiol 57: 1259-1268.
-
Wiwanitkit S, Wiwanitkit V (2012) Pyogenic Brain Abscess in Thailand. N Am J Med Sci 4(6): 245-248.
-
Carpenter J, Stapleton S, Holliman R (2007) Retrospective Analysis of 49 Cases of Brain Abscess and Review of the Literature. Eur J Clin Microbiol Infect Dis 26(1): 01-11.
-
Mathisen GE, Johnson JP (1997) Brain Abscess. Clin Infect Dis 25(4): 763‑779.
-
Gadgil N, Chamoun RB, Gopinath SP (2012) Intraventricular Brain Abscess. J Clin Neuroscie 19(9): 1314‑1316.
-
Kao PT, Tseng HK, Liu CP, Su SC, Lee CM (2003) Brain Abscess: Clinical Analysis of 53 Cases. J Microbiol Immunol Infect 36(2): 129-136.
-
Yamamoto M, Jimbo M, Ide M (1993) Penetration of Intravenous Antibiotics into Brain Abscess. Neurosurgery 33(1): 44-49.
-
Muzumdar D, Jhawar S, Goel A (2011) Brain Abscess: An overview. Int J Surg 9(2): 136-144.
-
Salzman C, Tuazon CU (1987) Value of the Ring-Enhancing Sign in Differentiating Intracerebral Hematomas and Brain Abscesses. Arch Intern Med 147(5): 951-952.
-
Carpenter J, Stapleton S, Holliman R (2007) Retrospective Analysis of 49 Cases of Brain Abscess and Review of the Literature. Eur J Clin Microbiol Infect Dis 26(1): 1-11.
-
Cunha BA (2001) Central Nervous System Infections in the Compromised Host: A Diagnostic Approach. Infect Dis Clin North Am 15(2): 567-590.
-
Brydon HI, Herdwide C (1994) The Management of Cerebellar Abscess Since the Introduction of CT Scanning. Br J Neurosurg 8(4): 447-455.
-
Patri R, Sood S, Bathia R (1995) Post Traumatic Brain Abscess Experience of 36 Patients. Br J Neurosurg 9(1): 29-35.
-
Zhang C, Hu L, Wu X, Hu G, Ding X, et al. (2014) A Retrospective Study on the Aetiology, Management, and Outcome of Brain Abscess in an 11-Year, Single-Centre Study from China. BMC Infect Dis 14: 311.
-
Brouwer MC, Beek DVD (2017) Epidemiology, Diagnosis, and Treatment of Brain Abscesses. Curr Opin Infect Dis 30(1): 129-134.
-
Campioli CC, Almeida NEC, Ohoro JC, Garrigos ZE, Wilson WR, et al. (2021) Bacterial Brain Abscess: An Outline for Diagnosis and Management. Am J Med 134(10): 1210- 1217.
-
Calfee DP, Wispelwey B (2000) Brain Abscess. Semin Neurol 20(3): 353-360.
-
Agrawal D, Suri A, Mahapatra AK (2003) Primary Excision of Pediatric Posterior Fossa Abscesses--Towards Zero Mortality? A Series of Nine Cases and Reviews. Pediatric Neurosurg 38(2): 63-67.
-
Sankararaman S, Romero RRM, Gonzalez TE (2012) Brain Abscess from a Peritonsillar Abscess in an Immunocompetent Child: A Case Report and Review of the Literature. Pediatric Neurol 47(6): 451-454.
-
Tseng JH, Tseng MY (2006) Brain Abscess in 142 Patients: Factors Influencing Outcome and Mortality. Surg Neurol 65(6): 557-562.
-
Lu CH, Chang WN, Lui CC (2006) Strategies for the Management of Bacterial Brain Abscess. J Clin Neurosci 13(10): 979-985.
-
Amornpojnimman T, Korathanakhun P (2018) Predictors of Clinical Outcomes among Patients with Brain Abscess in Thailand. J Clin Neurosci 53: 135-139.
-
Moorthy RK, Rajshekhar V (2008) Management of Brain Abscess: An Overview. Neurosurg Focus 24(6): E3.
-
Lu CH, Chang WN, Lui CC (2006) Strategies for the Management of Bacterial Brain Abscess. J Clin Neurosci 13(10): 979-985.
-
Louvois JD, Brown EM, Bayston R, Lees PD, Pople IP (2000) Infection in Neurosurgery Working Party of the British Society for Antimicrobial Chemotherapy. The Rational Use of Antibiotics in the Treatment of Brain Abscess. Br J Neurosurg 14(6): 525‑530.
-
Nathoo N, Narotam PK, Nadvi S, Van Dellen JR (2012) Taming an Old Enemy: A Profile of Intracranial Suppuration. World Neurosurg 77(3): 484-490.
-
Hall WA, Truwit CL (2008) The Surgical Management of Infections Involving the Cerebrum. Neurosurgery 62(S2): 519-530.
-
Kao PT, Tseng HK, Liu CP, Su SC, Lee CM (2003) Brain Abscess: Clinical Analysis of 53 Cases. J Microbiol Immunol Infect 36(2): 129-136.
-
Carpenter J, Stapleton S, Holliman R (2007) Retrospective Analysis of 49 Cases of Brain Abscess and Review of the Literature. Eur J Clin Microbiol Infect Dis 26(1): 1-11.
-
Hakan T, Ceran N, Erdem I, Berkman MZ, Goktas P (2006) Bacterial Brain Abscesses: An Evaluation of 96 Cases. J Infect 52(5): 359-366.
-
Xiao F, Tseng MY, Teng LJ, Tseng HM, Tsai JC (2005) Brain Abscess: Clinical Experience and Analysis of Prognostic Factors. Surg Neurol 63(5): 442-450.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury