Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
Fluoride helps prevent tooth decay by forming fluoroapatite, a compound more resistant to acid than hydroxyapatite in tooth enamel. Without fluoride, dental caries can progress to the pulp of the tooth, potentially requiring root canal treatment. In Israel, community water fluoridation was mandatory in cities with over 5,000 residents from 1998 until it was discontinued in 2014. This study examines the effect of community water fluoridation on socioeconomic disparities in dental health, focusing on the prevalence of root canal treatments in deciduous teeth among 6-year-old children. A retrospective analysis was conducted using computerized dental records from 2014–2015 (with fluoridation) and 2016–2022 (without fluoridation). The data included dental checkups and root canal treatments in deciduous teeth. Statistical significance was set at p < 0.05. Result: Showed that children from lower socioeconomic backgrounds had higher rates of root canal treatments, especially in areas without fluoridated water. In contrast, children from higher socioeconomic groups had relatively stable treatment rates regardless of fluoridation status. Across all groups, boys had more root canal treatments than girls. Conclusion: Community water fluoridation can reduce socioeconomic disparities by reducing the incidence of root canal treatment in deciduous teeth.
Chana SZ¹*, Jonathan M¹, Guy T¹, Mordechai F², Doron H² and Tali C³
¹Department of Community Dentistry, Hebrew University of Jerusalem, Israel ²Dental Research Unit – Maccabi-Dent, Maccabi Healthcare Fund, Israel ³Department of Periodontology, Hebrew University of Jerusalem, Israel
Abbreviations
CWF: Community Water Fluoridation; OHRQoL: Overall Quality of Life.
Background
The Structure of Teeth: From Eruption to Decay and Treatment
The human oral cavity has 20 deciduous teeth, usually emerging between 8 and 31 months [1, 2]. In 6-year-old
children, the deciduous teeth have been in the mouth for about 3 to 5 years, and at this age, the process of their replacement with permanent teeth begins [3].
The tooth has three layers. The outer layer is the hardest, mostly made of hydroxyapatite. The dentin layer is in the middle, also mostly made of hydroxyapatite [4, 5]. The innermost layer - the tooth pulp contains nerves, blood vessels, and other living cells [6].
Tooth decay is the most common chronic disease in the world. It occurs when bacteria metabolize sugars to create acids that cause demineralization. The acid combines with a base in the hydroxyapatite crystal, breaking down the enamel [7]. Caries in the enamel and dentin can be treated by removal of the bacteria and reconstruction of the tooth structure and function [8].
When the decay is deep and reaches the pulp of the tooth, it is necessary to perform a root canal treatment. This treatment includes the debridement of the canal by chemical and mechanical means and sealing to prevent the passage of microorganisms and fluids through the apex. In this way, the function of the tooth is preserved [9].
The Impact of Dental Caries
Dental pain, a prevalent issue among preschool children, significantly affects daily activities, school performance, and overall quality of life (OHRQoL). In Capão do Leão, Brazil, a cross-sectional study evaluated the prevalence of dental pain in children aged 2–5 years and its association with caries severity, dental trauma, and maternal perception of OHRQoL.
Findings revealed a 14.5% prevalence of dental pain, primarily linked to untreated carious dentin lesions, pulp involvement, and abscesses. Children with severe caries stages experienced more dental pain, often requiring invasive treatments like restorations, pulp therapy, or extractions. Dental pain negatively impacted all domains of OHRQoL, highlighting the importance of preventive strategies and timely interventions [10].
Fluoride
Fluoride occurs naturally in a range of animal-derived foods, and plants, and can also be found in natural drinking water [11]. In Israel, the amount of natural fluoride in drinking water is approximately 0.3 Parts Per Million (PPM), and there is no fluoride in desalinated water [12].
Community water fluoridation (CWF) to improve oral health has a long history with significant scientific support [11, 13, 14, 15, 16]. Fluoride replaces the hydroxyl group in the tooth hydroxyapatite, forming fluorapatite that resists acid from food and bacteria, thus preventing decay. Fluoride also accelerates the deposition of minerals in the enamel, reducing the risk of decay. Some studies suggest fluoride can arrest tooth decay [11].
Fluoride reaches the teeth through the systemic circulation mainly from CWF, and ingestion of processed foods and drinks. It is also applied topically by various products, such as dentifrices [17].
Fluoride Efficacy in Previous Studies
Global and Israeli health authorities recommend that the optimal range of water fluoridation concentration in order to significantly decrease caries incidence is 0.7-1.0 mg for those consuming fluoridated water from infancy [18].
In 2012, a study conducted at the Hebrew University in Israel showed a 29% decrease in caries morbidity in a city with optimized water fluoride concentration compared to a city with insufficient levels [18].
In 2014, a New Zealand report confirmed that water fluoridation decreased caries rate, especially in high-risk groups, saved healthcare costs, and posed no significant health risks [15]. A 2022 study in Israel observed a notable rise in restorative dental treatments among children following the cessation of CWF, in 2014 based on data from “Maccabi-Dent” clinics [16].
The Reform in Israel
In 1998, Israel introduced regulations requiring fluoridation of drinking water in cities with over 5,000 inhabitants. The regulations took effect in 2002, and approximately 70% of the population benefited from fluoridated water by 2012. However, in August 2014, the law was repealed, prohibiting external fluoridation of drinking water in Israel [12, 18].
In 2002, a survey in Israel revealed a socio-economic gap in caries morbidity among 12-year-old children. In 2010, dental health reform was initiated, offering free preventive dental treatments and retainers with financial deductibles for children up to age 8, aiming to narrow the morbidity gap.
A 2012 study post-implementation showed reduced differences between socio-economic levels, though disparities persisted [19, 20]. The reform has since expanded, providing free or financial deductible dental treatment for children up to the age of 18 and adults over 72 [20].
Maccabi-Dent
The “Maccabi” Health Fund founded in 1940 is the second largest in Israel and has approximately 2.6 million members. It’s dental chain, “Maccabi-Dent”, has 59 dental clinics nationwide, with 461 dental units, and about 1400 dentists, including specialists from all disciplines. “Maccabi- Dent”, treats all strata of the population.
In this study, we examined the effect of the cessation of CWF by comparing the number of root canal treatments performed on all deciduous teeth in 6-year-old children between 2014-2015 to the number in 2016-2022. We also examined socio-economic status and gender.
The Rationale of this Study
The main aim is to examine how the cessation of CWF affects socio-economic disparities in caries morbidity by examining the effect of fluoride cessation on the incidence of root canal treatments- secondary objective.
Methods
The study was approved by the Review Board (IRB) MHS-0157020 and The Helsinki committee of Maccabi Healthcare Services. The study population included children aged 6 from all over Israel who are in the “Maccabi” Health Fund from the whole spectrum of the population.
The comparison was made between the number of root canal treatments performed on deciduous teeth between the years 2014-2015 and the years 2016-2022 following the cessation of CWF in 2014. In addition, a comparison was made according to socio-economic status.
The data was examined retrospectively from the electronic records of the “Maccabi-Dent” clinics in Israel. “Maccabi-Dent” dentists are remunerated by the Fee for Service method; thus, each procedure has a treatment code, and codes are recorded for all treatments.
We also classified the treatments based on the socioeconomic status determined according to the list of districts and socio-economic clusters, formulated by the Central Bureau of Statistics in 2015. This list has 9 socioeconomic levels, 1-3 represents a low socio-economic level, 4-6 represents medium and 7-9 represents high [21]. In this study, we collected data regarding check-ups and root canal treatments in deciduous teeth in 6-year-olds. SPSS statistics software version 27.0. was used.
Statistical tests were used to compare the independent variables: fluoride levels in the water, socio-economic status, and gender, to the dependent variable: the number of root canal treatments performed on deciduous teeth among 6-year-olds.
The following comparisons were made:
- Root canal treatment rate for each socio-economic level.
- Root canal treatment rate with and without CWF.
- Root canal treatment rate for each socio-economic group taking into account CWF.
- Root canal treatment rates in different socio-economic groups and gender.
Results
Sample size: 8,007 children from all over Israel and from the whole spectrum of the population. 4097 males (51%), 3910 females (49%). All deciduous teeth were examined and evaluated. Various analyses were performed, as presented in the following graphs.
Analysis of the rate of root canal treatments as a function of socio-economic level (Figure 1), showed an inverse correlation: as the socio-economic level increased, the rate of root canal treatments decreased.
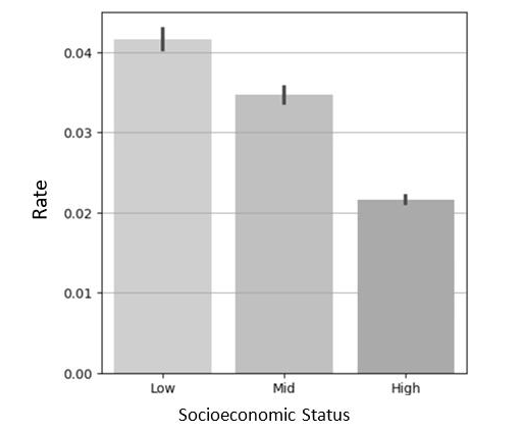
The results of Levene’s test for equality of variances were statistically significant (stat=396.56, p= 6.06e-165), indicating that the variances were not equal.
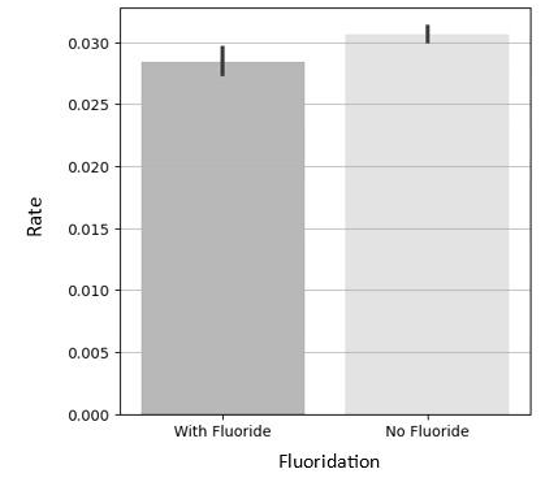
As a result, we conducted Welch’s F-test for unequal variances ANOVA, which revealed a significant difference among the conditions, with a large effect size (Partial eta- squared=0.13) (Figure 2).
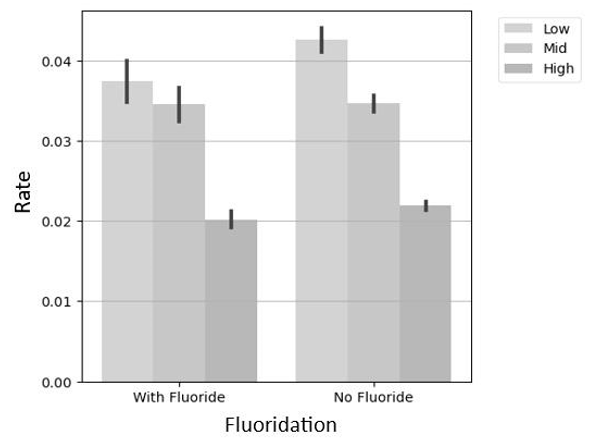
In the presence of CWF, no statistically significant difference between low and mid-socio-economic levels were found regarding the rate of root canal treatments (Figure 3). However, in the absence of fluoridation, individuals with lower socioeconomic status had the most significant increase in the rate of root canal treatment (p<0.05). In addition, those with mid and high socio-economic status maintained a relatively stable root canal treatment rate regardless of the presence or absence of CWF.
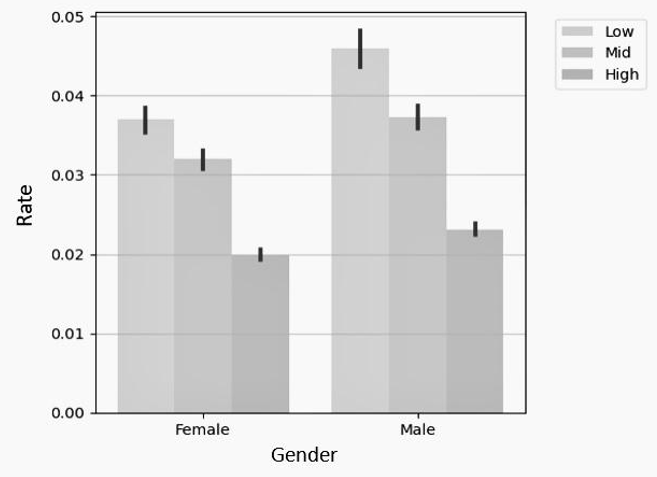
When analyzing the rate of root canal treatments as a function of socioeconomic status and gender (Figure 4), we found that males, across all three socio-economic levels, had more root canal treatments than females (p<0.05). Furthermore, for both genders, a significant correlation showed that as socioeconomic status improved, the number of root canal treatments decreased (p<0.05).
Discussion
The effect of CWF cessation on the rate of root canal treatments among 6-year-old children and the ability of fluoridation to reduce socio-economic disparities were examined by comparing two periods: 2014-2015 and 2016- 2022. These periods were selected based on the timing of the initiation of CWF in Israel in 1998, its legal inclusion in 2002, and its removal from legislation in 2014.
Children aged 6 in 2014 were born in 2008 and therefore exposed to CWF throughout their lives, including prenatally, we assumed similar exposure in children 6 years of age in 2015. Conversely, 6-year-olds between 2016-2022 were exposed to CWF for a maximum of 2 years or not at all. The choice of 6-year-old children for this study was deliberate, taking into consideration that their deciduous teeth will remain in the mouth for approximately 3 to 5 additional years. The data shows incidence in order to highlight the rate of new cases of root canal treatments within a specified period.
The significant results of the current study are congruent with published findings. 1. Less root canal treatments were performed in children from a higher socio-economic status and the converse was also found to be true. These results were noted in other studies: A 1997 South African review of 6, 12, and 15-year-olds, children from urban families with higher socio-economic levels had lower rates of dental caries [22]. A Canadian study from 2014 found that higher-income individuals required less dental care, underscoring the need to improve access to dental care for low-income populations [23]. A 2021 study in China revealed that lower parental education and household income were significantly linked to a higher incidence of dental caries in preschool children [24].
This finding can be at least partly explained by a 2005 study from the USA that showed that individuals with low income and education levels consume a diet high in added sugar [25].
Another possible explanation is that those with higher socio-economic status (characterized by high income and education levels) tend to exhibit greater consistency in maintaining oral hygiene practices. Good oral hygiene contributes to lower rates of caries morbidity, providing another perspective on the observed differences in caries experience in socio-economic groups [26, 27].
2. The rate of root canal treatments is lower with CWF than without CWF. Similar results were observed in other studies: A 2015 review found that community water fluoridation reduced caries indices and increased the percentage of caries-free children by 15% in deciduous teeth and 14% in permanent teeth [28]. In a 2021 study in Brazil, children and adolescents using fluoridated water showed a lower prevalence and severity of dental caries compared to those relying solely on fluoridated toothpaste [29]. The mechanism underlying these findings lies in fluoride’s ability to replace the hydroxyl group in enamel hydroxyapatite, forming fluoroapatite—a compound that resists acid from food and bacteria, thereby preventing decay. Additionally, fluoride accelerates mineral deposition in the enamel, further reducing the risk of caries, and some studies even suggest its potential to arrest tooth decay [11].
When deep dental decay occurs, it may reach the tooth’s pulp, necessitating root canal treatment. By preventing the onset of decay in the first place, we can avoid the need for root canal procedures altogether [9].
3. Those most affected by the cessation of CWF had low socio- economic status, with a significant increase in the rate of root canal treatments performed. In children with mid and high socioeconomic status, the number of root canal treatments performed remained relatively stable with and without CWF.
These findings may be clarified by the observation that affluent populations do not necessarily need water fluoridation to maintain oral health.
Studies reveal that individuals from high socioeconomic status are the least impacted by the absence of community water fluoridation (CWF) [30, 31, 32]. This could be attributed to their economic capacity, enabling them to consume healthier foods [25], gain access to treatments, and maintain oral hygiene [33].
In contrast, populations with low-income levels often lack these resources, underscoring the importance of fluoridation for them. We assume that in the absence of alternative means, CWF plays a vital role in promoting oral health within communities with low socio-economic status [33].
4. For all socio-economic levels, more root canal treatments were performed in boys compared to girls. These finding contrasts other studies that show that more dental treatments are performed in females than males [34, 35, 36].
Our findings can be interpreted in various ways: A. The disparity in treatment frequency between genders is influenced by age:
According to a 2015 study in the USA, there were no significant gender differences in dental treatments in children aged 1-5. However, girls aged 6-11 exhibited 1.5 fewer affected teeth than boys. In the 12-17 age group, caries rates were similar in girls and boys. Among adults (18-59 years), females had more dental restorations, while males had a higher incidence of current decay [37].
B. Boys are more susceptible to dental trauma at early ages compared to girls:
A retrospective study in Greece in 2021 revealed that children experience dental trauma more frequently at ages 5, 7, and 11, with boys being more prone to dental injuries and receiving more treatment at a young age [38].
C. Additionally, a 2021 review revealed that men often neglect oral health, showing poorer hygiene habits and facing higher risks of gum disease and oral cancer. They tend to seek dental care for immediate issues rather than preventive care. In contrast, women generally exhibit better oral health behaviors and attitudes [39].
Limitations
1. We relied on a database that provided treatment records without diagnoses, assuming that there were appropriate indications for the treatments performed. However, in fee-for-service payment systems like “Maccabi-dent,” the accuracy of treatment codes in patients’ records might not be completely accurate. 2. Numerous children undergo dental examinations, but difficulties with cooperation often result in referrals for treatment. “Maccabi Dent,” has a specialized clinic at Assuta Hospital for children aged 1-5 and sometimes older, where treatments are administered exclusively under general anaesthesia. This clinic treats children from across the entire country, and no records are kept regarding their socio-economic status. Consequently, we excluded records from this clinic. While acknowledging this exclusion as a limitation in our analysis, incorporation of the data from this clinic into our calculations could have strengthened our argument, as there was a notable increase in the overall number of root canal treatments performed.
Conclusion
Community water fluoridation can reduce socio- economic disparities by reducing the incidence of root canal treatment in deciduous teeth among 6-year-old children.
Ethical Approval
The present study was approved by the Review Board (IRB) MHS-0157020 The Helsinki committee of Maccabi Healthcare Services.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Competing Interests
The authors declare that they have no competing interests.
Funding
Self-Financing.
Author’s Contribution
SC, TG, MJ – Conception and design of the study, analysis of the data, writing, reviewing, and editing. FM – Conception and design of the study, data curation CT – supervision and methodology HD – Conception and design of the study, data curation
Acknowledgements
Not Applicable.
References
-
Aruede G, Pepper T (2023) Anatomy, Permanent Dentition. In: StatPearls. Treasure Island (FL): StatPearls Publishing.
-
Li RX, Hu Y (2017) A Cross-Sectional Survey on the Patterns of Primary Teeth Eruption in 2 581 Children. Zhonghua er ke za zhi = Chinese Journal of Pediatrics 55(1): 37-41.
-
Karki RK (2016) Eruption Pattern of Dentition and Its Medico-legal Significance. Kathmandu University Medical Journal (KUMJ) 14(54): 103-106.
-
Ruan Q, Moradian-Oldak J (2015) Amelogenin and Enamel Biomimetics. J Mater Chem B 3: 3112-3129.
-
Grawish ME, Grawish LM, Grawish HM, Grawish MM, Holiel AA, et al. (2022) Demineralized Dentin Matrix for Dental and Alveolar Bone Tissues Regeneration: An Innovative Scope Review. Tissue Engineering and Regenerative Medicine 19(4): 687-701.
-
Ghannam MG, Alameddine H, Bordoni B (2023) Anatomy, Head and Neck, Pulp (Tooth). In: StatPearls. Treasure Island (FL): StatPearls Publishing.
-
Neel EAA, Aljabo A, Strange A, Ibrahim S, Coathup M, et al. (2016) Demineralization-Remineralization Dynamics in Teeth and Bone. Int J Nanomedicine 11: 4743-4763.
-
John Schrefer, Penny Rudolph (2002) Sturdevant’s Art & Science of Operative Dentistry, Mosby.
-
Hui KC, Chen NN, Koh ET, Lam EC, Lim KC, et al. (2004) The Society of Endodontists, Guidelines for Root Canal Treatment. Singapore Dent Journal 26(1): 60-62.
-
Fernandez MS, Pauli LA, Araújo ABG, Demarco GT, Azevedo MS, et al. (2024) Dental Pain in Brazilian Preschool Children: Association with the Severity of Dental Caries and Impact on Oral Health-Related Quality of Life. European Archives of Paediatric Dentistry 25(4): 481-490.
-
Medjedovic E, Medjedovic S, Deljo D, Sukalo A (2015) Impact of Fluoride on Dental Health Quality. Mater Sociomed 27(6): 395-398.
-
Mann, et al. Petition to the High Court.
-
Senevirathna L, Ratnayake HE, Jayasinghe N, Gao J, Zhou X, et al. (2023) Water fluoridation in Australia: A Systematic Review. Environmental Research 237(Pt 1): 116915.
-
Zokaie T, Pollick H (2022) Community Water Fluoridation and the Integrity of Equitable Public Health Infrastructure. Journal of Public Health Dentistry 82(3): 358-361.
-
Royal Society of New Zealand and the office of the Prime Minister’s Chief Science Advisor, Health Effects of Water Fluoridation: A Review of the Scientific Evidence.
-
Tobias G, Findler M, Chackartchi T, Bernstein Y, Grinberg BC, et al. (2022) The Effect of Community Water Fluoridation Cessation on Children’s Dental Health: A National Experience. Israel Journal of Health Policy Research 11(1): 4.
-
Carey CM (2014) Focus on Fluorides: Update on the Use of Fluoride for the Prevention of Dental Caries. Journal of Evidence Based Dental Practice 14: 95-102.
-
(2019) Ministry of Health, Division of Dental Health, Facts about Drinking Water Fluoridation.
-
Mann (2020) Ministry of Health, Oral and Dental Health in Israel. Goals for a Healthy Future.
-
(2023) Ministry of Health, Expansion of Litzman’s Dental Treatment Reform.
-
(2015) List of Authorities by Districts and Socio- Economic Clusters Cluster, in Alphabetical Order According to the Central Bureau of Statistics.
-
Plessis JBD (1997) The Effect of Socio-Economic Status on Dental Caries Experience in 6, 12 and 15-Year-Old School Children in Port Elizabeth and Despatch. The Journal of the Dental Association of South Africa 52(7): 483-486.
-
Duncan L, Bonner A (2014) Effects of Income and Dental Insurance Coverage on Need for Dental Care in Canada. J Can Dent Assoc 80: e6.
-
Zhang T, Hong J, Yu X, Liu Q, Li A, et al. (2021) Association between Socioeconomic Status and Dental Caries among Chinese Preschool Children: A Cross-Sectional National Study. BMJ Open 11(5): e042908.
-
Thompson FE, McNeel TS, Dowling EC, Midthune D, Morrissette M, et al. (2009) Interrelationships of Added Sugars Intake, Socioeconomic Status, and Race/ Ethnicity in Adults in the United States: National Health Interview Survey, 2005. Journal of the American Dietetic Association 109(8): 1376-1383.
-
Fernando C, Ha DH, Do LG, Tadakamadla SK (2023) Socioeconomic Status and Toothbrushing in Indigenous and Non-Indigenous Australian Children. JDR Clinical & Translational Research 8(2): 139-147.
-
Trinh VA, Tarbit E, Do L, Ha D, Tadakamadla SK (2021) The Influence of Family Socioeconomic Status on Toothbrushing Practices in Australian Children. Journal of Public Health Dentistry 81(4): 308-315.
-
Iheozor-Ejiofor Z, Worthington HV, Walsh T, O’Malley L, Clarkson JE, et al. (2015) Water Fluoridation for the Prevention of Dental Caries. Cochrane Database of Systematic Reviews 10(10): CD010856.
-
Silva MCC, Lima CCB, Lima MDM, Moura LFAD, Tabchoury CPM, et al. (2021) Effect of Fluoridated Water on Dental Caries and Fluorosis in Schoolchildren who Use Fluoridated Dentifrice. Brazilian Dental Journal 32(3): 75-83.
-
Evans RW, Beck DJ, Brown RH, Silva PA (1984) Relationship between Fluoridation and Socioeconomic Status on Dental Caries Experience in 5-year-old New Zealand Children. Community Dentistry and Oral Epidemiology 12(1): 5-9.
-
Slade GD, Spencer AJ, Davies MJ, Stewart JF (1996) Influence of Exposure to Fluoridated Water on Socioeconomic Inequalities in Children’s Caries Experience. Community Dentistry and Oral Epidemiology 24(2): 89-100.
-
McLaren L, McNeil DA, Potestio M, Patterson S, Thawer S, et al. (2016) Equity in Children’s Dental Caries before and after Cessation of Community Water Fluoridation: Differential Impact by Dental Insurance Status and Geographic Material Deprivation. International Journal for Equity in Health 15(24).
-
Northridge ME, Kumar A, Kaur R (2020) Disparities in Access to Oral Health Care. Annu Rev Public Health 41: 513-535.
-
Lukacs JR, Largaespada LL (2006) Explaining Sex Differences in Dental Caries Prevalence: Saliva, Hormones, and “Life-History” Etiologies. American Journal of Human Biology 18(4): 540-555.
-
Walter BS, DeWitte SN, Redfern RC (2016) Sex Differentials in Caries Frequencies in Medieval London. Archives of Oral Biology 63: 32-39.
-
Lukacs JR (2011) Sex Differences in Dental Caries Experience: Clinical Evidence, Complex Etiology. Clinical Oral Investigations 15(5): 649-656.
-
Shaffer JR, Leslie EJ, Feingold E, Govil M, McNeil DW, et al. (2015) Caries Experience Differs between Females and Males across Age Groups in Northern Appalachia. International Journal of Dentistry.
-
Agouropoulos A, Pavlou N, Kotsanti M, Gourtsogianni S, Tzanetakis G, et al. (2021) A 5-Year Data Report of Traumatic Dental Injuries in Children and Adolescents from a Major Dental Trauma Center in Greece. Dental Traumatology 37(4): 631-638.
-
Lipsky MS, Su S, Crespo CJ, Hung M (2021) Men and Oral Health: A Review of Sex and Gender Differences. American Journal of Men’s Health 15(3): 15579883211016361.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells
- Treatment of Temporomandibular Disorder and Orofacial Pain in Unified Health System in Brazil