Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
Excessive gingival display, an esthetically concerning clinical situation is characterized by an excessive display of gums during a normal smile. Etiology of the condition is multifactorial involving altered passive eruption, vertical maxillary excess, hypermobile upper lip or short upper lip. Hypermobile upper lip is prevalent among north Americans and Asians. Management of the hypermobility may involve non-surgical or surgical methods. The use of botulinum toxin as a non-surgical approach is widely popular, although with the primary disadvantage of being short lived and requiring frequent reapplication. Surgical technique provides more stable results and may include myotomy that involves complete resection of muscles or the or lip repositioning surgery involving repositioning of the vestibular mucosa. Reducing the vestibule depth. Lip repositioning offers the primary advantage of being less invasive and is reversible. This article describes a case report of management of excessive gingival display due to hypermobile upper lip using a modified lip repositioning surgery where in the midline labial frenum is left intact, thus significantly improving the esthetic results.
Abbreviations
EGD: Excessive Gingival Display; VME: Vertical Maxillary Excess.
Introduction
Excessive gingival display (EGD) refers to overexposure of the gingiva during a normal smile [1]. However, in severe cases, this may be evident when the lips are in repose position. Excessive gingival display is more commonly seen in women between the age groups of 20-30 years [2]. With increasing age, the gingival display decreases due to the falling back of the lip thus resulting in less exposure of the gingiva.
The etiology of excessive gingival display is multifactorial, and an accurate diagnosis is critical in successful management of the patient. Altered passive eruption characterized by the failure of the gingival tissue to recede apically resulting in short clinical crowns is one of the etiologies of EGD [3]. The alveolar bone may be at the level of CEJ or apical to it. A classification for altered passive eruption was suggested by Coslet JG, et al. [4], which also determines the treatment strategy (Table 1).
| Classification | Clinical Feature | Treatment Protocol |
|---|---|---|
| IA | Excessive amount of keratinized gingiva with normal alveolar crest–to–CEJ relationship | Gingivectomy |
| IB | Excessive amount of keratinized gingiva with osseous crest at the CEJ level | Osseous contouring |
| 2A | Normal amount of keratinized gingiva with normal alveolar crest–to–CEJ relationship | Apically positioned flap |
| 2B | Normal amount of keratinized gingiva with osseous crest at the CEJ level | Apically positioned flap with Osseous contouring |
Table 1: Altered Passive Eruption- Classification and treatment options.
Vertical maxillary excess, (VME) commonly seen in long face syndrome involves overgrowth of the maxilla in the vertical direction, especially the lower half of the face [5]. There is harmony in the occlusal plane between the anterior and posterior segments, however the occlusal plane is lower than normal and subjects with VME have the lower lip positioned on the incisal edges of the upper incisors and an excessive display of the maxillary gingiva. Diagnosis is established by a clinical and cephalometric evaluation of the patient. The treatment approach for management of VME involves combination of periodontal, orthodontics or restorative treatment and is dictated by the amount of gingival display [6] (Table 2).
| Degree | Gingival display (in mm) | Treatment Approach |
|---|---|---|
| I | 02-Apr | Orthodontic intrusion |
| Orthodontics and periodontics | ||
| Periodontal and restorative therapy | ||
| II | 04-Aug | Periodontal and restorative therapy |
| Orthognathic surgery (Le Fort I osteotomy) | ||
| III | >8 | Orthognathic surgery with or without adjunctive periodon- tal and restorative therapy |
Table 2: Classification of vertical maxillary excess.
The length and muscular activity of the upper lip plays a significant role in the amount of gingival display. A short upper lip measuring less than 15mm from the subnasale to the philtrum may result in excessive gingival display [7]. Hyperactivity of the musculature of the upper lip, especially elevator muscles results in significant lip elevation of about 8 mm from rest. The prevalence of hypermobile upper lip among north Americans and Asians with gummy smile is more than 80%. In about 40% of these cases, they are present isolated and in another 35% they are present in conjunction with altered passive eruption [8, 9].
The treatment approaches for management of hyperactive upper lip are focused on curbing the function of the elevator muscles or physical limitation of their movement. Both non-surgical and surgical techniques are employed. One of the common non-surgical methods is use of botulinum toxin which paralyses the muscles resulting in limited movement [10]. However, the effect is short lived lasting for about 3-6 months and usually needs reapplication at regular intervals [11]. Surgical techniques include invasive procedures such as the myotomy which may involve either complete or partial resection of the levator labii superioris muscle [12] to the less invasive procedure such as the lip repositioning which reduces lip mobility through reduction of the vestibular mucosa. Myotomies can be done either via a nasal or an intra oral access and are very effective in reducing the mobility. Since the procedure involves transection or resection of the muscles, they are usually not reversible and may result in greater postoperative morbidity [13].
Lip repositioning surgery was first described in plastic surgery by Rubinstein AM, et al. [14]. However, this procedure was introduced to the dental and periodontal literature by Rosenblat A, et al. [15]. The initial technique involved removing a single band of tissue outlined by a coronal incision placed at the mucogingival junction, apical incision placed at the depth of vestibule or at a distance that is double the amount of gingival display (not more than 10-12 mm from the coronal incision) and vertical incisions positioned bilaterally at the region of second premolar or molar depending on the patient’s smile. This procedure is associated with minor postoperative complications such as pain, swelling, tension during smiling and speaking, and rarely ecchymosis, transient numbness and early relapse [16] and is usually reversible.
The original technique does not involve frenulum reconstruction which frequently was associated with distortion of the midline. A modification of the technique introduced by Silva CO, et al. [17] involves removal of 2 bands of mucosa instead of a single band thus preserving the midline maxillary frenum. Several other modifications introduced in the later years include altering the suturing technique [18], use of a physical spacer [19] to prevent relapse and the use of LASER [20].
Here we present in detail a case report of excessive gingival display due to hypermobility of upper lip, effectively managed by the Silva’s modified lip repositioning technique.
Case Report
A 20-year-old female presented with complaints of excessive display of gums during smiling and she was unhappy about it. Clinical examination revealed 7 mm of gingival display during smile (Figure 1). The central incisor measured 10 mm, with the CEJ at a mm subgingival to the gingival margin, and the alveolar bone about 2 mm from the CEJ. The harmonious relationship of the CEJ, gingival margin and the alveolar bone precluded the diagnosis of altered passive eruption. The upper lip measured 18 mm indicating normal upper lip length. The lip elevation from rest to a full smile was 7 mm. The increased exposure of the gingiva during wide smile led to the diagnosis of hypermobile upper lip and was planned for a modified lip repositioning surgery.

Incision and Partial Thickness Dissection
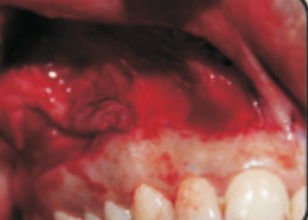
Following pre surgical rinse with 0.12% chlorhexidine, adequate anaesthesia was established by bilateral infiltration in the vestibular mucosa and upper lip between the right and the left first molar. Incision lines were marked with a sterile pencil (Figure 2). The coronal incision, a partial thickness incision was placed at the mucogingival junction on either side of the frenum leaving the frenum intact. The horizontal apical incision was placed 10 mm from the coronal incision, again leaving the frenum intact. The two horizontal incisions were connected by elliptical incisions at the mesial aspect of the right and left first molar (Figures 3a,3b). Since the patient had a very wide smile displaying the first molar, the elliptical incision lines were planned at the first molar region. Superficial partial thickness dissection was carried between the incision lines, removing 2 bands of tissue on either side of the frenum (Figure 4). Care was taken to avoid the minor salivary glands in the submucosa. Adequate hemostasis was achieved with compression.
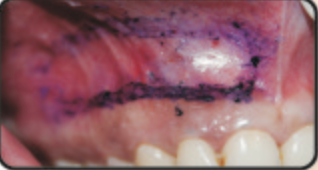
Figures 3a, 3b: Coronal and apical incisions placed and connected by distal elliptical incisions.

Suturing
After careful dissection, suturing was carried out to approximate the coronal and the apical incision lines.
Continuous interlocking sutures were placed using 4-0 polyglactone sutures (Figure 5). Care was taken to maintain tension free closure.

Post Operative Care
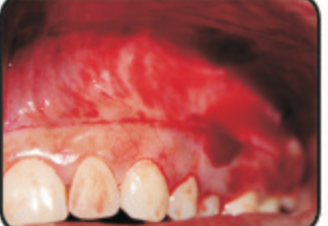
The patient was instructed to apply ice pack for several hours after the surgery. The patient was recommended soft diet for 1 week, to avoid brushing in the surgical site for about 2 weeks and to minimize lip movement during talking or smiling during the first 2 postoperative weeks. Analgesics (Ibuprofen 600 mg tid) was prescribed for managing post operative pain. Post operative rinse with chlorhexidine was recommended for 2 weeks. The sutures were removed at 2 weeks. During the post operative period, healing was uneventful. The patient reported mild pain and swelling for the first 2 days after the surgery which gradually subsided. She mentioned the notable tightness she felt during lip movement. Clinical examination revealed minimal scarring (Figure 6). The amount of gingival display significantly reduced to about 3 mm (Figure 7). The curvature of the upper lip remained unaffected with maintenance of the philtrum giving an esthetically pleasing result.


Discussion
Excessive gingival display is an esthetic concern to the patient as well as the clinician. While managing patients with EGD it is important to perform a thorough clinical and radiographic evaluation to identify the exact etiology of the gingival display which will help in the decision-making process of management thus ensuring long term success.
Lip repositioning surgery has shown to decrease gingival display and increases vermillion length during smile without altering the vertical dimensions of lip at rest in patients with hypermobile upper lip Though a simple procedure, it has shown evidence of some partial relapse which is dictated by the surgical technique and the patient selection. Systematic review evaluating the efficacy of the lip repositioning surgery [21] have concluded that this procedure results in 3-4 mm of gingival display reduction when evaluated over a period of 36 months.
In this case, the modified technique resulted in about 5 mm of reduction of gingival display. The utilization of the modified technique preserved the frenum thus maintaining the curvature of the lip and helped to achieve good esthetic results.
Conclusion
Surgical management of the hypermobility of upper lip using the modified lip repositioning surgery involves the suturing of the vestibular mucosa more coronal thus reducing the vestibular depth and reducing the excessive gingival display. The modified technique involves incisions on either side of the frenum leaving the frenum intact, thus maintaining the philtrum and achieve more esthetic results. As shown in this case report, this technique results in a significant reduction of the gingival display with less post operative morbidity.
References
-
Allen EP (1988) Use of Mucogingival Surgical Procedures to Enhance Esthetics. Dent Clin North Am 32(2): 307- 330.
-
Peck S, Peck L, Kataja M (1992) The gingival smile line. Angle Orthod 62(2): 91-100.
-
Goldman HM, Cohen DW (1968) Periodontal Therapy. 4th (Edn.), St. Louis, Mosby, USA.
-
Coslet JG, Vanarsdall R, Weisgold A (1977) Diagnosis and classification of delayed passive eruption of the dentogingival junction in the adult. Alpha Omegan 70(3): 24-28.
-
Kawamoto HK Jr (1982) Treatment of the elongated lower face and the gummy smile. Clin Plast Surg 9(4): 479-489.
-
Garber DA, Salama MA (1996) The aesthetic smile: Diagnosis and Treatment. Periodontol 2000 11(1): 18- 28.
-
Ahmad I (2005) Anterior dental aesthetics: Dentofacial perspective. Br Dent J 199(2): 81-88.
-
Andijani RI, Tatakis DN (2019) Hypermobile upper lip is highly prevalent among patients seeking treatment for gummy smile. Journal of periodontology 90(3): 256-262.
-
Cetin MB, Sezgin Y, Akinci S, Bakırarar B (2021) Evaluating the Impacts of Some Etiologically Relevant Factors on Excessive Gingival Display. International Journal of Periodontics & Restorative Dentistry 41(3): e73-e80.
-
Polo M (2008) Botulinum toxin type A (Botox) for the neuromuscular correction of excessive gingival display on smiling (gummy smile). American Journal of Orthodontics and Dentofacial Orthopedics 133(2): 195- 203.
-
Sucupira E, Abramovitz A (2012) A simplified method for smile enhancement: botulinum toxin injection for gummy smile. Plastic and Reconstructive Surgery 130(3): 726-728.
-
Ishda LH, Ishida LC, Ishida J, Julio G, Nivaldo A, et al. (2010) Myotomy of the levator labii superioris muscle and lip repositioning: a combined approach for the correction of gummy smile. Plastic and Reconstructive Surgery 126(3): 1014-1019.
-
Miskinyar SA (1983) A new method for correcting a gummy smile. Plast Reconstr Surg 72(3): 397-400.
-
Rubinstein AM, Kostianovsky AS (1973) Cirugia estetica de la malformacion de la sonrisa. Pren Med Argent 60: 952.
-
Rosenblatt A, Simon Z (2006) Lip repositioning for reduction of excessive gingival display: A clinical report. International Journal of Periodontics & Restorative Dentistry 26(5): 433-437.
-
Bhola M, Fairbairn PJM, Kolhatkar S, Chu SJ, Morris T, et al. (2015) LipStaT: The Lip stabilization technique- indications and guidelines for case selection and classification of excessive gingival display. International Journal of Periodontics & Restorative Dentistry 35(4): 549-559.
-
Silva CO, Ribeiro-Junior NV, Campos TV, Rodrigues JG, Tatakis DN, et al. (2013) Excessive gingival display: treatment by a modified lip repositioning technique. Journal of clinical periodontology 40(3): 260-265.
-
Mateo E, Collins JR, Rivera H, Nart J (2021) New surgical approach for labial stabilization: a long-term follow- up case series. International Journal of Periodontics & Restorative Dentistry 41(3): 405-410.
-
Arcuri T, Costa MFPD, Ribeiro IM, Júnior BDB, eSilva JPL (2018) Labial repositioning using polymethyl- methracylate (PMMA)-based cement for esthetic smile rehabilitation-A case report. International journal of surgery case reports 49: 194-204.
-
Ganesh B, Burnice NKC, Mahendra J, Vijayalakshmi R, AK K, et al. (2019) Laser-assisted lip repositioning with smile elevator muscle containment and crown lengthening for gummy smile: a case report. Clinical advances in periodontics 9(3): 135-141.
-
Younespour S, Yaghobee S, Aslroosta H, Moslemi N, Pourheydar E, et al. (2021) Effectiveness of different modalities of lip repositioning surgery for management of patients complaining of excessive gingival display: a systematic review and meta-analysis. BioMed Research International 9476013.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells
- Treatment of Temporomandibular Disorder and Orofacial Pain in Unified Health System in Brazil