A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
Introduction: Post-operative pain following endodontic procedures are often reported by patients. Pain perception is often subjective, varies for different individuals and is influenced by a range of physical and psychological factors. Pain management during and following-root canal treatment can be challenging, and previous literature reports the use of premedication to manage pain. Objective: This double-blinded, randomized clinical trial tested the effectiveness of a single, orally administered preoperative dose of Diclofenac potassium (DFK) or Dexamethasone (DEX) on postoperative pain following pulpectomy in teeth with irreversible pulpitis and symptomatic apical periodontitis. Material and Methods: 73 participants (N=73) with ages ranging from 18 to 60 years were recruited from the emergency clinics at University Dental Hospital Sharjah (UDHS), UAE. Following inclusion and exclusion criteria, participants were divided into 3 groups where either 50 mg DFK, 4 mg DEX or a placebo were given half hour prior to pulpectomy procedure. Participants recorded postoperative pain intensity at 6, 12, and 24 h using a 10-cm visual analogue scale (VAS). Results: A single preoperative dose of 50 mg DFK or 4 mg DEX reduced the incidence and severity of postoperative pain compared to placebo in all patients upto 24 h. Pain intensity data showed DEX consistently outperformed DFK and placebo, with significant differences observed at all-time points. Logistic regression analysis revealed that gender was a significant factor, with females showing higher odds of pain (p < 0.05), while age and tooth type did not significantly affect outcomes. Conclusion: The prevention of post-endodontic pain following endodontic treatment is essential for both patients and physicians. No adverse effects were reported with either medication. DEX emerged as the most effective medication for postoperative pain management.
Ibrahim Almaazmi H¹, Abraham SB¹*, Rawas-Qalaji M² and Gorduysus MO¹
¹Department of Restorative Dentistry, College of Dental Medicine, University of Sharjah, Sharjah, UAE ²Department of Pharmaceutics and Pharmaceutical Technology, College of Pharmacy, University of Sharjah, UAE Keywords: Pulpectomy; Dexamethasone; Diclofenac Potassium; Postoperative Pain
Introduction
Postoperative pain following endodontic treatment is an undesirable and frequent experience, often reported within hours after therapy [1]. Its effective prevention and management are of critical importance, as pain control not only improves patient comfort but also enhances trust in dental care. Pain arises from the release of acute inflammatory mediators such as prostaglandins, leukotrienes, bradykinin, serotonin, and cytokines, which activate and sensitize nociceptors, producing the neuronal response perceived as pain [2]. The synthesis of prostaglandins from arachidonic acid by cyclooxygenase enzymes plays a central role in mediating and amplifying inflammation and pain.
Systemic medications are frequently advocated to modulate this inflammatory response. Administration of a single oral dose of an anti-inflammatory drug before the procedure has been shown to reduce post-endodontic pain [3]. Premedication with nonsteroidal anti-inflammatory drugs (NSAIDs) is commonly recommended because of their ability to block prostaglandin synthesis and thereby attenuate both peripheral and central sensitization [4]. Diclofenac remains one of the most widely used NSAIDs in dental practice [5]. Its potassium salt exhibits higher solubility and faster absorption than the sodium form, resulting in a more rapid onset of analgesia [6]. Surveys of prescription patterns have consistently shown diclofenac to be among the preferred NSAIDs in endodontics [7], although systematic evidence remains limited [8].
Corticosteroids, such as dexamethasone, represent another class of anti-inflammatory agents with distinct mechanisms of action. By suppressing prostaglandin and leukotriene synthesis, reducing polymorphonuclear leukocyte migration, and down regulating proinflammatory cytokines, dexamethasone can attenuate postoperative inflammatory pain. A systematic review confirmed its efficacy in reducing post-endodontic pain within the first 24 hours after treatment compared with placebo [9].
Accurate assessment of pain is essential for clinical trials, although inherently challenging due to its subjective nature and the influence of physical and psychological factors. The Visual Analog Scale (VAS) has been extensively validated as a simple, reliable, and reproducible tool for pain measurement [10].
Objective
The objective of this study was to evaluate the effectiveness of preoperative oral administration of diclofenac potassium and dexamethasone in reducing postoperative pain following pulpectomy in teeth with irreversible pulpitis with symptomatic apical periodontitis. Specifically, the study aimed to determine the individual analgesic effects of diclofenac potassium and dexamethasone and to compare their efficacy in order to identify the more effective premedication for improving patient comfort after endodontic treatment. The null hypothesis assumed that premedication with either diclofenac potassium or dexamethasone would not significantly reduce postoperative pain compared with placebo.
Material and Methods
This randomized, double-blind, placebo-controlled trial was conducted at the Urgent Care Clinics of the University Dental Hospital Sharjah, University of Sharjah, UAE. The study protocol was approved by the Research Ethics Committee, University of Sharjah (Reference number: REC-23- 06-05-01- PG). All participants received information about the study, provided written informed consent, and the procedures followed were in accordance with the ethical standards of the committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000.
A total of 57 patients were required, calculated using G*Power 3.1.2 software based on an effect size of 0.48, α = 0.05, and power = 0.90, with three groups of equal size.
All patients aged 18–60 years requiring root canal treatment for irreversible pulpitis with symptomatic apical periodontitis, reporting spontaneous pain ≥3 on the Visual Analog Scale (VAS), and willing to participate were included in the study. Diagnosis was confirmed following the relevant clinical pulp tests (cold tests and electric pulp tests) and the periapical radiograph showing periodontal ligament space widening of the suspect tooth. Exclusion criteria included recent analgesic use (<12 h), allergies to study drugs, systemic contraindications (peptic ulcer, asthma, renal/hepatic impairment, bleeding disorders, uncontrolled diabetes, cardiac arrhythmia, infections, immunocompromised state), pregnancy or lactation, and gastrointestinal disorders.
Participants were randomly assigned (1:1:1) to diclofenac potassium (50 mg), dexamethasone (4 mg), or placebo groups using a computer-generated random sequence with allocation concealment through sealed opaque envelopes. Study medications and placebo were dispensed in identical gelatin capsules to ensure blinding of both operator and participants.
Patients received a single oral capsule of diclofenac potassium 50 mg, dexamethasone 4 mg, or placebo (microcrystalline cellulose) 30 minutes before pulpectomy. All drugs were within the standard therapeutic range and administered under identical instructions.
Local anesthesia was administered using 2% lidocaine with 1:100,000 epinephrine. Access cavity preparation was performed under rubber dam isolation, followed by extirpation of pulp tissue, working length determination with apex locator and radiograph, and canal preparation using rotary and hand files with irrigation by sodium hypochlorite and EDTA. The canals were dried with absorbent paper points, temporarily restored, and occlusion adjusted. All procedures were carried out by a single experienced operator (IAH).
Pain intensity was recorded using a 10-cm Visual Analog Scale at baseline, and at 6, 12, and 24 hours postoperatively. Patients reported scores via phone text to the investigator. Rescue medication (ibuprofen 400 mg every 6 h if required) was provided, and such cases were excluded from final analysis. Primary outcomes were incidence and intensity of postoperative pain, while secondary outcomes included the influence of age, gender, and tooth type. Data were analyzed using SPSS software. One-way ANOVA and Chi-square test were used for intergroup comparisons. The Friedman test with pairwise comparisons assessed intra-group changes. Logistic regression was applied to explore associations between pain incidence and clinical variables. A p-value <0.05 was considered statistically significant.
Results
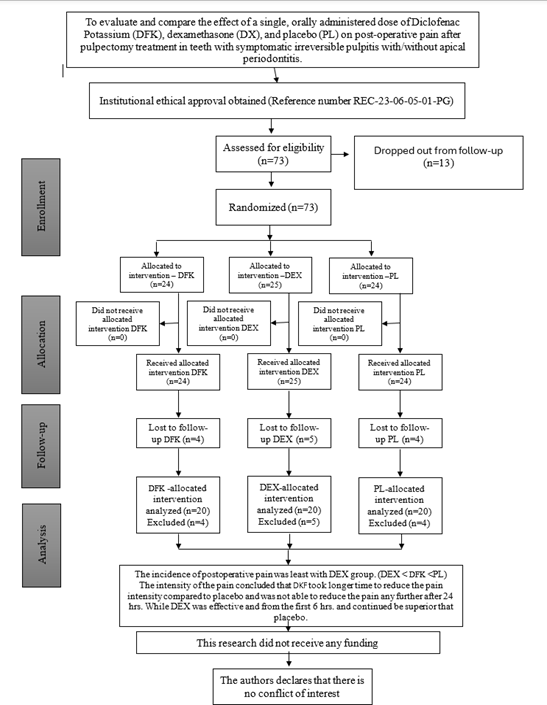
The trial commenced in September 2023 and concluded in September 2024 with 73 patients enrolled. The flow diagram of the trial is shown in Figure 1. Pulpectomy was performed on 61 molars (37 mandibular, 24 maxillary), 9 premolars (2 mandibular, 7 maxillary), and 3 anterior maxillary teeth. Thirteen patients were lost to follow-up (4 DFK, 5 DEX, 4 placebo) due to inconvenient follow-up calls, misunderstanding instructions, or lack of interest after pain relief. The operator remained blinded during data analysis. Baseline demographic and clinical characteristics. Table 1 showed no significant differences among groups for age (p = 0.739), gender (p = 0.932), tooth type (p = 1.000), or preoperative pain scores (p = 0.071).
| Variables | DFK | DEX | Placebo | P value |
|---|---|---|---|---|
| aAge (Mean, SD) | 31.80 (9.545) | 32.25 (8.058) | 33.90 (9.233) | 0.739 |
| bGender (%) | ||||
| Male | 12 (60) | 13 (65) | 12 (60) | 0.932 |
| Female | 8 (40) | 7 (35) | 8 (40) | |
| bTooth Arch (%) | ||||
| Maxillary | 9 (45) | 9 (45) | 9 (45) | 1 |
| Mandible | 11 (55) | 11 (55) | 11 (55) | |
| cPreop VAS Score (median, IQR) | 8 (2.0) | 8 (3.5) | 7 (2.0) | 0.071 |
Table 1: Baseline demographics of distribution of patients amongst the groups.
SD: Standard Deviation; Preop: Preoperative; VAS: Visual Analogue Scale; IQR: Interquartile Range a: One-Way ANOVA; b: Chi-Square Test; c: Independent samples Median Test. Table 1: Baseline demographics of distribution of patients amongst the groups.
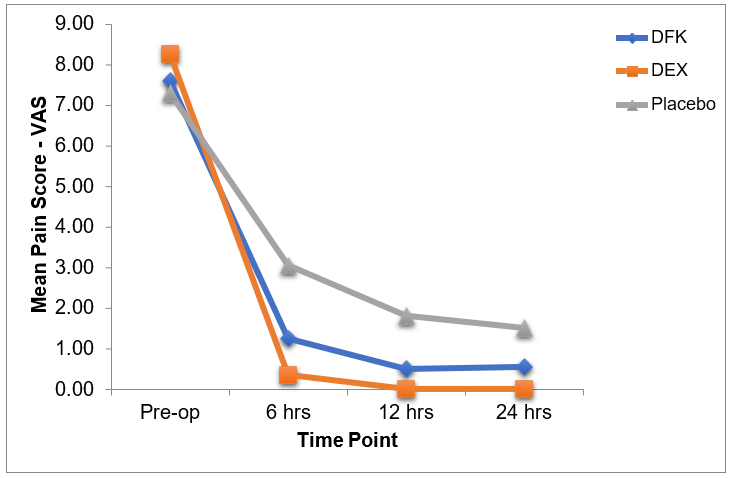
At 6, 12, and 24 hours, pain incidence differed significantly among groups (p < 0.05, <0.001, and <0.001, respectively) (Table 2 & Figure 2). Pain intensity analysis (Table 3) revealed.
| Drugs | 6 hours | 12 hours | 24 hours |
|---|---|---|---|
| DFK | 40 | 25 | 30 |
| DEX | 25 | 0 | 0 |
| Placebo | 80 | 65 | 60 |
| P value | 0.002* | <0.001** | <0.001** |
Table 2: Incidence of post-operative pain (%) at 6, 12 and 24 hrs.
Chi-Square Test *p<0.05; Significant; **p<0.001; highly significant. Table 2: Incidence of post-operative pain (%) at 6, 12 and 24 hrs.
Intra-group: No significant changes over time in DFK and DEX; significant reduction in placebo between 6–12 h and 6–24 h.
Inter-group: At 6 h, DEX vs placebo was significant; at 12 h, all groups differed significantly; at 24 h, DEX remained superior to both DFK and placebo, while DFK vs placebo was not significant.
| Time | DFK | DEX | Placebo | |
|---|---|---|---|---|
| 6 hrs | Mean (SD) | 1.25 (1.773) Aab | 0.35 (0.671) Aa | 3.05 (2.089) Ab |
| Median | 0 | 0 | 4 | |
| IQR | 2.75 | 0.75 | 3.75 | |
| 12 hrs | Mean (SD) | 0.50 (1.051) Aa | 0.0 (0.0) Ab | 1.80 (1.765) Bc |
| Median | 0 | 0 | 2 | |
| IQR | 0.75 | 0 | 3.5 | |
| 24 hrs | Mean (SD) | 0.55 (1.050) Aa | 0.0 (0.0) Ab | 1.50 (1.539) Ba |
| Median | 0 | 0 | 1.5 | |
| IQR | 1 | 0 | 2 |
Table 3: Intensity (Mean, SD, Median, IQR) of post-operative pain among three groups at 6, 12 and 24 hrs.
Same lowercase letters indicate no significant difference between the intergroup analysis at a time interval. Same uppercase letter indicates no significant difference between the various time intervals in intragroup comparison. IQR, interquartile range; SD, standard deviation. Table 3: Intensity (Mean, SD, Median, IQR) of post-operative pain among three groups at 6, 12 and 24 hrs.
OR P value 95% CI
At 6 hrs
Gender 4.188 0.036 1.099 15.955
Tooth Arch 3.698 0.059 0.954 14.341
DFK 0.107 0.007 0.021 0.544
DEX 0.05 0.001 0.008 0.291
Age 0.97 0.419 0.902 1.044
Constant 0.261 0.459
At 12 hrs
DEX 0 0.998 0 0
Gender 26.59 0.006 2.509 281.76
Tooth Arch 3.151 0.286 0.382 25.973
DFK 0.047 0.015 0.004 0.548
Age 0.958 0.46 0.856 1.073
| Constant | 0.024 | 0.093 | ||
|---|---|---|---|---|
| At 24 hrs | ||||
| DFK | 0.165 | 0.044 | 0.029 | 0.955 |
| DEX | 0 | 0.998 | 0 | 0 |
| Gender | 14.16 | 0.003 | 2.4 | 83.499 |
| Age | 1.005 | 0.912 | 0.915 | 1.105 |
| Tooth Arch | 1.769 | 0.522 | 0.309 | 10.148 |
| Constant | 0.016 | 0.054 |
Table 4: Logistic regression analysis with variables like age, gender, tooth type and pain score at 6, 12 and 24 hrs.
Logistic regression Table 4 confirmed reduced odds of pain with both DFK and DEX, with DEX showing the strongest effect. Females had consistently higher odds of pain (p < 0.05). Age and tooth location did not significantly affect outcomes.
No adverse effects were observed. Pain diary non- compliance was 16.2% (DFK), 20% (DEX), and 16.6% (placebo).
Discussion
This randomized, double-blind trial evaluated the effect of preoperative diclofenac potassium (DFK) and dexamethasone (DEX) on postoperative pain following pulpectomy in patients with irreversible pulpitis with symptomatic apical periodontitis. Pain intensity was assessed at 6, 12, and 24 hours using the Visual Analog Scale (VAS), a validated method widely applied in dental pain research [11]. VAS and Numeric Rating Scales are favored because of their simplicity, sensitivity, and reproducibility, with reported failure rates of only 4–11% [12].
Our results showed that both DEX and DFK reduced postoperative pain compared with placebo, but DEX provided faster onset and more sustained relief across all time intervals. At 6 hours, pain incidence was significantly lower in the intervention groups, with DEX at 25% and DFK at 40% compared to 80% in the placebo group. At 12 hours, DEX achieved complete pain relief (0%), while DFK reduced pain incidence to 25%, and the placebo group remained high at 65%. At 24 hours, DEX maintained full pain relief, while DFK patients reported 30% pain incidence, and placebo 60%. These findings demonstrate the superior analgesic efficacy of DEX, consistent with its broader anti-inflammatory action compared to NSAIDs.
Previous studies have highlighted similar trends. Al- Rawhani, et al. [13] reported significant pain reduction with DFK, particularly between 24 and 48 hours. Soliman, et al. [14] found that DFK provided immediate pain relief but showed diminished efficacy at 6 and 12 hours, whereas corticosteroids like DEX provided longer-lasting benefits. Suresh, et al. [5] demonstrated that DEX was highly effective in reducing postoperative pain at 6, 12, and 24 hours, outperforming both NSAIDs and placebo. Systematic reviews have also emphasized the role of corticosteroids in modulating multiple pathways of inflammation, confirming their superior role in controlling endodontic pain [9].
Meta-analyses reinforce these findings. Nagendrababu, et al. [8] ranked corticosteroids as the most effective preoperative medications for reducing postoperative endodontic pain, particularly in the first 24 hours, while diclofenac was identified as one of the most effective NSAIDs, though less potent than corticosteroids. These results are in line with our study, which directly compared the two drugs in a controlled setting, thus contributing new data to an important clinical question.
Our study’s focus on the first visit of endodontic treatment adds clinical value. Pulpectomy is often associated with heightened pain due to acute inflammation triggered by debridement and instrumentation. Effective pain management during this initial stage not only improves patient comfort but also reduces anxiety for subsequent visits and fosters compliance. These findings have immediate implications for clinicians managing patients presenting with irreversible pulpitis with symptomatic apical periodontitis.
The pharmacological differences between the drugs explain the observed outcomes. Diclofenac is a fast-acting NSAID that inhibits cyclooxygenase enzymes and reduces prostaglandin synthesis, leading to pain relief within hours. Dexamethasone, by contrast, suppresses multiple inflammatory mediators, including prostaglandins, leukotrienes, and cytokines, while also reducing leukocyte chemotaxis and reactive oxygen species. This multimodal mechanism likely explains its superior and sustained analgesic effect.
Our results align with studies showing early superiority of corticosteroids. Suresh, et al. [5] found lower pain incidences with DEX, prednisolone, and piroxicam compared to placebo (35.0%, 47.5%, and 45.9% vs 71.8%). Soliman, et al. [14] confirmed that DFK provided significant short- term pain relief but was less effective than corticosteroids beyond the immediate period. Mehrvarzfar, et al. [15] also found NSAIDs like naproxen and novafen to be effective, but their analgesic benefit was slightly less than corticosteroids at 24 hours. These consistent results reinforce the superiority of corticosteroids such as DEX.
Pain scores in our study declined significantly over time in all groups, but the decrease was fastest and most complete in the DEX group. Al-Rawhani, et al. [13] similarly reported mean pain scores with DFK around 1.0 at 24 hours and 0.5 at 48 hours, compared to higher scores in placebo. In contrast, Suresh, et al. [5] reported mean pain scores as low as 0.2 at 24 hours with DEX, far lower than placebo (≈2.0). Collectively, these findings highlight the consistent superiority of corticosteroids for prolonged pain control.
Natural resolution of inflammation, placebo effects, and psychological reassurance may account for some decline in pain in control groups, but pharmacological intervention remains essential for achieving rapid and sustained relief. This is particularly important in dental practice, where acute pain significantly impacts quality of life and patient satisfaction.
Another interesting finding in our study was the higher pain incidence among females, consistent with reports that women experience more frequent and severe postoperative pain. Biological factors, including hormonal fluctuations (estrogen and progesterone), are known to heighten nociceptive sensitivity and inflammatory responses, while psychosocial elements such as higher anxiety levels may amplify pain perception [16, 17]. Although not universally reported in endodontic studies, these gender differences underscore the importance of tailoring pain management strategies.
Our logistic regression confirmed DEX as the strongest predictor of reduced pain at 6, 12, and 24 hours, followed by DFK. Gender was a significant variable at 6 hours, with women reporting higher pain levels, while tooth location showed only borderline significance. Similar trends were noted by Suresh, et al. [5], who found reduced odds of pain with corticosteroids, though they did not detect gender- related differences. Al-Rawhani, et al. [13] also observed significant effects of DFK but no strong influence of demographic factors.
Combination therapies are increasingly explored to optimize postoperative pain relief. Menhinick, et al. [18] reported superior analgesia with ibuprofen plus acetaminophen compared to either drug alone. Kumar, et al. [19] confirmed in a systematic review that combining NSAIDs with acetaminophen or corticosteroids improved outcomes compared to monotherapy. Hashem, et al. [20] also demonstrated the benefit of ibuprofen– enzyme combinations. While our study did not evaluate combinations, future research should examine whether dexamethasone combined with NSAIDs could offer additive or synergistic benefits, balancing efficacy with safety.
Our trial has strengths including randomized double- blind design, allocation concealment, use of validated outcome measures, and standardized operator technique. However, limitations must be acknowledged. The study had a relatively short follow-up (24 hours), did not measure longer- term pain or flare-ups, and excluded patients who required rescue medication. These factors may limit generalizability. In addition, the single-center design and modest sample size reduce external validity. Future studies should involve multicenter recruitment, larger samples, and longer follow- up, while exploring dose–response relationships and multimodal regimens.
For adults undergoing pulpectomy, dexamethasone should be considered the preferred preoperative medication for controlling postoperative pain, particularly within the first 24 hours. Diclofenac potassium remains a viable alternative when corticosteroids are contraindicated or not preferred. Clinicians should tailor drug selection based on patient profile, medical history, and contraindications. Preoperative administration approximately 30 minutes before treatment appears optimal.
Conclusion
This study reinforces existing evidence that preoperative dexamethasone provides superior analgesia compared to diclofenac potassium and placebo. While NSAIDs like diclofenac potassium remain effective in reducing short- term pain, dexamethasone targets a broader inflammatory response, offering more complete and sustained relief. Gender differences in reported pain suggest that individualized strategies may further improve outcomes. Together, these findings provide valuable evidence for evidence-based selection of premedication in endodontic practice.
Conflict of Interest
The authors declare no conflict-of-interest
Funding
This study did not receive any funding
References
-
Wang C, Xu P, Ren L, Dong G, Ye L (2010) Comparison of post-obturation pain experience following one-visit and two-visit root canal treatment on teeth with vital pulps: a randomized controlled trial. Int Endod J 43(8): 692-697.
-
Shahi S, Mokhtari H, Rahimi S, Yavari HR, Narimani S, et al. (2013) Effect of premedication with ibuprofen and dexamethasone on success rate of inferior alveolar nerve block for teeth with asymptomatic irreversible pulpitis: a randomized clinical trial. J Endod 39(2): 160-162.
-
Jalalzadeh SM, Mamavi A, Shahriari S, Santos FA, Pochapski MT (2010) Effect of pretreatment prednisolone on post endodontic pain: a double-blind parallel-randomized clinical trial. J Endod 36(6): 978-981.
-
Hargreaves KM, Keiser K (2002) Local anesthetic failure in endodontics: Endodontic Topics 1: 26-39.
-
Suresh N, Nagendrababu V, Koteeswaran V, Haritha JS, Swetha SD, et al. (2021) Effect of preoperative oral administration of steroids in comparison to an anti- inflammatory drug on postoperative pain following single-visit root canal treatment - a double-blind, randomized clinical trial. Int Endod J 54(2): 198-209.
-
Derry S, Wiffen PJ, Moore RA (2015) Single dose oral diclofenac for acute postoperative pain in adults. Cochrane Database Syst Rev 2015(7): CD004768.
-
Jayadev M, Karunakar P, Vishwanath B, Chinmayi SS, Siddhartha P, et al. (2014) Knowledge and pattern of antibiotic and non-narcotic analgesic prescription for pulpal and periapical pathologies- a survey among dentists. J Clin Diagn Res 8(7): ZC10-ZC14.
-
Nagendrababu V, Pulikkotil SJ, Jinatongthai P, Veettil SK, Teerawattanapong N, et al. (2019) Efficacy and safety of oral premedication on pain after nonsurgical root canal treatment: a systematic review and network meta- analysis of randomized controlled Trials. J Endod 45(4): 364-371.
-
Nogueira BML, Silva LG, Mesquita CRM, Menezes SAF, Menezes TOA, et al. (2018) Is the use of Dexamethasone effective in controlling pain associated with symptomatic irreversible pulpitis? A systematic review. J Endod 44(5): 703-710.
-
Scott J, Huskisson EC (1976) Graphic representation of pain. Pain 2(2): 175-184.
-
Jensen MP, Chen C, Brugger AM (2003) Interpretation of visual analog scale ratings and change scores: a reanalysis of two clinical trials of postoperative pain. J Pain 4(7): 407-414.
-
Kremer E, Atkinson HJ, Ignelzi RJ (1981) Measurement of pain: patient preference does not confound pain measurement. Pain 10(2): 241-248.
-
Al-Rawhani AH, Gawdat SI, Wanees Amin SA (2020) Effect of diclofenac potassium premedication on post endodontic pain in mandibular molars with symptomatic irreversible pulpitis: a randomized placebo-controlled double-blind trial. J Endod 46(8): 1023-1031.
-
Soliman AA, Ezzat KM, Shaker OG, Abouelenien SS (2024) Influence of diclofenac potassium versus prednisolone on post endodontic pain and pulpal interleukin-8 expression in symptomatic irreversible pulpitis cases: a randomized placebo-controlled trial. J Endod 50(9): 1213-1220.
-
Mehrvarzfar P, Abbott PV, Saghiri MA, Delvarani A, Asgar K, et al. (2012) Effects of three oral analgesics on postoperative pain following root canal preparation: a controlled clinical trial. Int Endod J 45(1): 76-82.
-
Berkley KJ (1997) Sex differences in pain. Behav Brain Sci 20(3): 371-380.
-
Bartley EJ, Fillingim RB (2013) Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth 111(1): 52-58.
-
Menhinick KA, Gutmann JL, Regan JD, Taylor SE, Buschang PH (2004) The efficacy of pain control following nonsurgical root canal treatment using ibuprofen or a combination of ibuprofen and acetaminophen in a randomized, double-blind, placebo-controlled study. Int Endod J 37(8): 531-541.
-
Kumar G, Sangwan P, Tewari S (2021) Effect of premedication on postoperative pain after root canal therapy in patients with irreversible pulpitis: a systematic review and meta-analysis. J Dent Anesth Pain Med 21(5): 397-411.
-
Hashem AAR, Abd El Sattar AA, Abdel Rahman TY (2023) The effect of trypsin-chymotrypsin on postoperative pain after single visit endodontic treatment: a randomized controlled trial. J Endod 49(3): 240-247.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells
- Treatment of Temporomandibular Disorder and Orofacial Pain in Unified Health System in Brazil