Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
Mental nerve paraesthesia of odontogenic origin is rare and its etiology may be misdiagnosed during initial evaluation. The present case report describes a 37-year-old female presenting with persistent numbness and tingling of the left lower lip and chin, with no improvement in symptoms despite medical consultation. Neurosensory assessment revealed complete sensory deficit (S0) of the said dermatome. Clinical examination revealed deep caries in left mandibular second premolar (#20), and its radiographic findings disclosed a periapical radiolucency. 3-Dimensional imaging using cone-beam computed tomography (CBCT) was conducted to confirm the etiological relationship of periapical radiolucency in #20 with the mental nerve. Non-surgical endodontic treatment (NSET) was performed, resulting in progressive neurosensory recovery from S0 to S4 over eight weeks. This case highlights the critical importance of accurate diagnosis in patients presenting with unexplained paraesthesia and underscores the value of CBCT in delineating the relationship between periapical pathology and adjacent neural structures. NSET can effectively eliminate the etiology in such cases, aiding in complete neurosensory recovery without the need for any surgical intervention.
Introduction
Paresthesia refers to an altered or abnormal sensory perception, commonly described as burning, prickling, tingling, or tickling sensations. Clinically, it may present in various forms, including complete loss of sensation (anesthesia), unpleasant abnormal sensations such as burning or tingling (dysesthesia), pain elicited by non- noxious stimuli (allodynia), or an exaggerated pain response to stimuli (hyperesthesia) [1]. Facial paresthesia can result from either local or systemic causes. Local etiologies encompass traumatic injuries such as mandibular fractures, compressive space-occupying lesions, impacted teeth and infectious conditions such as osteomyelitis, periapical and peri-implant pathologies. Iatrogenic factors may include complications associated with tooth extraction, administration of local anesthesia, endodontic procedures (including overextension of obturating materials and apical surgery), implant placement, and preprosthetic surgical interventions. Paresthesia affecting the facial region most often involves the inferior alveolar and mental nerves [2].
The mental foramen is most commonly located in the region of the mandibular premolars, frequently between the first and second premolars, and often lies in close proximity to their root apices. In a morphometric study, Phillips, et al. [3] reported that the mental foramen is positioned approximately 2.4 mm inferior to the radiographic apex of the mandibular second premolar. Cadaveric investigations have further indicated that the distance between the mandibular second premolar apex and the mental foramen may vary, ranging from 0- 4.7 mm [4]. The anatomical proximity between the apices of mandibular premolars and the mental foramen may facilitate the extension of periapical infections to the mental nerve. Inflammatory processes associated with such lesions can induce ischemia, while the accumulation of suppurative or inflammatory exudate and the release of bacterial toxins may generate localized mechanical pressure in the surrounding bone, ultimately leading to paresthesia of the mental nerve [5].
The reported incidence of mental nerve paresthesia resulting from periapical infection or pathology is less than 1% [6]. Buchanan et al, reported paresthesia of lower left lip due to incomplete primary endodontic treatment of the left mandibular second premolar tooth, which further resulted in the progression of apical periodontitis involving the left mental neurovascular bundle [7]. Similarly, Patel, et al. [8] reported two clinical cases of mental nerve paraesthesia due to close proximity of mental nerve foramen to periapical infections in respect to mandibular second premolar teeth.
The present report describes a rare case presenting a diagnostic challenge, wherein mental nerve paresthesia was initially misdiagnosed and subsequently identified using advanced three-dimensional cone-beam computed tomography (CBCT) imaging.
Case Report
A 37-year-old female patient with progressive neurosensory disorders of the lower lip and chin was referred to the department of conservative dentistry and endodontics. The patient presented with a chief complaint of unilateral paresthesia accompanied by a tingling sensation involving the left lower lip, since three months. She had previously consulted a neurologist and was prescribed Vitamin B therapy for the same. However, despite compliance with the medication, no improvement in symptoms was observed. The patient’s medical history was non-contributory and this was her first dental visit. On Extra-oral examination the patient had facial symmetry with no pain or sinus tracts.
Neurosensory evaluation: Neurosensory evaluation was performed using standardized tests, as recommended by Robinson, et al. [9] (Figure 1).
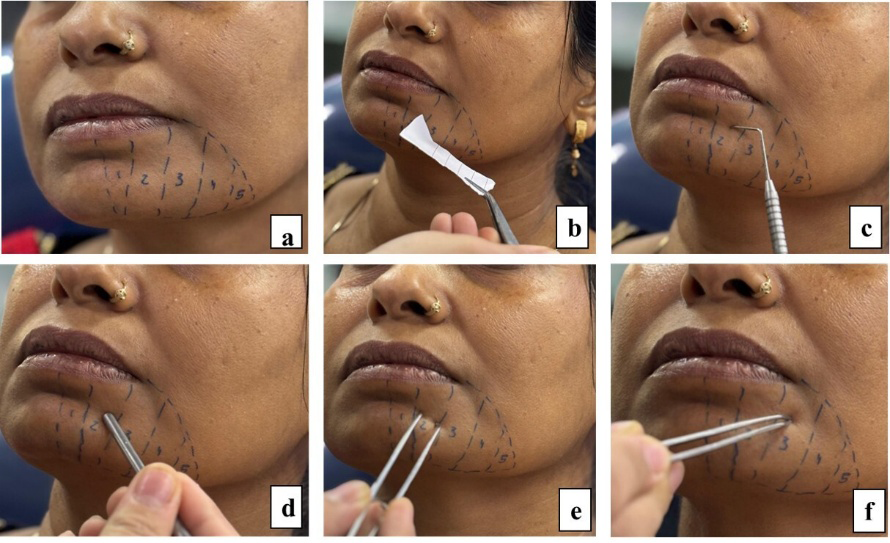
Figure 1: Neurosensory evaluation tests performed. a. Mapping of the injury site; b. Light touch perception; c. Sharp discrimination test ; d. Blunt discrimination test; e. Two point discrimination test (open beak); f. Two point discrimination test (close beak) Mapping the injury area: The involved neuropathic region was carefully mapped and recorded by marking its extent on the patient’s face with a ballpoint pen.
Function scoring: A subjective assessment of sensory function was obtained by asking the patient to compare the affected side with the contralateral normal side on a scale of 0 to 10, where 0 represented no perception of touch and 10 represented normal sensation. The patient assigned a score of 0 to the left lip and chin area.
Light touch test: The corner of a paper was moved over the injured area and repeated 5 times. The patient reported lack of light touch perception.
Sharp/blunt discrimination test: Sensory testing with a dental probe (tip and handle) revealed an inability to differentiate between sharp pricking and blunt pressure sensations.
Two-point discrimination test: The patient was unable to
discriminate between 2 pressure points (open-beak tweezer) and a single pressure point (closed-beak tweezer).
Based on the British Medical Research Council Score
of sensory recovery modified by Mackinnon, et al. [10], the patient was assigned a primary sensory function score was S0 (Table 1).
| S0 | Absence of sensibility in the autonomous area of the nerve |
|---|---|
| S1 | Recovery of deep cutaneous pain and tactile sensibility |
| S1+ | Recovery of superficial pain sensibility |
| S2 | Recovery of some degree of superficial cutaneous pain and tactile sensibility |
| S2+ | As in S2, but with over response |
| S3 | Return of pain and tactile sensibility with disappearance of over response, s2pd>15mm, m2pd>7mm |
| S3+ | Return of sensibility as in S3 with some recovery of 2-point discrimination, s2pd: 7-15mm, m2pd: 4-7mm |
| S4 | Complete recovery, s2pd: 2-6mm, m2pd: 2-3mm |
Table 1: British Medical Research Council Score of sensory recovery modified by Mackinnon and Dellon.
Intra-oral examination revealed deep carious lesion with respect to mandibular left second premolar (#20), tenderness on percussion was negative, pulp sensibility tests such as cold test (Endo-Frost, coltene, Switzerland) and electric pulp testing showed no response and confirmed non vitality of the tooth.
Radiographic examination: Digital intraoral radiography of #20 revealed a deep carious lesion involving pulp and a ill- defined periapical radiolucency. A CBCT scan was advised to check for any aberrant root canal anatomy and to delineate the position and proximity of mental foramen with respect to the periapical lesion. A small field of view (FOV) CBCT (NEWTOM NNT at 6*6 mm voxel size, exposure time 5.6 s, with slice thickness of 0.5 mm) was obtained, which showed an ill-defined, non-corticated periapical radiolucent lesion (7.9 x 7.7 mm in size) involving inferior alveolar canal and mental foramen (Figure 2).
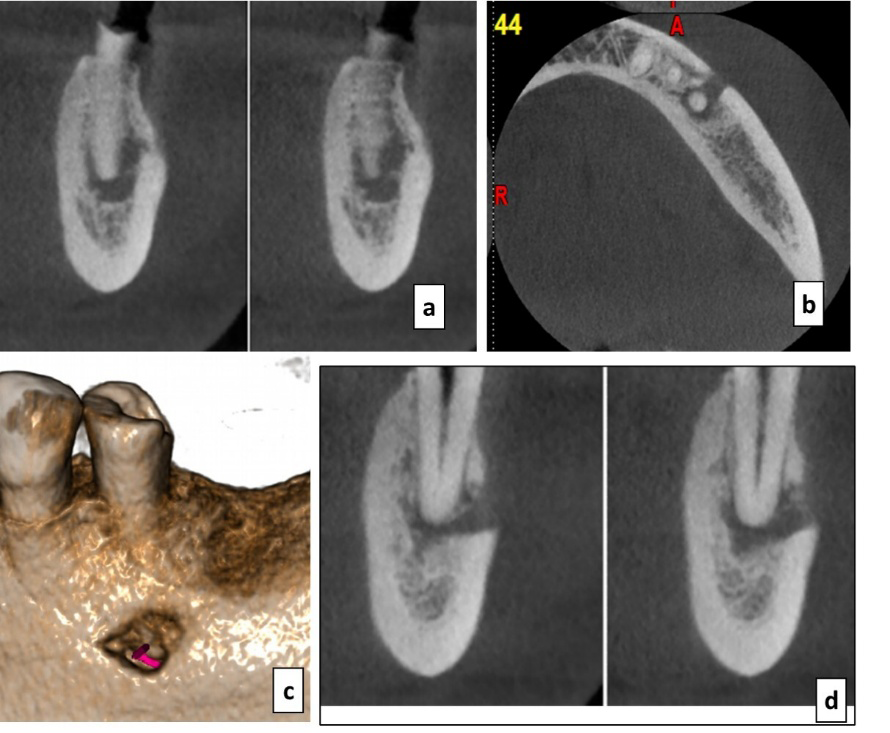
Figure 2: 3-D Imaging evaluation using CBCT. a. Transaxial section of #20 showing periapical lesion involving inferior alveolar canal with erosion on upper cortex of IAN canal. b. Axial section displaying periapical lesion involving mental foramen. c. 3D representation of the spatial relationship of mental nerve foramen with periapical lesion of #20 d. Transaxial section showing an ill-defined periapical radiolucency involving mental foramen with erosion of buccal cortical plate.
![Figure 3: Endodontic management of mandibular left second premolar (#20). a. Pre-operative Radiograph b. Working length determination c. Master cone d. Obturation and post endodontic restoration **Clinical Procedures:** Non-surgical endodontic treatment was advised in respect to #20. During the first visit, local anesthesia was achieved with 2% lidocaine containing epinephrine 1:100,000 (Xicaine, ICPA, INDIA) and tooth was isolated under rubber dam, caries was excavated and access cavity was prepared. Patency was achieved with a stainless steel #10 K file (Mani, Inc. MDCI Ltd. Japan). The working length was determined using electronic apex locator (Root ZX® II, Densply, J-Morita Inc., USA), and confirmed radiographically thereafter. Biomechanical preparation was done with Neo-endo files (Orikam Healthcare, India) up to 35.04% till working length. Between instrumentation, the root canals were irrigated with 2 mL of 2.5% sodium hypochlorite solution (Bharat Chemical, India), using 30G side vented needle (Endo-Rinse, SuperEndo, India), kept 2mm short of the apex. Calcium Hydroxide (Ca[OH]2) (Prevest DenPro, India) paste was then placed in the root canal and the access cavity was sealed with temporary filling material. (Orafil-G™, PREVEST DenPro, India). The patient was prescribed a vitamin B-complex supplement as part of the supportive management. One week later, the patient reported the onset of pain sensation in the subcutaneous region of the lower lip and chin, corresponding to a neurosensory score of S1. The temporary restoration was removed, and the root canal system was irrigated with saline (0.9% v/w, Infutec, India). The intracanal medicament was refreshed using a combination of calcium hydroxide and chlorhexidine (Ammdent Dentochlor). At the subsequent visit, with improvement in the neurosensory function to S2 and absence of any tooth-related symptoms, obturation was performed using a bioceramic sealer (Bioactive RCS, Safe Endo, India) in conjunction with a single-cone gutta-percha technique. The access cavity was restored by placing a thin layer of resin-modified glass ionomer (Glasseal, Waldent, India) over the gutta-percha as an intra-orifice barrier to enhance coronal sealing, followed by acid etching, application of a dentin bonding agent, and placement of composite resin as the definitive restoration. (Te-Econom Plus, Ivoclar Vivadent India Pvt. Ltd.).](/fulltextimages/14194/fig_3.png)
Figure 3: Endodontic management of mandibular left second premolar (#20). a. Pre-operative Radiograph b. Working length determination c. Master cone d. Obturation and post endodontic restoration Clinical Procedures: Non-surgical endodontic treatment was advised in respect to #20. During the first visit, local anesthesia was achieved with 2% lidocaine containing epinephrine 1:100,000 (Xicaine, ICPA, INDIA) and tooth was isolated under rubber dam, caries was excavated and access cavity was prepared. Patency was achieved with a stainless steel #10 K file (Mani, Inc. MDCI Ltd. Japan). The working length was determined using electronic apex locator (Root ZX® II, Densply, J-Morita Inc., USA), and confirmed radiographically thereafter. Biomechanical preparation was done with Neo-endo files (Orikam Healthcare, India) up to 35.04% till working length. Between instrumentation, the root canals were irrigated with 2 mL of 2.5% sodium hypochlorite solution (Bharat Chemical, India), using 30G side vented needle (Endo-Rinse, SuperEndo, India), kept 2mm short of the apex. Calcium Hydroxide (Ca[OH]2) (Prevest DenPro, India) paste was then placed in the root canal and the access cavity was sealed with temporary filling material. (Orafil-G™, PREVEST DenPro, India). The patient was prescribed a vitamin B-complex supplement as part of the supportive management. One week later, the patient reported the onset of pain sensation in the subcutaneous region of the lower lip and chin, corresponding to a neurosensory score of S1. The temporary restoration was removed, and the root canal system was irrigated with saline (0.9% v/w, Infutec, India). The intracanal medicament was refreshed using a combination of calcium hydroxide and chlorhexidine (Ammdent Dentochlor). At the subsequent visit, with improvement in the neurosensory function to S2 and absence of any tooth-related symptoms, obturation was performed using a bioceramic sealer (Bioactive RCS, Safe Endo, India) in conjunction with a single-cone gutta-percha technique. The access cavity was restored by placing a thin layer of resin-modified glass ionomer (Glasseal, Waldent, India) over the gutta-percha as an intra-orifice barrier to enhance coronal sealing, followed by acid etching, application of a dentin bonding agent, and placement of composite resin as the definitive restoration. (Te-Econom Plus, Ivoclar Vivadent India Pvt. Ltd.).
Follow-up evaluation at four weeks demonstrated further improvement in neurosensory status to S3, with complete recovery (S4) achieved by the end of eight weeks.
Discussion
Traumatic injuries to nerve are classified into three categories based on the severity of trauma and the feasibility of complete postoperative regeneration (Table 2) [5]. Most paresthesia cases are due to the neuropraxia, in which a transient trauma is inflicted on the myelin sheath of the nerve, with no injury to the nerve axon [11]. Periapical inflammation of mandibular premolars and the distal roots of second molars is the most common etiologic factor for paresthesia of the mental and inferior alveolar nerve respectively [6, 12].
| Types of neural injuries | Definition |
|---|---|
| Neuropraxia | Occurs when a nerve is injured and conduction is blocked, but this does not lead to Wallerian degeneration |
| Axonotmesis | Results in damage to the axons, but the endoneurial and epineurial sheaths are preserved |
| Neurotmesis | Conduction is completely disrupted resulting in the loss of anatomic integrity of the endoneu- rium, perineurium and epineurium |
Table 2: Seddon’s classification of Neural injuries.
The present report highlighted a clinical case of mental nerve paresthesia of the left lower lip and chin dermatome, manifested most likely due to periapical inflammation of #20. Patient had no complaints of dental origin, a non- contributory medical history and was already on medicinal therapy for her neurological symptoms. A series of subjective neurosensory tests, followed by a thorough intraoral examination was conducted to arrive at the provisional diagnosis. The diagnosis was further confirmed by high end 3-dimensional imaging modality, i.e. CBCT.
The diagnosis of mental nerve paraesthesia, is primarily based on subjective clinical neurosensory assessment. These evaluations are broadly classified into mechanoreceptive and nociceptive modalities, depending on the receptors stimulated. Mechanoreceptive tests include static light touch, two-point discrimination, and directional brush stroke analysis, while nociceptive assessment involves pinprick and thermal discrimination tests [13]. In the present clinical case, the neurosensory evaluation was performed using light touch test, sharp/ blunt discrimination test, two- point discrimination test and functional scoring along with mapping the affected region [9]. The patient was assigned a primary baseline sensory score and a score on each follow up visit, based on the well validated British Medical Research Council Score of sensory recovery [10].
Following the neurosensory evaluation of the affected dermatome, a thorough intraoral examination was performed to determine the etiology of the mental nerve paresthesia. This was patient’s first dental visit, which ruled out any post procedural or iatrogenic causes of nerve injury. The intraoral examination further revealed carious mandibular left second premolar (#20), with a diagnosis of pulp necrosis with asymptomatic apical periodontititis. To further confirm the diagnosis, and to establish a spatial relationship between the mental foramen and the periapical lesion, a limited FOV CBCT imaging was performed. CBCT offers a small field of view with relatively less radiation and is recommended as a diagnostic aid in examining causes, suggesting a safety zone for any procedure, and delineating important structures missed with conventional periapical radiography. There were no extra canals/aberrant anatomy visible in CBCT imaging [8]. Also, the CBCT imaging clearly demonstrated the periapical lesion involving mental foramen, which confirmed the etiology of mental nerve paresthesia in the present case report.
The periapical inflammation due to an infectious root canal system might give rise to neuropraxia due to hyperemia and inflammatory edema, which compresses the nerve, thereby injuring the nearby neural bundles. Furthermore, ischemia might lead to nerve dysfunction, associated with the symptoms and signs of paresthesia [14]. Furthermore, Gram-negative bacteria endotoxins and metabolic products of bacteria might have neurotoxic effects [5]. On the other hand, direct invasion of nerve structures by bacteria themselves might be another factor injuring the nerve structures [15]. Thus, the treatment modalities for management of teeth with periapical inflammation leading to nerve paresthesia, include: extraction of the causative tooth, surgical intervention, or conservative non-surgical endodontic treatment [16].
Infection-related mental nerve paresthesia usually subsides after appropriate endodontic therapy. As soon as the cause is removed, paresthesia should resolve within days or weeks [17]. Naik, et al. [17] reported the resolution of mental nerve paresthesia due to endodontic infection of the mandibular second premolar within one week after endodontic treatment. For the present case, non-surgical endodontic treatment was undertaken in #20, it being the most conservative option, supported with Vitamin B complex therapy, subsequently resolving the paresthesia in eight weeks [18].
Elimination of bacteria from the infected root canal system of #20, was performed using strict infection control measures, including: rubber dam isolation, thorough debridement of the root canal system, a well-defined irrigation protocol, inter-appointment calcium hydroxide medication and proper sealing of the root canal system both apically and coronally. Obturation was done using bioceramic sealer and single matching GP cones. Although gutta-percha is considered a biologically inert material, but the collective effect of over- instrumentation and excessive vertical pressure during compaction of the filling material may exaggerate the pre- existing paraesthesia. Thus, a single cone obturation using bioceramic sealer was undertaken in the present case [7]. During endodontic treatment in such cases, care should be exercised in working length determination (with the use of radiography and apex locators), preparation and root canal obturation steps due to the close proximity of the apices of these teeth to nerves [5]. Following endodontic treatment, resolution of the associated nerve injury occurred without the need for surgical intervention.
In the present case, endodontic therapy was supplemented with Vit B complex therapy. B-complex vitamins, particularly thiamine (B1), pyridoxine (B6), and cyanocobalamin (B12), have demonstrated antinociceptive properties in neuropathic pain associated with neuronal injury. Furthermore, vitamin B complex contributes to nerve regeneration by enhancing Schwann cell proliferation, increasing myelinated fiber density, and promoting axonal growth. Collectively, these effects support their role as adjunctive agents in facilitating recovery following peripheral nerve injury.
Non-surgical endodontic treatment in combination with pharmacological therapy of vitamin B complex led to a gradual reduction of patient’s paraesthesia in 8 weeks, evaluated using the neurosensory tests.
Conclusion
In conclusion, long-standing untreated apical periodontitis can lead to significant neurosensory complications, including paraesthesia, due to involvement of adjacent neural structures. This case underscores the importance of meticulous diagnostic evaluation in patients presenting with sensory disturbances, particularly when the initial assessment fails to identify an odontogenic source. The use of cone-beam computed tomography (CBCT) proved indispensable in accurately delineating the relationship between the periapical lesion and the mental foramen. Notably, in this case, the Mental foramen was in close proximity of the lesion, thereby accounting for the patient’s symptoms of lower lip and chin numbness. Neurosensory assessment demonstrated a marked improvement from an initial score of S0 to S4 following treatment. Non-surgical endodontic therapy effectively eliminated the source of infection, resulting in complete resolution of the paraesthesia. These findings highlight the critical role of advanced imaging and conservative endodontic management in achieving favorable clinical outcomes.
References
-
Moore PA, Haas DA (2010) Paresthesias in Dentistry. Dent Clin North Am 54(4): 715-730.
-
Censi R, Vavassori V, Borgonovo AE, Re D (2016) Infection Related Inferior Alveolar Nerve Paresthesia in the Lower Premolar Teeth. Case Rep Dent 2016: 2623507.
-
Phillips JL, Weller RN, Kulild JC (1992) The mental foramen: 2. Radiographic position in relation to the mandibular second premolar. J Endod 18(6): 271-274.
-
Denio D, Torabinejad M, Bakland LK (1992) Anatomical relationship of the mandibular canal to its surrounding structures in mature mandibles. J Endod 18(4): 161-165.
-
Shadmehr E, Shekarchizade N (2015) Endodontic periapical lesion-induced mental nerve paresthesia. Dent Res J 12(2): 192-196.
-
Knowles KI, Jergenson MA, Howard JH (2003) Paresthesia associated with endodontic treatment of mandibular premolars. J Endod 29: 768-770.
-
Buchanan GD, Smit C, Gamieldien MY, ElSheshtawy AS (2023) Resolution of Apical Periodontitis-induced Mental Nerve Paresthesia Through Nonsurgical Endodontic Retreatment: A Case Report. J Endod 49(7): 920-924.
-
Patel N, Langaliya A, Kanodia S, Kumbhar A, Buch A, et al. (2021) Mental Nerve Paraesthesia: A Report of Two Cases Associated with Endodontic Etiology. Case Rep Dent 2021: 1747519.
-
Robinson PP, Smith KG, Johnson FP, Coppins DA (1992) Equipment and methods for simple sensory testing. Br J Oral Maxillofac Surg 30(6): 387-389.
-
Wang Y, Sunitha M, Chung KC (2013) How to measure outcomes of peripheral nerve surgery. Hand Clin 29(3): 349-361.
-
Graff-Radford SB, Evans RW (2003) Lingual Nerve Injury. Headache 43: 975-983.
-
Varinauskas V, Nimcenko T, Kubilius R (2011) Case report: inferior alveolar nerve injury due to root canal treatment, diagnosis and treatment possibilities. Biomedicina 21: 89-95.
-
Lambrianidis T, Molyvdas J (1987) Paresthesia of the inferior alveolar nerve caused by periodontal-endodontic pathosis. Oral Surg Oral Med Oral Pathol 63(1): 90-92.
-
Szmigielski S, Blankenship M, Robinson JP, Harshman S (1979) Injury of myelin sheaths in isolated rabbit vagus nerves by alpha-toxin of Staphylococcus aureus. Toxicon 17(4): 363-371.
-
Genc Sen O, Kaplan V (2015) Temporary Mental Nerve Paresthesia Originating from Periapical Infection. Case Rep Dent 2015: 457645.
-
Morse DR (1997) Infection-related mental and inferior alveolar nerve paresthesia: literature review and presentation of two cases. J Endod 23(7): 457-460.
-
Naik A, Ataide IN, Fernandes M (2011) Management of paresthesia in relation to mandibular second premolar-a case report. Int J Dent Case Rep 1: 40-45.
-
Altun I, Kurutaş EB (2016) Vitamin B complex and vitamin B12 levels after peripheral nerve injury. Neural Regen Res 11(5): 842-845.
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells
- Treatment of Temporomandibular Disorder and Orofacial Pain in Unified Health System in Brazil