Ovarian Endometrioma: Rate of Recurrence and Factors Correlated
Background: To evaluate the recurrence rate of ovarian endometrioma during a period of five years and risk factors associated with this disorder. Methods: A retrospective cross-sectional study of 97 women diagnosed with ovarian endometrioma during a period of 5 years was conducted. These women were recruited from the Endometriosis Outpatient Facility at the University of Campinas. The following variables were analyzed in the groups of women with and without recurrence of ovarian endometrioma: age, pregnancies, parity, cesarean section, abortion, body mass index (BMI), symptomatology of endometrioma (dysmenorrheal, dyspareunia, chronic pelvic pain and infertility), type of surgery for excision of endometrioma (laparotomy or laparoscopy), presence of other foci, postoperative treatment with drugs and associated disorders. The frequencies, means and standard deviation were analyzed for each variable. Fisher’s exact test and logistic regression model were used for a comparative analysis between variables. Results: The mean age of the patients was 33.8±6.6 years. The recurrence rate of endometrioma was 40.2% and the mean time for disease recurrence was 34 months after surgery. There was a significant association between a higher recurrence rate of endometrioma and the presence of other foci (p=0.03). There was no statistical significance of the recurrence of endometrioma with the other variables. Conclusion: The recurrence rate of ovarian endometrioma is high. Women with advanced stages of endometriosis have a higher recurrence rate of endometrioma and recurrence is higher at 2 years after surgery. The postoperative treatments with drugs do not change the recurrence rate of ovarian endometrioma.
Introduction
Endometriosis is characterized by the presence of endometrial tissue outside the uterine cavity. There seems to be a familial tendency for the disease. Although it has not been fully elucidated, genetic inheritance is most likely multi factorial. The incidence of endometriosis ranges between 1% and 15% of women. Of these women, 20% to 40% have ovarian endometrioma. Ovarian endometrioma has a high prevalence and recurrence rate in the population [1, 2, 3]. The implications of this disorder are highly undesirable for women, who may present with pain and infertility. A study of women with ovarian endometriomas showed a total recurrence rate of 29.4% and a high cumulative recurrence index of 42% in a 5-year period following surgery. This same study attempted to associate risk factors for recurrence and concluded that women aged younger at the time of endometrioma excision had a higher risk of recurrence, while pregnancy after endometrioma excision decreased the recurrence risk [4]. Other studies associated the higher recurrence rate with a larger diameter of cystic mass and a lower recurrence rate with pregnancy after surgery and oral contraceptive use [5, 6]. The aim of this study was to retrospectively evaluate the recurrence rate of ovarian endometrioma related to potential risk factors. Furthermore, patients can be much better informed about their prognosis. Measures can be taken to reduce the recurrence of ovarian endometriomas and minimize impairment in these women.
Methods
A retrospective study of 97 women diagnosed with ovarian endometrioma diagnosed by anatomopathology and recruited from the Endometriosis Outpatient Facility at the University of Campinas was carried out from 2009 to 2014. All women had undergone excision of ovarian endometrioma by laparoscopy or laparotomy in the moment of inclusion of the study for the first time. The diagnosis of ovarian endometrioma was confirmed by histopathological analysis of the surgical specimen. During surgery, the abdominal cavity was inspected to assess the extent of endometriosis, according to a revised classification from the American Society of Reproductive Medicine (r ASRM). It was observed that patients had stage III or IV disease. Women who were treated after diagnostic confirmation of endometrioma received GnRH agonists for 3 months or combination estrogen/progestin oral contraceptive or continuous progestin. All the women were carried out during a period of five years by ultrasound each year. Recurrence of endometrioma was defined as the presence of a thick fluid cyst on transvaginal ultrasound with histopathological confirmation after excision. They were included all women with diagnosis of ovarian endometrioma by histopathological analysis and kept following the service for at least 5 years. They were excluded menopausal women and those whose medical records had not necessary data. The following variables were analyzed: age, pregnancies, parity, cesarean section, abortion, body mass index (BMI), symptomatology of endometrioma (dysmenorrhea, dyspareunia, chronic pelvic pain and infertility), duration of symptomatology, type of surgery for the excision of endometrioma (laparotomy or laparoscopy), staging of endometriosis, associated disorders, postoperative treatment with drugs that block menstruation, pregnancy after surgery. This study was approved by the Research Ethics Committee of the institution under number 699671/2014.
Statistical analysis
Sample size was based on the recurrence rate of ovarian endometrioma after laparoscopy, which was equal to 45.1% [5]. The rate was calculated according to methodology demonstrated by Hulley et al. The Z test was used for prevalence’s. Considering a significance level of 5%, a confidence level of 95% and a tolerable absolute error of 10%, we obtained n = 96 cases [7]. For statistical analysis, the frequencies, means and standard deviation of the variables were evaluated. To compare variables of women with and without recurrence, the Student’s t-test and the Mann-Whitney were used. For analysis of recurrence factors, Fisher’s exact was used. For the performance of these procedures, the SAS software version 9.4 was used.
Results
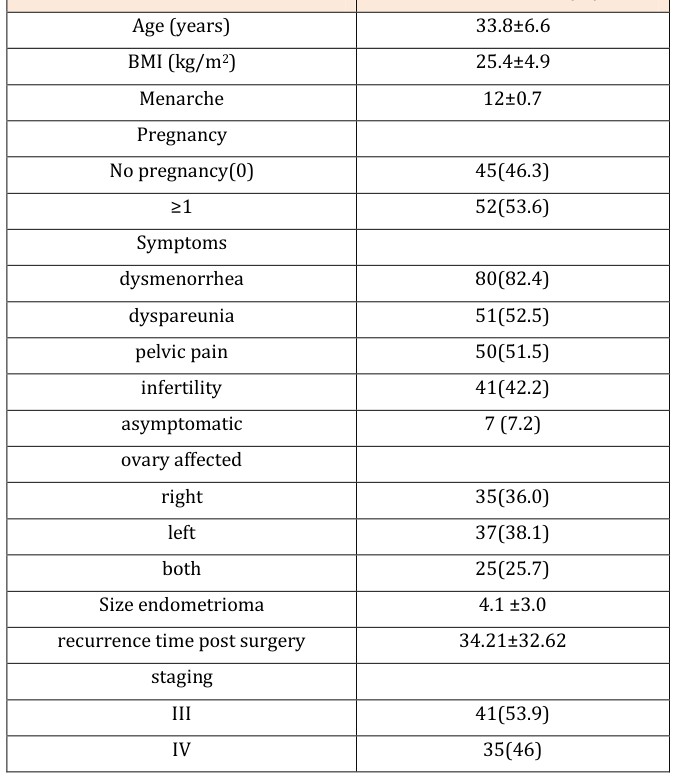
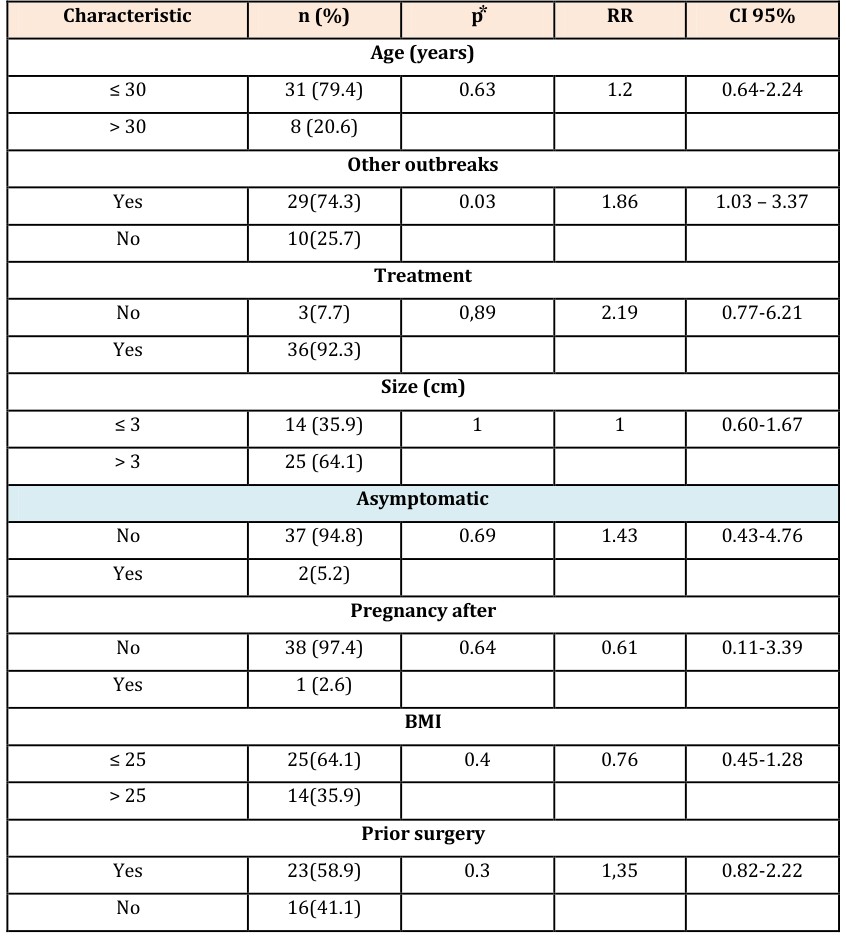
The mean age of the patients was 33.8±6.6 years. Mean age at menarche was 12±0.7 years and BMI was 25.4±4.9 kg/m2. We observed that 46.39% of patients were nulliparous women, 7.22% were asymptomatic and 46.6% reported having infertility. The most frequent symptom was dysmenorrhea (82.6%). The left ovary was most commonly affected (62.6%). All women had advanced stages of endometriosis (III or IV) and mean endometrioma size was 4.1±3 cm (Table 1). The recurrence rate was 40.2% at a mean postoperative period of 34 months. There was no significant statistical difference between age, BMI, duration of dysmenorrhea and dyspareunia and size of the first endometrioma in the moment of the surgery in women with and without recurrence, but there was a significant difference in the duration of pelvic pain among these women (p=0.04) (Table 2). There was a significant association between a higher recurrence of endometrioma and the presence of other foci (p = 0.03). Early-stage endometriosis has a lower chance of recurrence than advanced-stage endometriosis (Stage IV). There was no statistical significance in the recurrence of endometrioma with the other variables (Table 3). Patients mean ± SD or n (%)
| Yes (n=39) | No (n=58) | P | |
|---|---|---|---|
| Age# | 33.23 ± 4.54 | 34.06 ± 7.1 | 0.4 |
| BMI # | 25.73± 5.7 | 25.15± 4.35 | 0.07 |
Table 1: Characteristics of women with ovarian endometrioma (N=97).
| 54.33±62.91 | 44.45±55.23 | 0.41 | |
| Dysmenorrhea time (months)# | 24.44±44.86 | 18.62±34.86 | 0.47 |
| Dyspareunia time (months)# | 11.77±26.11 | 22.83±36.67 | 0.04 |
| Time pelvic pain (months)* | |||
| Size of endometrioma (cm)# | 4.15±3.13 | 4.1±2.98 | 0.87 |
Table 2: Characteristics of women with ovarian endometrioma according to presence of recurrence.
| n (%) | p* | RR | CI 95% | |
|---|---|---|---|---|
| Age (years) | ||||
| ≤ 30 | 31 (79.4) | 0.63 | 1.2 | 0.64-2.24 |
| > 30 | 8 (20.6) | |||
| Other outbreaks | ||||
| Yes | 29(74.3) | 0.03 | 1.86 | 1.03-3.37 |
| No | 10(25.7) | |||
| Treatment | ||||
| No | 3(7.7) | 0,89 | 2.19 | 0.77-6.21 |
| Yes | 36(92.3) | |||
| Size (cm) | ||||
| ≤ 3 | 14 (35.9) | 1 | 1 | 0.60-1.67 |
| > 3 | 25 (64.1) | |||
| Asymptomatic | ||||
| No | 37 (94.8) | 0.69 | 1.43 | 0.43-4.76 |
| Yes | 2(5.2) | |||
| Pregnancy after | ||||
| No | 38 (97.4) | 0.64 | 0.61 | 0.11-3.39 |
| Yes | 1 (2.6) | |||
| BMI | ||||
| ≤ 25 | 25(64.1) | 0.4 | 0.76 | 0.45-1.28 |
| > 25 | 14(35.9) | |||
| Prior surgery | ||||
| Yes | 23(58.9) | 0.3 | 1,35 | 0.82-2.22 |
| No | 16(41.1) | |||
Table 3: Factors associated with recurrence of ovarian endometrioma (n = 39).
Discussion
Our study demonstrated a recurrence of endometrioma in 40.2% of cases. There was a positive relationship between the recurrence of endometrioma and presence of other foci (p =0.03). Women showing evidence of other implants of endometriosis had an increased risk of recurrence of endometrioma 1.86. Therefore, women with early-stage endometriosis have a lower chance of recurrence than those with advanced stage disease. In the literature, there was also a stronger association between the recurrence of endometrioma and a more advanced stage of the disease [5, 8]. The literature also presents high recurrence rates, ranging from 30 to 50% [5, 6, 9, 10, 11]. One study showed recurrence rates that were lower than 20 % [12]. Concerning the time for recurrence, our study showed that the disease recurred after 34 months since surgery. Studies have shown that disease recurred earlier, at a period ranging from 20 to 32 months [5, 13, 14]. In a study with 167 patients that demonstrated recurrence in 50% of cases was observed that administration of postoperative hormonal therapy decreases the risk of recurrence [9]. Another study with 129 patients after laparoscopic excision of ovarian endometrioma revealed that endometrioma recurred in 18.6% of cases, and interruption of clinical treatment after surgery was the statistically significant risk factor. This study concluded that adjuvant treatment for endometriosis with oral contraceptives should be employed, since it seems to drastically reduce the relapse rate of ovarian endometrioma. This was not found in our sample. In this study, hormonal treatment interruption was the factor associated with a higher impairment after surgery treatment [12]. A study analyzed 87 women during a 24-month period following laparoscopic excision of ovarian endometrioma and showed that the risk of recurrence may be influenced by factors such as the administration of oral contraceptives. When administered for 24 months, the disease recurred in 2.9% of cases. In the patient group using contraceptives for some time, the recurrence rate was 14.3%. In contrast, the recurrence rate was 43.5% in patients who did not use oral contraceptives during the period of 24 months [13]. The relationship between a decreased recurrence risk and the administration of contraceptives was also demonstrated by a prospective Italian study of 168 patients. This study, however, attempted to demonstrate the relationship between different types of contraceptives. The cumulative risk of disease recurrence was: 74.7% for patients who did not use oral contraceptives; 26.5% for patients receiving daily doses of tablets with ethinyl estradiol and desogestrel 31.8% for patients receiving daily doses of tablets with ethinyl estradiol and gestodeno 20.5 % for patients receiving daily doses of tablets with estradiol valerate and dienogest [15]. In the majority of studies, the use of drugs that block menstruation is an important factor to prevent recurrence, a fact that was not observed in our study. This may be explained by the retrospective nature of the study, or by the small sample size when compared to the others. In a similar manner, the results of a study including 307 patients suggested that the recurrence rate of endometrioma after surgical excision was inversely related to patient age at the time of surgery and postoperative pregnancy [16]. In another study covering 248 women, the recurrence rate was 42%, which was similar to the rate found in our study. On the other hand, younger age at the time of diagnosis was considered a risk factor but it was not observed in our study. Pregnancy after surgery also seemed to be a protective factor [17], did not have the same impact in our sample. An important limitation of this study was the fact of the data acquisition is dependent upon information included in patient medical charts. Unfortunately, it is one of the major limitations of our methodology, since important information may be lost during the process. The strength of the study is decreased, making it more difficult to obtain statistically significant results. Due to the high rate of recurrence ovarian endometrioma must be carefully monitored especially in women with endometriosis in more advanced stages, since this disease involves an important pelvic pain and infertility. Although have not found factors related to recurrence, prospective studies are needed in order we can detect these factors in order to reduce the recurrence of endometrioma. Therefore, we may conclude that the recurrence rate of ovarian endometrioma was elevated. Women with advanced-stage endometriosis had a higher recurrence of the disease, and recurrence rate was higher at 2 years after surgery.
References
-
Crispi CP, Oliveira FMM, Junior Damiam JC, Oliveira MAP (2007) Endometriose. In: Tratado de videoendoscopia e cirurgia minimamente invasiva em ginecologia, (2ndedn ) Editora revinter, (capter 22), pp. 295-327.
-
Eskenazi B, Warner ML (1997) Epidemiology of endometriosi. Obstet Gynecol Clin North Am 24(2): 235-258.
-
Bulun SE (2009) Endometriosis, N England J Med 360(3): 268-279.
-
Sengoku K, Miyamoto T, Horikawa M, Katayama H, Nishiwaki K, et al. (2013) Clinicopathologic risk factors for recurrence of ovarian endometrioma following laparoscopic cystectomy. Acta Obstetricia et Gynecologica Scandinavica 92(3): 278-284.
-
Hayasaka S, Ugajin T, Fujii O, Nabeshima H, Utsunomiya H, et al. (2011) Risk factors for recurrence and re-recurrence of ovarian endometriomas after laparoscopic excision. J. Obstet. Gynaecol 37(6): 581-585.
-
Koga K, Takemura Y, Osuga Y, Yoshino O, Hirota Y, et al. (2006) Recurrence of ovarian endometrioma after laparoscopic excision. Human Reproduction 21(8): 2171-2174.
-
Hulley SB, Cummings SR, Browner WR, Grady D Hearst N, Newman TB (2008) Delineando a Pesquisa Clínica. (3rdedn), In: São Paulo: Artmed SA.
-
Dimitrijevic D, Vasiljevic M, Anicic R, Brankovic S, Ristic A, et al. (2015) Recurrence rate of ovarian endometriosis in patients treated with laparoscopic surgery and postoperative suppressive therapy 42(3): 339-343.
-
Ouchi N, Akira S, Mine K, Ichikawa M, Takeshita T (2014) Recurrence of ovarian endometrioma after laparoscopic excision: Risk factors and prevention. J. Obstet. Gynecol 40(1): 230-236.
-
Kikuchi I, Takeuchi H, Kitade M, Shimanuki H, Kumakiri J, et al. (2006) Recurrence rate of endometriomas following a laparoscopic cystectomy. Acta Obstet Gynecol Scand 85(9): 1120- 1124.
-
Liu X, Yuan L, Shen F, Zhu Z, Jiang H, et al. (2007) Patterns of and risk factors for recurrence in women with ovarian endometriomas. Obstet Gynecol 109(6): 1411-1420.
-
Carvalho MSR, Pereira AMG, Martins JA, Lopes RCG (2015) Predictive factors for recurrence of ovarian endometrioma after laparoscopic excision. Rev. Bras. Ginecol. Obstet 37(2): 77-81.
-
Takamura M, Koga K, Osuga Y, Takemura Y, Hamasaki K, et al. (2009) Post-operative oral contraceptive use reduces the risk of ovarian endometrioma recurrence after laparoscopic excision. Hum Reprod 24(12): 3042-3048.
-
Roman H, Quibel S, Auber M, Muszynski H, Huet E, et [INLINE_TABLE:5:0]
-
Cucinella G, Granese R, Calagna G, Svelato A, Saitta S, et al. (2013) Oral contraceptives in the prevention of endometrioma recurrence: does the different progestins used make a difference? Arch Gynecol Obstet 288(4): 821-827.
-
Yuan M, Wang W, Li Y, GAO L, Wang T, et al. (2014) Risk Factors Recurrence of Ovarian Endometriomas after Surgical Excision. J Huazhong Univ Sci Technol 34 (2): 213-219.
-
Sengoku K, Miyamoto T, Horikawa M, Katayama H, Nishiwaki K, et al. (2013) Clinicopathologic risk factors for recurrence of ovarian endometrioma following laparoscopic cystectomy. Acta Obstetricia et Gynecologica Scandinavica 92(2): 278-284.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’