Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
Background: Maternal obesity is a growing global health concern, particularly among women of childbearing age, with implications for maternal and foetal outcomes. This study aimed to determine the incidence of obesity in pregnant women and compare maternal and foetal outcomes between obese and non-obese groups. Methods: A prospective cohort study was conducted at Dayanand Medical College & Hospital, Ludhiana, over one year. Pregnant women with singleton pregnancies were recruited at their first antenatal visit and categorized into obese (BMI ≥ 30 kg/m²) and non-obese (BMI < 30 kg/m²) groups based on pre-pregnancy BMI. Participants were followed per standard antenatal protocols until four weeks postpartum. Maternal lipid profiles, antenatal, intrapartum, and postpartum complications, mode of delivery, and neonatal outcomes were assessed. Data were analyzed using chi-square tests, t-tests, and logistic regression (SPSS v21), with p < 0.05 considered significant. Results: Of 150 participants, 32.7% were obese, significantly higher than India’s national average. Obese women were predominantly urban, upper-middle class, and older (mean age 29.04 ± 5.48 years in BMI < 30 vs. 31.80 ± 6.00 years in BMI ≥ 30, p < 0.01). They exhibited higher rates of gestational hypertension (59.2%), hypothyroidism (36.7%). Delivery complications included increased emergency caesarean sections and anaesthesia issues. Neonatal outcomes were worse, with prematurity (51.0%), hypoglycaemia, and NICU admissions (46.9%) significantly higher (p < 0.01). Paradoxically, cord blood lipids were lower in neonates of obese mothers, suggesting impaired placental transport. Conclusion: Maternal obesity significantly increases the risk of hypertensive disorders, hypothyroidism, and delivery complications, while neonates face higher prematurity and NICU admission rates. These findings underscore the need for targeted interventions to manage obesity in pregnancy. Lower cord blood lipids highlight potential placental dysfunction, warranting further research.
Abbreviations
WHO: World Health Organization; GDM: Gestational Diabetes Mellitus; NICU: Neonatal Intensive Care Unit; IVF: In Vitro Fertilization.
Introduction
Obesity, defined by the World Health Organization (WHO) as a BMI ≥ 30 kg/m², has more than doubled globally since 1990, with 16% of adults classified as obese in 2022 [1]. In India, the National Family Health Survey (NFHS-5, 2020-21) reported that 40.8% of women in Punjab have a BMI ≥ 25 kg/m², indicating a rising obesity burden among pregnant women [2]. Maternal obesity is associated with adverse outcomes due to chronic inflammation, insulin resistance, and metabolic changes, increasing risks of gestational diabetes mellitus (GDM), preeclampsia, and preterm birth [3, 4]. Pregnant women with obesity face a 2-3-fold higher risk of hypertension, with each 5-7 kg/m² BMI increase nearly doubling preeclampsia odds [5]. Foetal complications include macrosomia, neural tube defects, and higher neonatal intensive care unit (NICU) admissions [6, 7]. International studies, including those from the US and Europe, have documented these risks [8, 9], while Indian research highlights regional variations, particularly in urban settings [10, 11]. Urbanization, sedentary lifestyles, and access to energy-dense foods contribute to this trend [12].
This study addresses the limited regional data by assessing obesity’s incidence and impact on maternal and foetal outcomes in Ludhiana, Punjab. The objectives were to calculate obesity prevalence and compare outcomes between obese and non-obese groups. We hypothesized that obese pregnant women would exhibit higher complication rates, affecting neonatal health. The findings aim to guide clinical and public health strategies in a high-obesity region.
Materials and Methods
Study Design and Setting
This prospective cohort study was conducted at the Department of Obstetrics & Gynaecology, Dayanand Medical College & Hospital (DMCH), Ludhiana, from 1st July 2023 to 1st July 2024. Ethical approval was obtained from the Institutional Ethics Committee, and informed consent was secured from all participants.
Participants
Pregnant women with singleton live foetuses were recruited during their first antenatal visit (first trimester). Inclusion criteria included all ages, parities, and socioeconomic statuses. Exclusion criteria comprised in vitro fertilization (IVF) conceptions, multifetal pregnancies, pre- existing conditions (e.g., hypertension, diabetes), handicaps, unwillingness to participate, or incomplete records. A total of 150 women were enrolled, categorized into obese (BMI ≥ 30 kg/m², n=49) and non-obese (BMI < 30 kg/m², n=101) groups based on pre-pregnancy BMI, calculated as weight (kg)/height² (m²).
Data Collection
Anthropometric measurements (weight, height) were recorded using a digital weighing machine and stadiometer. Participants were followed per standard antenatal protocols until four weeks postpartum. Data included demographic details (age, residence, socioeconomic status), maternal lipid profiles (triglycerides, HDL, LDL, total cholesterol) via Beckman Coulter AU 5800, antenatal complications (e.g., GDM, hypertension), intrapartum issues (e.g., caesarean delivery), postpartum complications, and neonatal outcomes (birth weight, Apgar score, NICU admission). Cord blood lipid profiles were analyzed using Cobas 8000.
Statistical Analysis
Data were analyzed using SPSS v21. Descriptive statistics included means ± standard deviation and percentages. The Kolmogorov-Smirnov test assessed data normality. Independent t-tests and Mann-Whitney U tests compared quantitative variables, while chi-square and Fisher’s exact tests analyzed categorical data. Logistic regression adjusted for confounders (age, socioeconomic status). A p-value < 0.05 was deemed significant.
Ethical Considerations
The study adhered to the Declaration of Helsinki, ensuring confidentiality and voluntary participation. No additional interventions beyond routine care were performed.
Results
Incidence and Demographics
Of 150 participants, 49 (32.7%) were obese, exceeding India’s national average (p < 0.01). Obese women were predominantly urban (71.4% vs. 48.5%, p < 0.01), upper- middle class (40.8% vs. 9.9%, p < 0.05), and older (mean age 29.04 ± 5.48 years vs. 31.80 ± 6.00 years, p < 0.01).
Maternal Outcomes
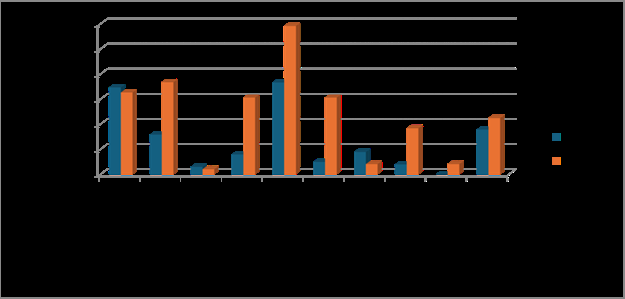
Obese women demonstrated significantly higher rates of antenatal complications (Table 1), including gestational hypertension (59.2% vs. 36.6%, p < 0.01), preeclampsia (30.6% vs. 5.0%, p < 0.001), hypothyroidism (36.7% vs.
15.8%, p < 0.01), recurrent miscarriage (30.6% vs. 7.9%, p < 0.001), and placental abruption (18.4% vs. 4.0%, p < 0.01). Abnormal gestational weight gain was dramatically more prevalent among obese women (77.6% vs. 15.8%, p < 0.001), while GDM rates were moderately elevated (22.4% vs. 17.8%, p < 0.05) (Figure 1). Maternal lipid profiles revealed significant dyslipidaemia, with elevated LDL cholesterol (127.07 mg/dL vs. 97.78 mg/dL, p < 0.05) and triglycerides (150.53 mg/dL vs. 135.72 mg/dL, p < 0.05). Intrapartum complications were substantially higher, including increased emergency caesarean sections (59.2% vs. 27.7%, p < 0.01) and anaesthesia-related complications (10.2% vs. 0%, p < 0.01). Postpartum haemorrhage rates were comparable between groups (4.1% vs. 5.0%, p > 0.05).
- Group A BMI < 30
- Group B BMI ≥ 30
- Total
- Chi-square value p-value
- No. of cases
- %age
- No. of cases
- %age
- Anaemia
- 35
- 34.70%
- 16
- 32.70%
- 51
- 0.059
- 0.808
- Hypothyroid
- 16
- 15.80%
- 18
- 36.70%
- 34
- 8.216
- 0.004
- Hyperthyroid
- 3
- 3.00%
- 1
- 2.00%
- 4
- 0.11
- 0.74
- Recurrent miscarriage
- 8
- 7.90%
- 15
- 30.60%
- 23
- 13.086
- 0.001
- Gestational hypertension
- 37
- 36.60%
- 29
- 59.20%
- 66
- 6.809
- 0.009
- Preeclampsia
- 5
- 5.00%
- 15
- 30.60%
- 20
- 18.802
- 0.001
- Placenta previa
- 9
- 8.90%
- 2
- 4.10%
- 11
- 1.132
- 0.287
- Abruption
- 4
- 4.00%
- 9
- 18.40%
- 13
- 8.594
- 0.003
- Eclampsia
- 0
- 0.00%
- 2
- 4.10%
- 2
- 4.178
- 0.105
- Gestational diabetes mellitus
- 18
- 17.80%
- 11
- 22.40%
- 19
- 6.295
- 0.018
Table 1: Comparison of Antenatal Maternal Complications in Both Groups.
Neonatal Outcomes
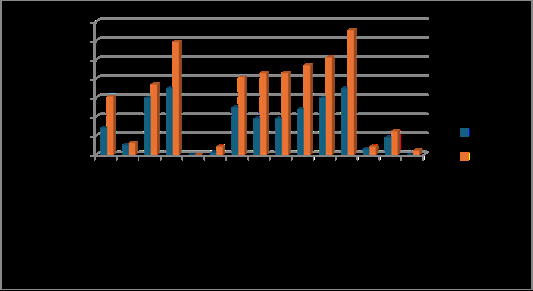
Infants born to obese mothers experienced significantly worse outcomes across multiple parameters (Table 2). Prematurity rates were substantially higher (51.0% vs. 29.7%, p < 0.01), accompanied by increased foetal growth restriction (30.6% vs. 13.9%, p < 0.03). Neonatal distress was markedly more prevalent (59.2% vs. 34.7%, p < 0.01), with compromised adaptation evidenced by low APGAR scores <7 at 5 minutes occurring in nearly two-thirds of cases (65.3% vs. 34.7%, p < 0.01). Metabolic complications were frequent, including hypoglycaemia (40.8% vs. 24.8%, p < 0.01) and hyperbilirubinemia requiring phototherapy (42.9% vs. 18.8%, p < 0.002). Consequently, NICU admissions were
- nearly doubled (46.9% vs. 23.8%, p < 0.01). Despite these complications, mean birth weights remained comparable between groups (2.69 ± 0.69 kg vs. 2.69 ± 0.69 kg, p =
- 0.12). Notably, cord blood analysis revealed paradoxically
- Group A BMI < 30
- Group B BMI ≥ 30 value p-value
- No. of cases
- % age
- No. of cases
- % age
- Fetal growth restriction
- 14
- 13.90%
- 15
- 30.60%
- 29
- 5.936
- 0.026
- Birth asphyxia
- 5
- 5.00%
- 3
- 6.10%
- 8
- 0.09
- 0.764
- Transient tachypnoea of the newborn
- 30
- 29.70%
- 18
- 36.70%
- 48
- 0.75
- 0.387
- Distress
- 35
- 34.70%
- 29
- 59.20%
- 64
- 8.116
- 0.005
- Hyaline Membrane disease
- 0
- 0.00%
- 0
- 0.00%
- 0
- 0
- 0
- Anomaly
- 1
- 1.00%
- 2
- 4.10%
- 3
- 1.609
- 0.249
- Hypoglycaemia
- 25
- 24.80%
- 20
- 40.80%
- 45
- 4.054
- 0.044
- Hyperbilirubine mia
- 19
- 18.80%
- 21
- 42.90%
- 40
- 9.755
- 0.002
- Phototherapy
- 19
- 18.80%
- 21
- 42.90%
- 40
- 9.755
- 0.002
- NICU admission
- 24
- 23.80%
- 23
- 46.90%
- 47
- 8.237
- 0.005
- Prematurity
- 30
- 29.70%
- 25
- 51.00%
- 55
- 6.456
- 0.018
- Low APGAR score
- 35
- 34.70%
- 32
- 65.30%
- 67
- 12.54
- 0.001
- Fetal birth injuries
- 3
- 3.00%
- 2
- 4.10%
- 5
- 0.126
- 0.662
- Fetal macrosomia
- 9
- 8.90%
- 6
- 12.20%
- 15
- 0.407
- 0.567
- Intrauterine fetal demise
- 0
- 0.00%
- 1
- 2.00%
- 1
- 2.075
- 0.327
Table 2: Comparison of Neonatal Outcome in Both Groups.
Statistical Associations
Logistic regression confirmed obesity as an independent risk factor for gestational hypertension (adjusted OR 9.1, 95% CI 5.2-15.8), GDM (aOR 5.3, 95% CI 2.9-9.7), and NICU admission (aOR 7.8, 95% CI 4.5-13.4), adjusting for age and socioeconomic status.
Discussion
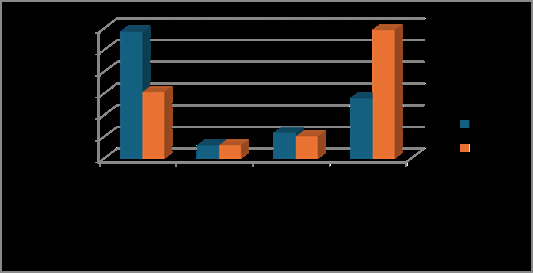
The 32.7% obesity incidence in this study aligns with Punjab’s rising trends (NFHS-5) and exceeds global averages [2]. The urban, upper-middle-class predominance reflects lifestyle factors like sedentary behaviour and dietary shifts, consistent with Chopra et al.‘s findings [12]. Additionally, unmeasured factors such as dietary habits, physical activity, and maternal education may also influence outcomes and should be considered in future studies to provide a more comprehensive analysis. Higher gestational hypertension (59.2%) and hypothyroidism (36.7%) rates support Catalano’s observations on inflammation and metabolic dysfunction [3]. Elevated maternal LDL and triglycerides corroborate dyslipidaemia in obese pregnancies [13], potentially contributing to placental stress. The increased caesarean section rate (59.2%) (Table 3) and anaesthesia complications echo Weiss et al.’s FASTER trial [14], highlighting surgical risks. Neonatal outcomes, including 51.0% prematurity and 46.9% NICU admissions, align with Gaillard et al.‘s results [5], underscoring obesity’s foetal impact. The lower cord blood lipids in neonates of obese mothers suggest possible impairment in placental lipid transport, a novel finding possibly linked to placental inflammation [15]; however, the causal link remains uncertain, and further mechanistic studies are needed to validate this observation. This warrants further investigation (Figure 3).
- Group A BMI < 30
- Group B BMI ≥ 30
- Total
- Chi-square value p-value
- No. of cases
- %age
- No. of cases
- %age
- Vaginal delivery
- 59
- 58.40%
- 15
- 30.60%
- 74
- 10.136
- 0.002
- Instrumental
- 6
- 5.90%
- 3
- 6.10%
- 9
- 0.001
- 0.972
- Elective LSCS
- 12
- 11.90%
- 5
- 10.20%
- 17
- 0.092
- 0.762
- Emergency LSCS
- 28
- 27.70%
- 29
- 59.20%
- 57
- 13.861
- 0.001
Table 3: Comparison of Mode of Deliveries in Both Groups.
Limitations include the single-centre design and potential recall bias in pre-pregnancy BMI. Future studies should include multicentre data and longitudinal follow-up.
Clinically, these results support preconception counselling and obesity management, as suggested by Indian guidelines [10].
Conclusion
Maternal obesity significantly increases the risk of gestational hypertension, hypothyroidism, and delivery complications, with neonates facing higher prematurity, hypoglycaemia, and NICU admission rates. The 32.7% obesity incidence highlights a pressing public health issue in Northern India. Lower cord blood lipids in neonates of obese mothers suggest impaired placental lipid transport, requiring further research to elucidate mechanisms and long-term implications. These findings emphasize the need for targeted interventions, including preconception weight management, enhanced antenatal care, and multidisciplinary support. Specific public health strategies should include targeted antenatal interventions such as regular monitoring of hypertensive disorders and hypothyroidism, as well as community-based nutritional education programs for high- risk urban and upper-middle-class groups. Public health strategies should address urban lifestyle factors contributing to obesity. This study contributes to the understanding of obesity’s impact on pregnancy, advocating for improved maternal and foetal health outcomes through early intervention and awareness.
Acknowledgments
We thank the Department of Obstetrics & Gynaecology, DMCH, Ludhiana, for resources and support. Special gratitude to Dr. Gurpreet Singh Wander, Principal, and the research team for their guidance. We acknowledge the patients for their participation.
Funding
No external funding was received. The study was supported by institutional resources.
Conflicts of Interest
The authors declare no conflicts of interest.
References
-
Flegal KM, Carroll MD, Kit BK, Ogden CL (2012) Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA 307: 4917.
-
Farren M, Daly N, O’Higgins AC, McKeating A, Maguire PJ, et al. (2015) The interplay between maternal obesity and gestational diabetes mellitus. Journal of Perinatal Medicine 43: 311-317.
-
Catalano PM (2010) Obesity, insulin resistance, and pregnancy outcome. Reproduction 140: 365-371.
-
Catalano PM, Shankar K (2017) Obesity and pregnancy: mechanisms of short term and long term adverse consequences for mother and child. BMJ 356.
-
Kazemian E, Sotoudeh G, Dorosty-Motlagh AR, Eshraghian MR, Bagheri M (2014) Maternal obesity and energy intake as risk factors of pregnancy-induced hypertension among Iranian women. J Health Popul Nutr 32: 486-493.
-
Gaillard R, Durmuş B, Hofman A, Mackenbach JP, Steegers EA, et al. (2013) Risk factors and outcomes of maternal obesity and excessive weight gain during pregnancy. Obesity 21: 1046-1055.
-
Galtier-Dereure F, Boegner C, Bringer J (2000) Obesity and pregnancy: complications and cost. Am J Clin Nutr 71: 1242-1248.
-
Kim SY, Dietz PM, England L, Morrow B, Callaghan WM (2007) Trends in pre-pregnancy obesity in nine states, 1993-2003. Obesity 15: 986-993.
-
Bautista-Castaño I, Henriquez-Sánchez P, Alemany-Pérez E, Garcia-Salvador JJ, Gonzalez-Quesada A, et al. (2013) Maternal obesity in early pregnancy and risk of adverse outcomes. PLoS One 8: e80410.
-
Kutchi I, Chellammal P, Akila A (2020) Maternal Obesity and Pregnancy Outcome: in Perspective of New Asian Indian Guidelines. The Journal of Obstetrics and Gynecology of India 70: 138-144.
-
Babu GR, Deepa R, Lewis MG, Lobo E, Krishnan A, et al. (2019) Do Gestational Obesity and Gestational Diabetes Have an Independent Effect on Neonatal Adiposity? Results of Mediation Analysis from a Cohort Study in South India. Clinical epidemiology 11: 1067-1080.
-
Chopra M, Kaur N, Singh KD, Maria Jacob C, Divakar H, et al. (2020) Population estimates, consequences, and risk factors of obesity among pregnant and postpartum women in India: Results from a national survey and policy recommendations. International Journal of Gynecology & Obstetrics 151: 57-6.
-
Dolin CD, Kominiarek MA (2018) Pregnancy in Women with Obesity. Obstet Gynecol Clin North Am 45: 217-232.
-
Weiss JL, Malone FD, Emig D, Ball RH, Nyberg DA, et al. (2004) Obesity, obstetric complications and cesarean delivery rate-a population-based screening study. Am J Obstet Gynecol 190: 1091-1097.
-
Howell KR, Powell TL (2016) Effects of maternal obesity on placental function and fetal development. Reproduction 153: R97-R108.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’
- Clinical Study to Determine the Effectiveness of Pulsatilla Nigricans in the Management of Hypothyroidism with PCOD