‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’
Normoprolactinemic hypogonadotropic hypogonadismis (HH) a germanely frequent etiology of anovulation. It originates from pituitary and /or suprapituitary structures. Besides hyperprolactinemia, ovulation induction by gonadotropins or pulsatile gonadotropin-releasing hormone (GnRH) delivery might be posited in women who want pregnancy. The choice of ovulation induction medications are based on the region of the gonadotropic axis impacted: pulsatiledelivery of GnRH might just be taken into account in suprapituitary etiologes, while injectable gonadotropins possess the capacity of getting utillized in both suprapituitary and pituitary etiologes. Hypothalamic anovulation is usually categorized into congenital and acquired etiologies .In case of acquired normoprolactinemic HH, organic etiologies are compared to functional hypothalamic amenorrhea (FHA). FHA takes place by diminished pulsatilityof GnRH leading to a diminished frequency and amplitude of luteinizing hormone (LH) pulses. Restriction of fat intake and/or increased physical activity is implicated in such diminished pulsatility. The phenotypic expression of suprapituitary congenital hypogonadotropic hypogonadism (CHH) might differ. An escalating number of genes are implicated in the migration of GnRH neurons at the time of intrauterine life in addition to / or in the homeostasis of the gonadotropic axis are isolated. Till now, practically 50%of corroborated cases of CHH continue to be idiopathic subsequent to genetic evaluation.No studies have contrasted the efficacy of pulsatile GnRH delivery as per the etiology of suprapituitary anovulation or tried to isolate prognostic factors for the success of this treatment. Recently in a retrospective cohort study at France, the ongoing pregnancy rate per initiated cycle amongst FHA and CHH patients was contrasted subsequent to treatment with pulsatile GnRH delivery aiming for monofollicular ovulation. Comparable outcome were seen in FHA and CHH, advocating its superiority over gonadotropins and IVF.
Abbreviations
FHA: Functional Hypothalamic Amenorrhea; IHH: Idiopathic Hypogonadotropic Hypogonadism; KS: Kallmann Syndrome; FGF8: Fibroblast Growth Factor 8; FGFR1: Fibroblast Growth Factor Receptor 1; HS6T1: Heparin Sulfate-6-O-Transferase; GNRHR: Gonadotropin Releasing Hormone Receptor; CHH: Congenital Hypogonadotropic Hypogonadism; FHA: Functional Hypothalamic Amenorrhea; OPR: Ongoing Pregnancy Rates; LH: Luteinizing Hormone; OB: Olfactory Bulb; AN: Anorexia Nervosa; IVF: In vitro Fertilization; OHSS: Ovarian Hyperstimulation Syndrome; LBR: Live Birth Rates; ART: Assisted Reproductive Technology.
Introduction
Earlier we had reviewed regarding how patients of anorexia nervosa (AN) who present with primary/ secondaryhypothalamic amenorrhoea were substantially recalcitrant to any forms of treatment. Furthermore, we detailed -an update on aetiopathogenesis, endocrine profile and management of hypothalamica amenorrhea with the part of pulsatile GnRH in its treatment [1, 2, 3]. Additionally, besides describing the part of Kisspeptins (kp) in human reproduction [4], wecomprehensively described, aetiopathogenesis of Idiopathic hypogonadotropic hypogonadism (IHH) -apart from the 9 widely acknowledged mutations for Kallmann Syndrome (KS) for instance KAL1, Fibroblast growth factor 8 (FGF8), fibroblast growth factor receptor 1(FGFR1), prokineticin 2 (PROK2), PROK receptor 2 (PROKR2), WDR11, heparin sulfate-6-O-Transferase (HS6T1), chromodomain helicase DNA binding protein 7 (CHD7) as well as semaphorin 3A (SEMA 3A), extra mutations in “FGF8 synexpression” group for instance FGF 17, ILRD, dual specificphosphatase -8(DUSP6), SPRY4 in addition to FLRT3 have been illustrated to be implicated in congenital hypogonadotropic hypogonadism (CHH), usually KS apart from semaphorin 7A (SEMA 7A). Despite, canonically further classification were dependent on anosmic/normosmic guidelines , greater genes were observed to result in nIHH disorders for instance Gonadotropin releasing hormone receptor (GNRHR). KISS1, TAC3, TACR3 werefurther observed to be correlated with hyposmia on exhaustive evaluation on university of Pennsylvania Smell IdentificationTest (UPSIT) along with MRI in reference to olfactory structure abnormalities displayed eliminated olfactory bulb (OB).
Therapy with recombinant follicle stimulating hormone (rFSH) / human chorionic Gonadotropins (hCG) yields practically akin outcomes obtained to administration of GnRH in the form of pulses (alias pulsatile GnRH therapy in addition have requirement to be dependent on cost factor, accessiblity as well as in rare instances particularly for say in case of kp along with NKB mutations kisspeptin therapy is advocated [5, 6]. Therefore, in contrast to canonical thought process there is need for changing this classification were the conclusions drawn by us in 2016 instead of dependent on absence/no absence of smell (that is anosmic/ normosmic classification simply as KS. Requirement for evaluating mutations for instance in Sox10/CHD7/ILRD7 is mandatory in the presence of deafness taking into account 38% correlation with them. Therapy should be personalized dependent on accessiblity of pulsatile GnRH, cost viability as well as in tough subjects,whereas in case of subjects with kp along with NKB mutations, kp therapy might be utilized [5, 6]. Maximum work on IHH therapy has been done by the group of Pitteloud N, Dwyer AA, Crowley Jr WF(reviewed in details in) [6, 7, 8].
Hypogonadotropic hypogonadismis(HH) with normal prolactin quantities (alias Normoprolactinemic HH) portrays a germanely frequent etiology of anovulation. Its initiation takes place at the pituitary as well as /regions above pituitary structures. Besides therapy for hyperprolactinemia, ovulation induction by gonadotropins or pulsatile gonadotropin- releasing hormone (GnRH) delivery might be posited in women who want pregnancy. The choice of ovulation induction medications are based on the region of the gonadotropic axis impacted: Pulsatile delivery of GnRH might just be above the pituitary taken into account the hypothalamic cause of the so called hypothalamic pituitary-ovarian(H-P-O) axis etiologes, while administration of gonadotropins by injection possess the capacity of getting utillized in both above the pituitary (hypothalamic alias suprapituitary) along with pituitary etiologes [9]. Anovulation in view of hypothalamic etiologes is usually categorized into i)problems by birth (namely congenital group) along with ii)causes whose acquisition occurs subsequent to birth( namely acquired group) [10, 11]. In case of acquired HH group secondary to normal prolactin quantities, subjects having particular causes are compared to those without any causes get labelled as functional hypothalamic amenorrhea (FHA). FHA takes place by diminished pulsatility of GnRH leading to a diminished frequency in addition to height reached by LH pulses [12]. Restriction of fat intake as well as as/or increased physical activity is implicated in such diminished pulsatility [12, 13]. Thereby the expression of phenotype in CHH subjects where etiological factor was above the pituitary might differ [14]. For the GnRH neurons migration which takes place at the time of intrauterine life in addition to / in the homeostasis of the gonadotropic axis escalating numbers of genes have been isolated [6, 14]. Till now, practically 50% of corroborated cases of CHH continue to be idiopathic subsequent to genetic evaluation. Practically negligible studies have contrasted the efficacy of administration of GnRH in the form of pulses in reference to as per the causative factor of anovulation above the pituitary /tried to isolate factors responsible for prognosis or the outcomes obtained of such treatment.
Methods
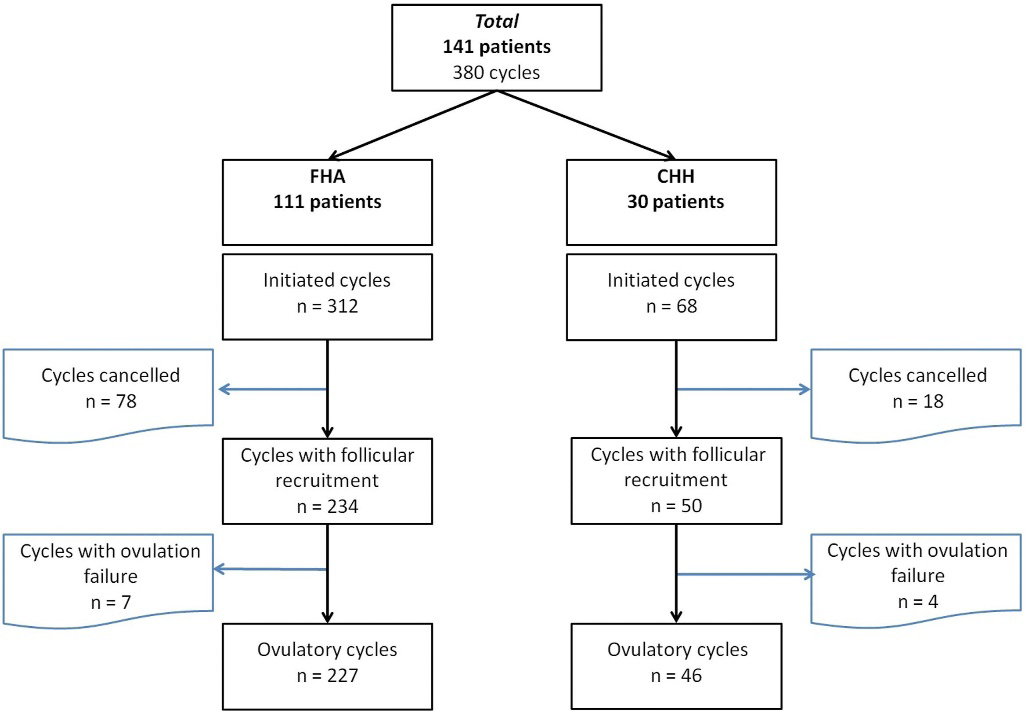
A retrospective single centred cohort study was performed by Everaere H, et al. [15], at the University Hospital of Lille from 2004 to 2022. A total of 141 patients who had been diagnosed with central suprapituitary amenorrhea at the time of infertility asssessment as well as followed by therapy with pulsatile GnRH therapywere recruited. 111 in addition to 30 cases were diagnosed with FHA or CHH, respectively.
The basic objective of their work was to contrast the ongoing/continuing pregnancy rate (OPR) per started cycle amongst subjects with FHA as well as CHH subsequent to treatment with administration of GnRH in the form of pulses. The objective of the treatment was to further attain just monofollicular ovulation [15]. The evaluation was inclusive of 380 cycles of delivery of pulsatile GnRH in case of 141 patients amongst time period of 2004 till 2022. Patients with FHA (n =111) were included dependent on serum proof of hormonal HH (lesser estradiol, follicle stimulating hormone (FSH) in addition to LH), with secondary hypoestrogenic amenorrhea of a minimal of 6 months along with the existence of dietary curtailing, weight reduction reaching significance physical overeractivity (Figure 1).
Results
Ongoing pregnancy rates (OPR) per started cycle were proportionate amongst groups: illustrated 21.5% in the FHA group vis a vis 22% in the CHH group. Contrasting the baseline properties illustrated that a greater prominent follicle-stimulating hormone (FSH) deficiency was observed in patients with CHH in contrast to those with FHA: 2.55 (0.6–4.92) vis a vis 4.80 (3.90–5.70) UI/L. amongst the CHH group, basal FSH quantities were positively correlated with the OPR (odds ratio, 1.57; 95% confidence interval, 1.11– 2.22). In the CHH group, the time period of treatment was greater in contrast to the FHA group: 23.59 ( 8.02) vs. 18.16 ( 7.66) days.
Out of the 30 patients with CHH, the maximum 19 presented with a diagnosis of normosmic(aliasnormal smell) kind of idiopathic CHH. Further 5 patients presented with a diagnosis of KS, as well as 6 presented with complete / partial GnRH gene mutations. Intravenously(iv) delivery was the route of delivery starting 2004 till 2010, for the administration of GnRH in the form of pulses in form of gonadorelin.
Subsequent to 2010, the route of delivery got changed to subcutaneous(s/c)using a pump, with the dosage/ pulse determined by body mass index (BMI), antimullerian hormone (AMH) quantities, in addition to/or antral follicle count (AFC) possessed by patient. Sustenance of pulsatile GnRH therapy was done till 5 days subsequent to the anticipated date of ovulation.On corroborating ovulation by escalated serum progesterone quantities, luteal phase intramuscular urinary hCG delivery was provided for 11 days postovulation to buttress luteal phase. Baseline patient properties were pronounced for a commensurate average age amongst the 2 groups along with a lesser mean BMI amongst patients with FHA in contrast to those with CHH. For iv gonadorelin particularly, the baseline and average daily dose, in addition to the time period of treatment total ultrasound examinations required , were all greater in patients with CHH in contrast to those with FHA (P<.001). Nevertheless, doses of gonadorelin were not statistically variable amongst the 2 groups when the route of administration was subcutaneous. Despite those variation the proportion of ovulatory cycles with monofollicular growth was commensurate amongst the 2 groups:64.7%in those with CHH along with 60.9%in those with FHA (P=ns).
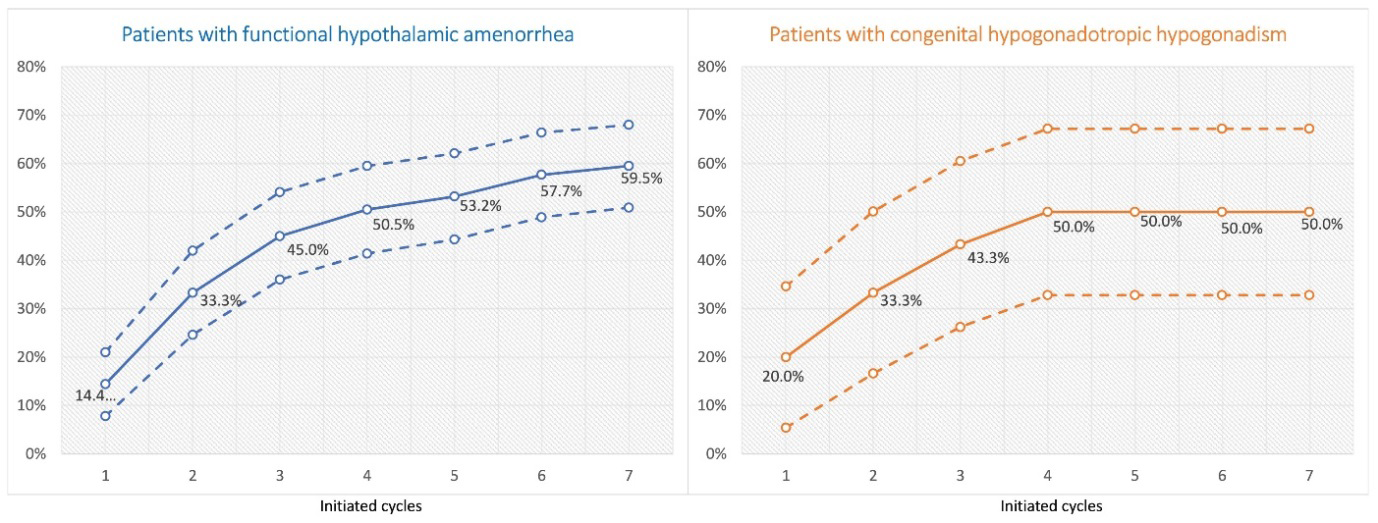
Figure 2: Courtesy Ref No-15- Cumulative Ongoing Pregnancy Rates Per Initiated Cycle. The Graph on the Left Represents the Group of Patients with Functional Hypothalamic Amenorrhea, and the Graph on the Right Represents the Group of Patients with Congenital Hypogonadotropic Hypogonadism. Data are Presented as Percentages (Solid Curves), with 95% Confidence Intervals (Dashed Curves).
The basic outcome of ongoing pregnancy rates (OPR/ cycle was further commensurate amongst 2 groups : 22% in patients with CHH as well as 21.5% in patients with FHA (P=ns). Fifty % of all patients attained an ongoing pregnancy subsequent to 4 cycles, with no variations in cumulative OPR/ rates of cycles needing cancellation amongst the 2 groups. Lastly ,among patients with CHH, a higher basal FSH quantities were observed to be anticipative of pregnancy subsequent to pulsatile GnRH delivery, Everaere H, et al. [15], posited this pointed to a higher expression of GnRH receptors in such patients’ gonadotropic cells following GnRH delivery compared to gonadotropins therapy perse [15].
Discussion
HH represents a disorder having properties of insufficiency with regards to liberation / working of GnRH, leading to lesser quantities of gonadotropin as well as, diminished ovarian working along with anovulation. This disorder is usually classified into 2 major kinds : FHA in addition to CHH [15]. The acquired as well as greater frequent kind, FHA, is usually reversible along with gets impacted by significant fat in addition to restricting calories as well as escalated exercise/stress pushing towards(AN [12]. Each of these factors possess the capacity of autonomously resulting in a reduced pulsatility of GnRH, leading to lesser amplitude in addition to of luteinizing hormone (LH) pulses frequency [15]. As compared to FHA, CHH represents an occasional, chronic disorder in view of an acknowledged genetic mutation canonically leading to the generation or physiology of the H-P-O axis. Although, the isolation of an escalating genes quantities correlated with CHH, practically 50% of all diagnosed CHH cases continue to bewith uncharted causative genes [16]. The pathophysiological differentiation amongst such 2 kinds of HH is significant. Thereby getting insight, has significance in view of them possessing the capacity of influencing diagnosis as well as affecting treatment strategy in addition to management. Despite ,no availability in the United States America (USA), pulsatile GnRH delivery is an efficacious treatment for central anovulation of hypothalamic origin as well as is frequently utilized in certain European countries, inclusive of Germany, Austria, France, along with the Holland & others [15, 17]. An earlier meta-analysis performed by Tranoulis A, et al. [18], illustrated that administration of GnRH in the form of pulses provides ovulation as well as live birth rates (LBR) in each cycle akin to those ladies having normal ovulatory cycles; particularly, rate of ovulation75.6% amongst CHH ladies in addition to 85.2% in FHA ladies respectively along with a LBR in each cycle of about 35% [18].
Despite, the study is limited in view of its retrospective design in addition to being a single-center study rather than involving multiple centers, its major strength is undeniably the clinical relevance to therapy with pulsatile GnRH delivery in the form of an efficacious as first-line treatment for patients with CHH as well as FHA who had not got outcomes obtained as pregnancy attained with lifestyle modifications. The favourable observations of this study highlight the plausible significance of making pulsatile GnRH therapy more broadly accessible, specifically by advocating for its approval in USA where it is at present not available. Having accessiblity to pulsatile GnRH therapy might significantly affect clinical setting by yielding patients an other option in addition to option needing lesser invasive technology both for ovulation induction without the need for exogenous gonadotropins as well as IVF &correlated risk of multiple pregnancies.
Conclusions
Despite ovulation induction by injecting gonadotropins along with combination treatment in vitro fertilization (IVF) have undoubtedly given breakthrough therapy in reproductive medicine, a strategy of using GnRH therapy might idealize outcomes obtained whereas guaranteeing least inimical sequelae.
Furthermore, it continues to be imperative to pursue generating as well as provide safety , along with othertherapies for cases that might have predilection for methodologies separate from assisted reproductive technology (ART) in view of religious thoughts, individual values, or wanting something akin to natural method of conception. Therefore, for person’s having CHH in addition to FHA, GnRH therapy pulses are considerably attractive because of safety along with efficacious treatment option for both situations as well as mandates wider adoption in addition to accessibility [19]. Thus since pulsatile GnRH therapy is expensive and not available in India as well apart from United States America (USA) one needs to see its promise in avoidance of IVF which might be equally cost prohibitive to try getting accessibility in countries where no availability as it gives a chance of success in most patients,avoiding Ovarian hyperstimulation Syndrome (OHSS), multiple pregnancies in either group. Despite our stressing not to use anosmic/normosmic criteria, in view of additional genes observed to result in so called nIHH like GnRHreceptor (GNRHR). KISS1, TAC3, TACR3 have further been observed to be correlated with hyposmia on exhaustive evaluation on UPSIT andMRI for olfactory structures displayed eliminated OB.
Everaere H, et al. [15], used the criteria of KS as hyposmia /normosmia only in their selection of patients with CHH. However their results were more specific for patients’ seeking infertility treatment, highlighting how in either FHA or CHH pulsatile GnRH therapy is efficacious although more so in FHA without any statistically significant variation.Therefore as far as infertility treatment is concerned it cuts down on cost of therapy vis a vis IVF. Nevertheless, for CHH patients it is essential to isolate &diagnose as early as possible in view of in males non descent of testis might result in azoospermia& start therapy before minipuberty is achieved(reviewed by us in ref no) Kochar K, et al. [20, 21], and latest in detail in ref Rohayem J, et al. [22].
References
-
Kochar Kaur K, Allahbadia GN, Singh M (2017) Therapeutic Impact of Dysfunction in Reward Processing in Anorexia Nervosa - A Mini Review. Ann Nutr Disord & Ther 4(2): 1045.
-
Kochar Kaur K, Allahbadia GN, Singh M (2022) Therapeutic applications of recent advancements in insight regarding mechanisms of development of Anorexia Nervosa: implications in the management and development of biomarkers for early detection besides avoidance of neonatal malformations-A Short Communication. Journal of Internal Medicine & Health Affairs 1(1).
-
Kochar Kaur K, Allahbadia GN, Singh M (2016) Hypothalamic Amenorrhea-an Update on Aetiopathogenesis, Endocrine Profile and Management. J Gynecol 1: 1.
-
Kochar Kaur K, Allahbadia GN, Singh M (2012) Kisspeptins in Human Reproduction-Future Therapeutic Potentials. Journal of Assisted Reproduction and Genetics 29: 999-1011.
-
Kochar Kaur K, Allahbadia GN, Singh M (2014) Male Hypogonadism-Areview ofSecondary Hypogonadism with Special Emphasis on Hypogonadotropic Hypogonadism. Journal of Endocrinology, Diabetes & Obesity 2: 1023.
-
Kochar Kaur K, Allahbadia GN, Singh M (2016) Idiopathic hypogonadotropic hypogonadism- an update on the aetiopathogenesis,management of IHH in both males and females-an exhaustive review. Advances in SexualMedicine 6: 50-78.
-
Pitteloud N, Hayes FJ, Boeoole PA, DeCruz S, Seminara SB, et al. (2002) The Role of Prior Pubertal Development, Biochemical Markers ofTesticular Maturation and Genetics in Elucidating the Phenotypic Herterogeneity of Idiopathichypogonadotrophic hypogonadism. Journal of Clinical Endocrinology & Metabolism 87: 152-160.
-
Hoffman AR, Crowley WF (1982) Induction of Puberty in Men by Long-Term Pulsatlle Administration of Low Dose Gonadotropin Releasing Hormone. The New England Journal of Medicine 307: 1237-1241.
-
Mason P, Adams J, Morris DV, Tucker M, Price J, et al. (1984) Induction of ovulation with pulsatile luteinising hormone releasing hormone. Br Med J (Clin Res Ed) 288: 181-185.
-
Fourman LT, Fazeli PK (2015) Neuroendocrine causes of amenorrhea–an update. J Clin Endocrinol Metab 100: 812-824.
-
Silveira LF, Latronico AC (2013) Approach to the patient with hypogonadotropichypogonadism. J Clin Endocrinol Metab 98: 1781-1788.
-
Couzinet B, Young J, Brailly S, Le Bouc Y, Chanson P, et al. (1999) Functional hypothalamic amenorrhoea: a partial and reversible gonadotrophin deficiencyof nutritional origin. Clin Endocrinol (Oxf) 50: 229-235.
-
Pape J, Herbison AE, Leeners B (2021) Recovery of menses after functional hypothalamic amenorrhoea: if, when and why. Hum Reprod Update 27: 130-153.
-
Young J, Xu C, Papadakis GEA, James S, Maione L, et al. (2019) Clinical management of congenital hypogonadotropic hypogonadism. Endocr Rev 40: 669-710.
-
Everaere H, Simon V, Bachelot A, Leroy M, Decanter C, et al. (2025) Pulsatile gonadotropin-releasing hormone therapy: comparison of efficacy between functional hypothalamic amenorrhea and congenital hypogonadotropic hypogonadism.Fertil Steril 123: 270- 279.
-
Bianco SDC, Kaiser UB (2009) The genetic and molecular basis of idiopathic hypogonadotropichypogonadism. Nat Rev Endocrinol 5: 569-576.
-
Morris DV, Abdulwahid NA, Armar A, Jacobs HS (1987) The response of patients with organic hypothalamic- pituitary disease to pulsatile gonadotropinreleasing hormone therapy. Fertil Steril 47: 54-59.
-
Tranoulis A, Laios A, Pampanos A, Yannoukakos D, Loutradis D, et al. (2018) Efficacy and safety of pulsatile gonadotropin-releasing hormone therapy among patients with idiopathic and functional hypothalamic amenorrhea: asystematic review of the literature and a meta-analysis. Fertility and Sterility 109: 708-719.e8.
-
Kassi LA, Eaton JL (2025) Pulsatile gonadotropin- releasing hormone therapy: does one size fit all. Fertil Steril 123: 243-244.
-
Kochar Kaur K, Allahbadia GN, Singh M (2021) An update on the Advances in the management of Congenital hypogonadotrophic hypogonadism-A Minireveview. J Pediatrics and Child Health Issues 2(1).
-
Kochar Kaur K, Allahbadia GN, Singh M (2023) An update on factors that enhance the chances of Discrimination of Constitutional Delay of Growth and Puberty from Congenital Hypogonadotropic Hypogonadism: Emphasis on role of INSL3:A Short Communication. Accepted for Publication In J of Fertilization: in vitro.
-
Rohayem J, Alexander EC, Heger S, Nordenström A, Howard SR (2024) Mini-Puberty, Physiological and Disordered: Consequences, and Potential for Therapeutic Replacement. Endocrine Reviews 45: 460-492.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- Clinical Study to Determine the Effectiveness of Pulsatilla Nigricans in the Management of Hypothyroidism with PCOD