Rare Complication of Hyperemesis Gravidarum-Central Pontine Myelinolysis, A Case Report
Hyperemesis gravidarum can sometimes be complicated with potentially life threatening complications, one of which is central pontine myelinolysis. Here we present a case of 23-year-old women who presented with hyperemesis with prolonged and severe hyponatraemia who subsequently developed spastic quadriparesis, diagnosed to be due to central pontine myelinolysis. She recovered on supportive measures and delivered at term uneventfully.
Background
Hyperemesis gravidarum is a severe form of nausea and vomiting in pregnancy and characterized by intractable vomiting, dehydration, electrolyte and acid- base imbalance and more than 5% loss of pre-pregnancy body weight. It occurs in 0.3 to 2% of women who are pregnant [1]. Although it is self-limiting majority of times, rarely severe electrolyte and vitamin imbalance results in complications such as Wernicke’s encephalopathy, central pontine myelinolysis, vasospasm of cerebral arteries, rhabdomyolysis, coagulopathy and peripheral neuropathy [2]. Central pontine myelinolysis (CPM), also known as osmotic demyelination syndrome, is a demyelinating disorder of the central pons, while preserving the axons. Myelinolysis can occur in extra-pontine sites as well. It is often associated with osmotic stress [3]. During pregnancy, CPM is most commonly seen in patients with hyperemesis gravidarum, in whom there is rapid fluctuation in blood osmolality due to hyponatraemia and its rapid correction. Pregnancy related CPM can also be seen associated with salt restricted diet [4], lithium toxicity [5], treatment with parenteral magnesium sulfate [6], gestational diabetes with hyperosmolar crisis [7]. Few risk factors have been identified for the development of CPM, with the most important being the concentration of serum sodium at presentation, the duration of hyponatraemia and speed of correction of chronic hyponatraemia [8, 9]. Here we report a case of hyperemesis gravidarum who presented with prolonged duration of hyponatraemia, who developed features of central pontine myelinolysis following correction of electrolyte imbalance. She was managed conservatively and recovered without any neurological deficits and delivered at term.
Case Report
A 23-year-old women presented at 16 weeks of gestation to the emergency department with complaints of excessive vomiting for 3 months, giddiness and yellowish discoloration of urine in the past 1 week and weight loss of 7kg in a week. She had been given primary care in a peripheral health center for the past 4 days and referred to our center for further management. On preliminary examination, she was found to be pale, afebrile, dehydrated with sunken eyes, with pulse rate of 116 bpm and blood pressure of 130/70 mmHg. Cardiovascular and respiratory system examination revealed normal findings. Uterine height corresponded to 16 weeks of gestation. There were no abnormal neurological findings at admission. Urine analysis for ketone bodies was negative. Her blood investigations revealed electrolyte imbalance [serum sodium- 120 mEq/L, serum potassium- 2.3 mEq/L] and deranged renal parameters [blood urea- 90 mg/dl, serum creatinine – 2 mg/dl] and liver function test [total bilirubin – 3.8 mg/dl, direct bilirubin-1.3 mg/dl, AST-226 IU/L, ALT-454 IU/L]. She was kept nil per oral, rehydration started with intravenous (IV) 0.9% sodium chloride (NaCl), ringers lactate (RL) and 5% dextrose solution alternatively at 125ml/hr. Potassium correction was initiated at rate of 10mEq/hr. Antiemetic Ondansetron 4mg was given IV every 8th hourly. Fifteen hours after admission patient developed altered sensorium and irrelevant talk. Repeat blood investigations showed persistent hyponatraemia (sodium-120mEq/L), hypokalemia (potassium-2.5 mEq/L) and hypochloremia (chloride-71 mEq/L). Serum magnesium and calcium were within normal limits. Arterial blood gas analysis showed metabolic alkalosis. Diagnosis of delirium due to hyponatraemia was made and correction was started with hypertonic 3% NaCl at 25ml/hr. Potassium correction was continued and injection thiamine 100mg once daily was added to prevent Wernicke’s encephalopathy. Examination of fundus revealed no evidence of papilledema. MRI brain was found to be normal. TSH was found to be 11.34 mIU/L, started treatment with levothyroxine 100 micrograms once daily. There was no irrelevant speech after sodium correction, nevertheless patient remained drowsy for next 2 days, meanwhile her serum sodium increased to
129 mEq/L in 24 hours and 131 mEq/L in 48 hours and so did her potassium, which was 3 mEq/L after 48 hours. Patient maintained adequate urine output throughout. The next day patient’s consciousness improved and hypertonic saline correction was stopped and patient was on maintenance IV fluids. Her renal and hepatic function tests showed significant improvement. The next 4 days was uneventful and patient was continued on same treatment and was stable. A day later she developed carpopedal spasm and was found to have hypocalcemia (serum calcium-6 mg/dl) and hypomagnesemia (serum magnesium-1mg/dl).Prompt correction was initiated with IV calcium gluconate (10% calcium gluconate, 20 ml over 20 mins every 8th hour) and magnesium (1gm/hr). Four days later, patient was having difficulty is walking and slurring of speech though serum electrolytes were fairly within normal limits. On examination patient’s consciousness was deteriorating and she was found to have spastic quadriparesis. On a repeat MRI, she was found to have features suggestive of osmotic demyelination changes in the brain stem/central pons, bilateral thalami, external capsule and basal ganglia (lentiform nucleus) (Figure 1). Diagnosis of central pontine myelinolysis due was made and patient shifted to Intensive Care Unit for 5 days. Patient gradually improved over these 5 days with conservative management and physiotherapy, and discharged. At discharge patient was conscious and had slowness of speech as the only neurological deficit. She was followed in antenatal OPD throughout her pregnancy and delivered at term without any neurological deficits.
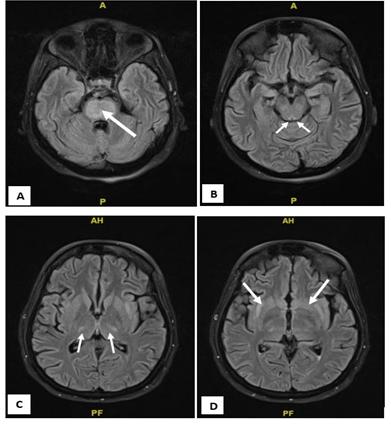
Figure 1: T2 heterogenous predominantly hyperintense area noted involving A. the central regions of pons. B. midbrain – tegmentum and tectum. C. Bilateral Thalami-Ventrolateral Regions and D. External Capsule with İnvolvement of Adjacent Lentiform Nucleus. There is evidence of diffusion restriction noted in these areas. No evidence of blooming in T2 sequences.
Discussion
The clinical presentation of central pontine myelinolysis varies widely based on the region of the brain involved. The classical presentation is of spastic quadriplegia and pseudobulbar paralysis which is attributed to the damage to corticospinal and corticobulbar pathways. These include para or quadriparesis, dysphagia, dysarthria, diplopia, loss of consciousness and other symptoms associated with brainstem damage [9]. The pathophysiology of myelinolysis is attributed to hyperosmotic stress produced by rapid correction of hyponatraemia, which causes endothelial injury and damages blood brain barrier resulting in release of myelinotoxic factors [9]. It is most commonly restricted to pontine neurons but can be observed in extra- pontine sites as seen in our case – thalamus, external capsule, midbrain, basal ganglia. Prolonged hyponatraemia and rapid correction predispose to CPM. In order to prevent it upper limits have been set for correction of hyponatraemia: 8 mEq/L in 24 hours, 14 mEq/l in 48 hours and 16 mEq/L in 72 hours [9]. Our case most likely already had prolonged hyponatraemia, which was uncorrected as she presented late to us with severe hyponatraemia (sodium 120 mEq/l). On correction,her serum sodium increased by 9 mEq/L in the first 24 hours and 11 mEq/L in 48 hours. As mentioned earlier CPM in pregnancy has been associated with parenteral administration of magnesium sulfate [6], and interestingly our patient too had parenteral magnesium sulfate for correction of hypomagnesemia before the onset of symptoms of CPM. The diagnosis of CPM is based on clinical history and symptoms and imaging tests. Cerebral magnetic resonance imaging (MRI) will show T1- weighted hypointense and T2- weighted hyperintense areas in the central pons and other extrapontine regions as described in our case. No optimal treatment is known for myelinolysis [3, 5]. Prognosis is uncertain and ranges from recovery after long periods of neurological deficits to death due to worsening of neurological damage [3]. The case we reported recovered spontaneously with supportive care and did not have any neurological sequelae and delivered at term without any complications.
Conclusion
Central pontine myelinolysis in pregnancy can cause both maternal mortality and morbidity in the form of severe neurological deficits. Hence it is imperative that fluid and electrolyte imbalance should be promptly detected early in the course of hyperemesis and care must be taken to avoid prolonged periods of hyponatraemia and avoid rapid correction of the same.
References
-
Goodwin TM (2008) Hyperemesis Gravidarum. Obstet Gynecol Clin North Am 35(3): 401-417.
-
Verberg MFG, Gillott DJ, Al-Fardan N, Grudzinskas JG (2005) Hyperemesis gravidarum, a literature review. Hum Reprod 11(5): 527-539.
-
Sánchez-Ferrer ML, Prieto-Sánchez MT, Orozco- Fernández R, Machado-Linde F, Nieto-Diaz A (2016) Central pontine myelinolysis during pregnancy: Pathogenesis, diagnosis and management. J Obstet Gynaecol 6: 1-7.
-
Ioannidis P, Balamoutsos G, Karacostas D (2017) Salt- free diet and pregnancy-related central pontine myelinolysis: “To diet or not?” J Neurol 257(12): 2101-2102.
-
Bejot Y, Depierre P, Osseby G-V, Troisgros O, Moreau T, et al. (2008) Central pontine and extra-pontine myelinolysis: A complication of lithium toxicity in a pregnant woman. Clin Neurol Neurosurg 110(8): 852- 854.
-
Riggs JE, Hogg JP (2000) Central pontine myelinolysis: association with parenteral magnesium administration. Mil Med 165(6): 494-495.
-
Lee IW, Su MT, Kuo PL, Chang CM (2010) Gestational diabetes and central pontine myelinolysis with quadriplegia: a case report. J Matern-Fetal Neonatal Med Off 23(7): 728-731.
-
Fraser D (1988) Central pontine myelinolysis as a result of treatment of hyperemesis gravidarum. Case report. Br J Obstet Gynaecol 95(6): 621-623.
-
Uzkeser M, Akoz A, Ozdemir G, Emet M, Bayramoglu A (2012) Wide Central Pontine, Bulbar and Thalamic Myelinolysis with Sequela. Eurasian J Med 44(3): 179- 181.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’