Eliminating Andean Region Health Disparities via Human Papilloma Virus Vaccination Administration Programs Implementation
This study explores human papilloma virus (HPV) disease epidemiology, successful school-based and combined clinicand school-based HPV vaccination programs, and the applicability thereof to Andean low- and middle-income countries (LMIC). Only 17% of incident cervical cancer cases occur in the Latin American Countries (LAC) of the Caribbean, Central and South America. But, the LAC have a 38% cervical cancer mortality. School-based HPV vaccination programs in LMIC have achieved three-dose vaccination rates greater than 80%. School-based vaccination programs are cost effective, deserving expansion. Three-dose HPV vaccination in LMIC schools satisfy the World Health Organization vaccination program requirements. Sustainable HPV vaccination campaigns require media campaigns including Internet components for health care providers, parents, and students. Campaigns cosponsored by Ministries of Education, Health, and Finance will increase national HPV vaccination awareness, program acceptance, and school-based program use
Introduction
Bolivia, Chile, Colombia, Ecuador, and Peru are part of the Latin American Andean region of South America. Globally, human papilloma virus (HPV) is responsible for over 500,000 incident cases of cervical cancer (CC), 86,000 (17%) of which occur in the Latin American
Countries (LAC) of the Caribbean, Central and South America [1, 2]. This amounts to about 7.8 million female years of life lost (YLL), limiting women’s socioeconomic contribution as grandmothers, mothers, daughters, sisters, and wives [3]. CC is the most frequent female cancer in Bolivia, the second most frequent female cancer in Colombia, Ecuador, and Peru, and the third most frequent female cancer in Chile [4]. Globally, about 274,000 die from CC annually, representing the fourth cause of global female deaths, but 241,120 (88%) of CC deaths occur in low- and middle-income countries (LMIC) [3, 4, 5, 6, 7]. Both LAC and LMIC comprise the Andean region. Cervical cancer is attributed with at least 33,000 (12%) deaths in LAC [8, 9]. In 2002 Colombia had 5,500 incident CC cases and 2,045 deaths [10]. In Peru CC has an estimated annual mortality rate of 24.6 per 100,000 translating to 2,098 deaths annually [2, 11, 12, 13]. CC is the leading female cancer mortality cause in Bolivia, Colombia, Ecuador, and Peru [2, 10, 12]. Consistent with this, increased case-fatality associated with decreased national income has been demonstrated for CC [14]. Between 1987 and 2003, Chile achieved a 48% reduction in CC mortality following improved CC screening [15, 16]. The outcome, a CC mortality rate of 8.4 per 100,000 women represents 677 deaths, the second leading female cancer mortality cause, and 129 YLL per 100,000 women in 2003 [16]. Subsequently, the CC mortality rate dropped to 7.3 per 100,000, reducing CC to the sixth cause of female cancer mortality in Chile for 2003 to 2007 [4]. The heat-labile bivalent (HPV2), quadrivalent (HPV4) and nonavalent (HPV9) vaccinations provide prophylactic primary prevention against the 70-82% of CC due to high risk (HR) HPV-16 and -18 [8, 12, 17, 18]. Long-term efficacy of HPV4 was confirmed with 6.26 years follow-up in Colombia [19]. An additional 9-15% prevention of CC from HR HPV-31, - 33, -35, -45, -52, and -58 is provided by HPV9 [18]. Vaccination-based primary prevention of CC is the leading method for LAC and LMIC to forestall impending unaffordable long term health care associated costs [14]. Peru approved HPV4 in 2008, the same year that hepatitis B virus vaccination (HepBV; the only other vaccine for primary prevention of cancer) was incorporated into the Peruvian National Vaccine Schedule [2]. HepBV implementation in low- income countries can take 20 years [13]. It may be unrealistic to expect HPV vaccination program implementation completion in less than 20 years from HPV vaccination marketing (2006). Colombia began a 3-dose school-based HPV vaccination program for 9 year old and older girls in 2011 [4]. Conversely, Chile started a 2-dose school-based HPV vaccination program for 9 year old and older girls in 2014 [4]. In 2011 Peru began a 3-dose school-based HPV vaccination program for 10 year old girls [4]. Bolivia and Ecuador lack HPV vaccination programs [4]. HPV is etiological in anal, oropharyngeal, penile, vaginal, and vulvar cancers [5, 20]. HPV types 6 and 11 contribute to 4.3 cases of incompletely curable recurrent respiratory papillomatosis (RRP) per 100,000 children [21]. HPV4 administered post incidence of RRP may reduce frequency of subsequent bouts of RRP [21]. External genital warts (EGW) may have a prevalence of 1%, with a total lifetime risk of 10% [22]. HPV types 6 and 11 are responsible for 90% of EGW [5]. HPV4 and HPV9 protect against EGW and RPP [18, 21]. Treatment of recurrent EGW has significant human and financial costs in Central and South America [1]. Low HPV vaccination rates mean that the incidence of anal, cervical, oropharyngeal, penile, vaginal, and vulvar cancers, EGW, and RRP will not decline as rapidly as possible. The Ministers of Health of LAC agreed in 2006 to introduce the HPV vaccination [9]. Yet, the Chilean Working Group on HPV requested additional information prior to HPV vaccination implementation leading to cost-effectiveness studies of HPV in Chile, which are reviewed below [23]. Despite proven efficacy, calculated cost-effectiveness, and a measure of political will, nine years later the Andean region lacks universal HPV vaccination programs. Attitudes towards HPV, vaccine supply costs, and vaccination implementation needs contribute to low vaccination rates. Attitudinal determinants of HPV vaccination acceptability will be the topic of a separate paper. Acceptable vaccination cost may be linked to both personal and national income, referred to in terms of gross domestic product (GDP). Vaccination acceptability only leads to immunization if affordable vaccine is available. Early detection and treatment may cure CC [14]. Given that LAC and LMIC may only have sufficient resources for a CC screen and treat program or an HPV vaccination program, means of reducing HPV vaccination program cost will be identified. It will be shown that there are resources available to provide HPV vaccination in the Andean region. Two Peruvian concurrent screen and treat and HPV vaccination trials will be presented. The selected approach to introduction of HPV vaccination in a nation may predetermine successful attainment of adequate vaccination rates.
Methods
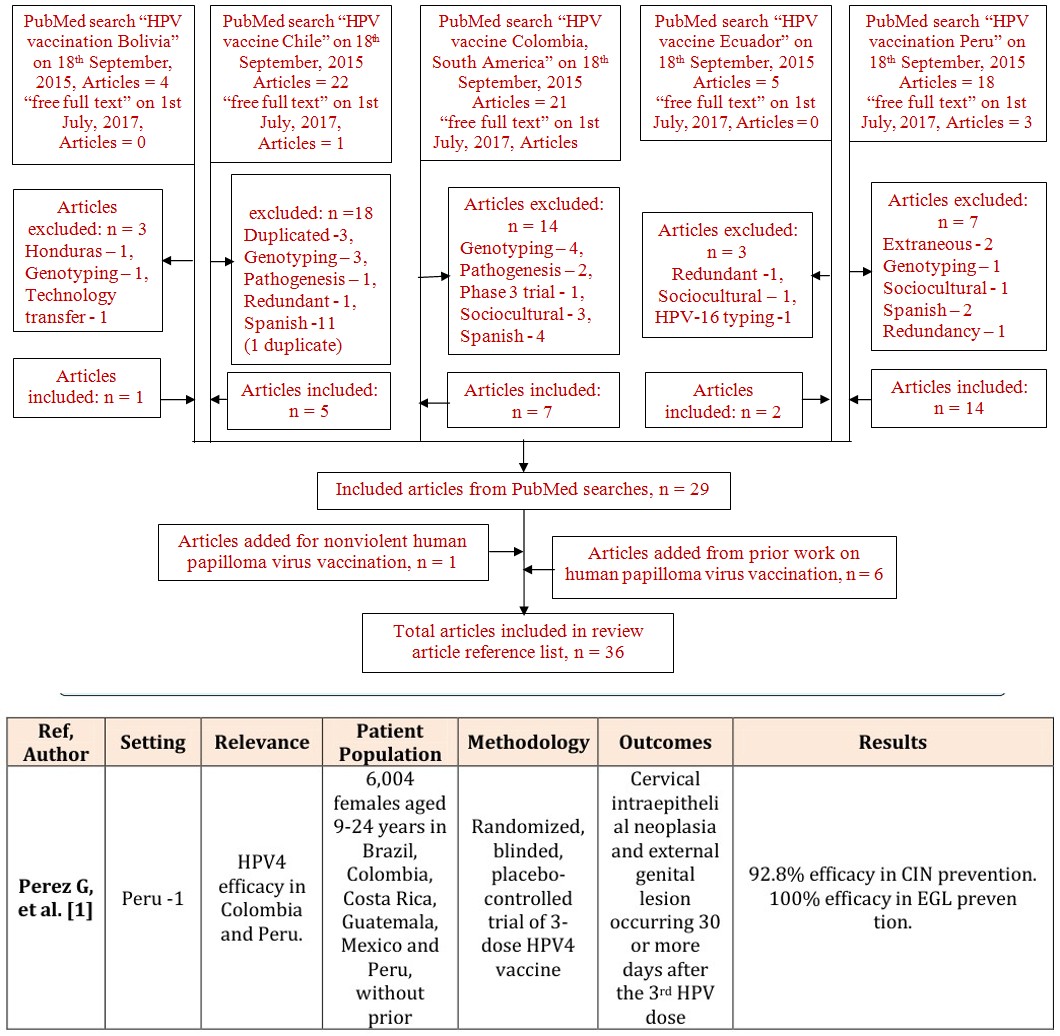
The PubMed database was searched using the terms “HPV vaccine” or “HPV vaccination” and Bolivia, Chile, Colombia, South America, Ecuador, or Peru as shown in Figure 1 yielding 58 English and 16 Spanish language articles. Articles were eliminated for duplication or redundancy, topic mismatch including sociocultural focus, repetitive phase 3 trials, repetitive discourse on the history of HPV-attributable disease and HPV vaccination. Spanish language articles were excluded, resulting in 29 included articles from the PubMed database searches. For coverage of the HPV9 vaccine, 1 article was added. For adequate background and discussion, 6 articles from the author’s prior research were added as shown in Figure 1 and Table 1.
abnormal Papanicolao
u tests, and with 4 or less sexual partners.
HPV awareness.
Purposive
319 FSW aged 18-29
sampling, Brown B,
HPV vaccine acceptabili
et al. [2] Peru -2
mixed- methods years in Lima, Peru
study.
ty.
Global HPV epidemiolo
Forman D,
Global men and women.
GLOBOCAN
et al. [3] Context -1
2008 data.
gy.
HPV prevalence
Soohoo M,
286 FSW in
Review
et al. [5] Peru -3
Lima, Peru
article.
in FSW.
Co- registering,
352 non- pregnant girls aged 10-13 years Interventio
Community
n ability to health worker led community- achieve 85% or higher 3- dose HPV vaccinatio Levinson non previously vaccinated against HPV, KL, et al.
Peru -4
[6]
based participatory and 323 research.
n rate.
non- pregnant women aged
30-45 years
30,900 girls aged 9-13 GAP provided free years in a mixed school and clinic-based
3-dose HPV vaccine per participant.
NGO-led
GAP supported vaccinatio n program.
Ladner J,
HP vaccine
NGOs covered cold-
et al. [7] Bolivia -1
program, and 3,480 girls aged 9- 13 years in a school-based chain, promotion and administratio HPV vaccine n.
program.
9.9% knew of HPV vaccine for CC prevention. 99% would accept 3-
HPV awareness. HPV vaccine acceptability
dose HPV vaccine. Average acceptable vaccine cost was US
$27.70. HPV knowledge was associated with having a STI within 1 year (p =.01), education, .
higher income, and not drinking alcohol before work (p =.033).
HPV-related
Adjusted female HPV prevalence
cancer and non-cancer with normal cervical cytology ranges from 1.7% in western Asia diseases to 35.4% in the Caribbean.
HPV prevalence ranged from
HPV prevalence
50.6-66.8%.
86% girls got 3-doses HPV
vaccine. 92% girls got 2-doses HPV
Subject participation
vaccine. 95% girls got 1-dose HPV vaccine.
, retention,
94% HPV+ women were treated.
and satisfaction.
90% HPV+ women had 6-month
follow-up. 96% participants were highly satisfied.
Program vaccination
The school-based program was
over subscribed with 3,739 participants (107%) receiving 3-
coverage based on census data.
doses HPV vaccine. The mixed school and clinic-based Vaccination
program achieved an 89% 3-dose adherence HPV vaccination rate. Both programs had a 96% vaccination (3-dose completion).
adherence rate
| Bartolini RM, et al. [8] | Peru -5 | Groundwo rk for HPV vaccine introductio n | Children, parents, community leaders, health and education officials, and policymaker s. | Mixed- methods formative research, including focus groups and in-depth interviews. | - | All respondents supported HPV vaccine introduction, cancer prevention. Community-level service safety and quality concerns exist. |
|---|---|---|---|---|---|---|
| Andrus JK, et al. [9] | Context -2 | Review of LAC HPV vaccine policy and delivery. | - | - | - | Use PAHO’s ProVac initiative for support. Provide HPV vaccine at US$5 or less, per dose. Use school-based vaccination programs. |
| Aponte- González J, et al. [10] | Columbia - 1 | CC epidemiolo gy in Colombia. Comparati ve cost- effectivene ss of 2vHPV and 4vHPV in Colombia. | CC incidence of 5,500. Annually, 2,045 CC deaths. 70% CC screening coverage. | Markov model simulation of cervical cancer and EGW natural history, CC screening, 2vHPV vaccination and screening, and 4vHPV vaccination and screening. | 2vHPV should cost US$ 17-47 to be very cost- effective or cost- effective. 4vHPV should cost US$19-49 to be very cost- effective or cost- effective. | Cost-effective HPV vaccine in Colombia should cost at most US$141-147 per vaccinated girl. Due to reduction of EGW, 4vHPV is more cost-effective than 2vHPV. |
| Lee FH, et al. [11] | Peru -6 | Brief educationa l interventio n effectivene ss. | 511 women aged 25-65 years inhabiting Puente Pidera, Los Olivos, and Comas, 3 low-income districts in Lima, Peru. | Convenience sampling, half from health centers, half from the market, pretest, posttest mixed methods survey with a 10-minute educational intervention | Knowledge of and attitudes towards HPV and CC. Knowledge that HPV vaccine prevents CC, and HPV vaccine acceptability . | 33% knowledge of HPV, CC, and HPV vaccine. 51% willingness to pay US$15 for HPV vaccination. 90% HPV vaccine acceptability. |
| Penny M, et al. [12] | Peru -7 | Identified facilitators of and barriers to HPV vaccinatio | 12 health facilities with affiliated schools and communities | Mixed- method, cross- sectional, purposive, case-study of | Feasibility of HPV vaccine addition to existing Peruvian Ministry of | 95% school-based HPV vaccination. 80% 1-dose or higher HPV vaccination rate. Unaffected routine vaccination schedules. |
n implement , health personnel, school-based HPV vaccination ation.
teachers, female 5th programs.
graders, aged 9 years or older, mothers, and civil authorities.
Parents of
Identificati
girls participating on of determina Purposive
sampling, qualitative study with Bartolini RM, et al.
in a 2008 Piura region school-based nts of parental acceptance Peru -8
[13]
in-depth interviews.
HPV vaccine demonstrati
of HPV vaccine.
on project.
National
(Mandatory Farmer P,
Colombia -
health insurance cancer treatment since 1994).
et al. [14]
2 program.
Model cohort was
123,581 girls aged 11 years, 58% CC screening Static Markov
Decision support for
onset at 25 years, 95% vaccination model simulation of CC screening possible Gomez JA, et al. [15] Chile -1 Chilean HPV vaccinatio n program.
coverage, with 2vHPV
80% prevalence or 4vHPV vaccination of HPV 16/18, EGW incidence of
4,685 Incidence
1,350. Annual mortality
(1997 Free radiotherapy
Suarez E,
Chile -2 Effect of CC
in PHI. 2001
Prieto M
677 representing in Chile.
Free chemotherap
[16]
129 YLL per
y in PHI).
100,000 women.
Health vaccine delivery.
PATH financial and technical support essential for program success.
Parental HPV vaccine
decision- Nonlinear HPV decision-making process changes with time from making conceptual HPV vaccine introduction. Prevention, cost, availability, and model. Differences credibility favor acceptance. Health system distrust favors in factors favoring HPV vaccine refusal.
acceptance and refusal.
(Vested interest in cost-effective cancer prevention to prevent potentially unaffordable national health insurance program outlays - - for cancer treatment).
Cost- effectiveness
2vHPV ICER was US$ 116 per QALY gained or US$ 147 per YLS.
of 2vHPV and 4vHPV, both costing
4vHPV ICER was US$ 541 per QALY gained or US$ 726 per YLS.
All are less than the PC-GDP US$
US$ 20 per
5th grade aged 9 years based simulation of or older in Goldie SJ, et al. [17] Peru -9 childhood the Ayacucho, Piura, and HPV vaccination and 3-5 lifetime adult Ucayali demonstrati HPV DNA screenings.
on project.
HPV genotype distributions
Compariso
n of simulated analyzed against HPV-
Posthoc analysis of 6
Riethmulle
r D, et al.
9vHPV
9vHPV efficacy to related diseases and multicenter retrospective trials [18]
4vHPV efficacy.
low-and high-efficacy studies.
9vHPV estimates
804 women aged 24-49 years in the early vaccination
6.26-year group, 703 women aged post- 4vHPV vaccinatio
29-50 years in the catch- Luna J, et al. [19]
Colombia -
3 n efficacy up vaccination in Colombia
group, and 103 women aged 29-50 years in the placebo group.
HPV contributio
80 Latin American VAIN and
Retrospectiv
e, cross- sectional study using Alemany L,
n to VAIN
et al. [20] Ecuador -1
and vaginal cancer.
191 American
hospital pathology vaginal Benefits,
Childhood HPV vaccination and 5
cost- effectiveness adult HPV DNA screenings may prevent 2/3 of CC deaths. Per dose HPV vaccine cost needs to be , and affordability $20 or less, for an ICER of $1,200/YLS, which is less than half Peru’s 2005 PC- GDP of US$ of HPV vaccination in Peru.
2,852.
9vHPV effect
9vHPV additional effect ranges from 9.9-15% for CC, 24.7-33.3%
on anogenital for CIN2-3, 12.3-22.7% for CIN1, 2.1-5.4% for EGW, 8.5-10.4% for and oropharynge anal cancer, 0-1.6% for oropharyngeal cancers. 9vHPV affords protection from almost al HPV- related disease in
90% of CIN, CC, EGW, and anal France
cancer.
At 6.26 years post-4vHPV vaccination no cases of HPV 6/11/16/18 – related CIN, EGW, - - or HPV 16/18-related CIN2 or worse occurred.
HPV DNA genotyping
Latin American VAIN samples had
a 93% HPV prevalence. American vaginal cancer samples had a 78%
via DNA Enzyme Immunoassa
HPV prevalence. HPV 31 has the greatest relative contribution cancer:VAIN ratio at 9.56, 95% y.
el Cáncer Hospital,
Quito, Ecuador from May 2012 to June
4vHPV efficacy trial, epidemiologi Velicer C, et al. [26]
Colombia -
8 prevalence providers,
7 academic .
and community c analysis.
health centers.
Estimated oncogenic
HPV prevalence
of 9.2% in Chile, 13.2%
HPV vaccine
in Peru, resulting in
Colantonio
Markov
cost- effectivene L, et al.
Chile -4
cohort model.
917 and 4,860 CC
[27]
ss in Peru and Chile.
cases respectively, and 532 and
3,155 CC
deaths respectively
8,092 5th grade girls in Piura region, who had participated Cross- sectional, 2- stage cluster LaMontagn HPV vaccine acceptabili e DS, et al.
in a PATH collaborated, school-based
Peru -10
sample design, using [28]
ty.
project, encompassin census districts.
g 264 schools and
161 health facilities.
PATH, et
al. [29] Peru -11 Peruvian
5th grade girls, aged 9 School-based
HPV
HPV
HPV prevalence.
HPV 16/18 prevalence - baseline
18.5% HPV 6/11 prevalence – baseline Serum and anogenital swabs at day
17% Risk factors for HPV infection –
1, months 7, prior Chlamydia or gonorrhea infection, 2 or more lifetime sex
12, 24, 36, and 48. Anogenital
partners, 1 or more new sex partners in the last 6 months, marital status other than first swabs at months 18, 30, and 42.
marriage.
Does universal
HPV vaccination
Vaccination plus current screening has an ICER per QALYs
cost less than twice the PC-GDP in Chile (3x US$26,594) and in Peru
gained ranges from US$ 4,576 in Peru to US$ 17,666 in Chile. As a middle-income nation Chile does not have access to the same funding array that Peru may have access to.
(3x US$
9,863).
82.6% HPV vaccination coverage
in Peru. HPV vaccine was accepted for CC
HPV vaccination
protection, disease prevention, and pro-vaccination belief. HPV refusal was programmatic, such as school absenteeism and lack of rates. HPV acceptance or refusal rationale.
make-up vaccination chances, or due to experimentation fears, allergies, and being advised against vaccination.
School- based HPV
>80% 3-dose HPV vaccination
rate. Multi-dose vaccination
vaccine pilot study.
years or older.
8,092 5th grade girls, aged 9 years or older, Piura region, Fiscal analysis of Mixed- methods involving 264 schools Peruvian fiscal analysis of school-based Levin CE, et al. [30] Peru -12 and 161 HPV vaccine pilot study health centers, from which 12 facilities HPV vaccination.
were selected for in-depth analysis.
Mothers and
daughters/ Communit y-based CC
grand- daughters, screen, treat, and vaccinate nieces, or Abuelo CE,
Prospective
et al. [31] Peru -13
female children of cohort program the community, aged 10-13
years.
HPV vaccinatio n program
Vicari A, et al. [32] Context -3
- - - planning.
Boys and girl
Non-blinded,
aged 11-15 randomized,
9vHPV years in Chile (n =
multicenter, comparative with routinely scheduled Schilling A,
et al. [33] Peru -14
100), Colombia (n
study with 1:1 gender pediatric = 140), and and intervention stratification vaccines Peru (n =
100).
vaccination. vaccination schedule requires co-ordination rate.
from education and health sectors. Health centers can be used for catch-up doses. Use consistent parental consent for all childhood vaccines.
US$ 3.88 per dose, for 82.6% 3- dose HPV vaccination rate. Project
Delivery cost school-
start-up and recurrent personnel based adolescent costs are largest portion of budget. HPV delivery cost can be HPV vaccination.
reduced if delivery is combined with existing health services.
Completion
of 3-doses HPV vaccine.
56% girls got 3-doses HPV
vaccine. 86% girls got 2-doses HPV
Treatment
of HPV+ women. 6-month follow-up of vaccine. 98% girls got 1-dose HPV vaccine.
81% HPV+ women were treated.
57% HPV+ women had 6-month
treated follow-up. 99.7% were highly satisfied HPV+ women CC incidence of 4,400, with 2,100 deaths annually in Peru. Plan vaccinate 287,000 girls aged 10 years annually.
Anti-HPV titers on day 1 and month
7. Antibody
titers for diphtheria, Equivalent antibody titers when 9vHPV was given with MCV4 and Tdap, or when 9vHPV was given 1 Neisseria meningitidis , pertussis, and tetanus month prior to MCV4 and Tdap.
on day 1, month 1, and month 7
for intervention,
- or month 1, month 2, and month 7 for controls.
- LAC vaccine program financing.
- Andrus JK, et al. [34] Context -4
- -
- -
- -
- Population, country, and
- LAC CC prevention simulation. region specific data.
- Individual-
- CC reduction,
- Goldie SJ, et al. [35] Context -5
- HPV 16/18 based stochastic
- GAVI eligible nations
- CC prevalence –
- ICER, YLS model in Bolivia
- 39%, in
- Chile 69%,
- Early global
- HPV vaccination
- Prevention
- Lowy DR,
- Schiller JT
- HPVrelated cancers.
- Review
- Context -6 programs’ theoretical article.
- -
- [36] and actual effectiveness
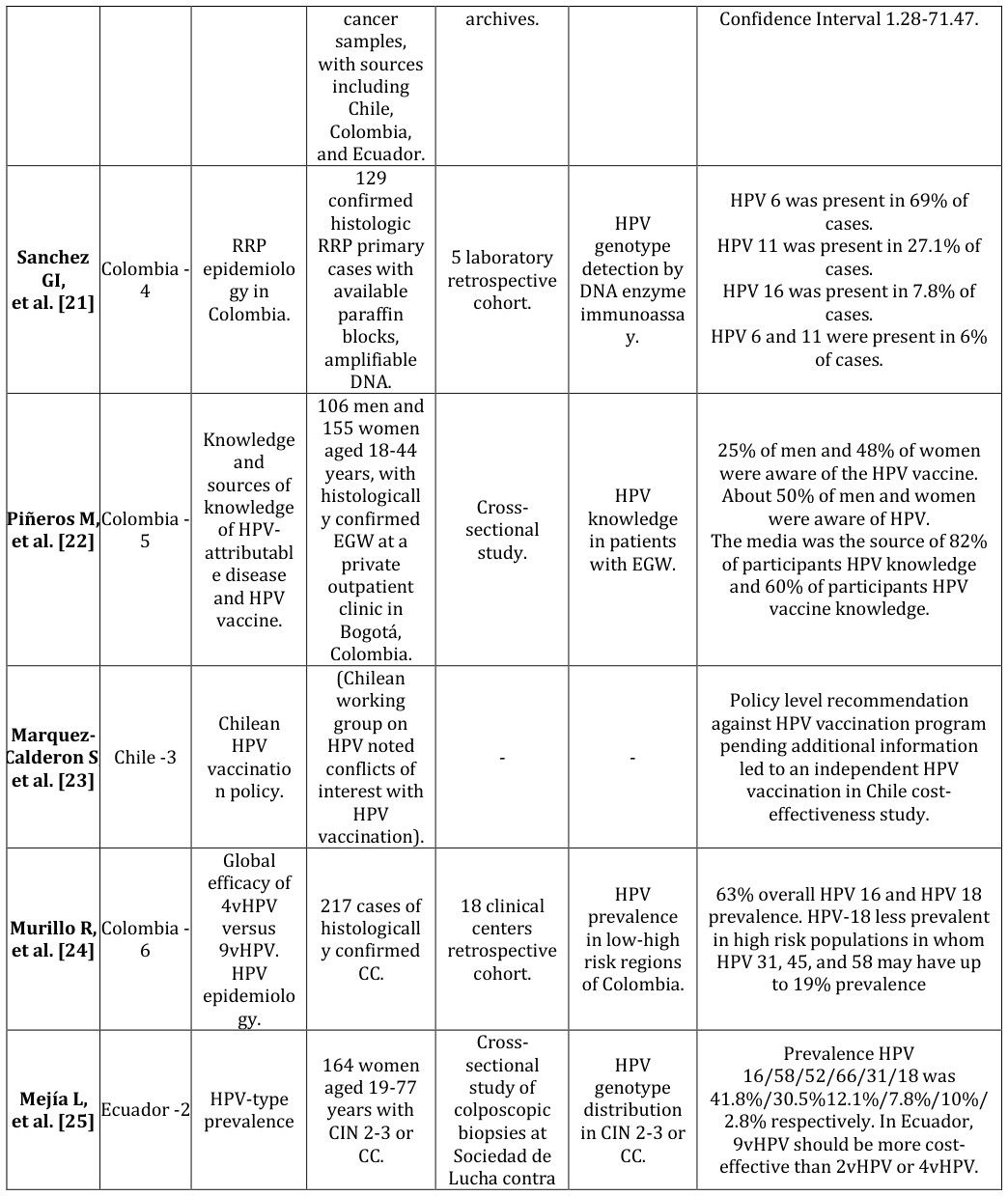
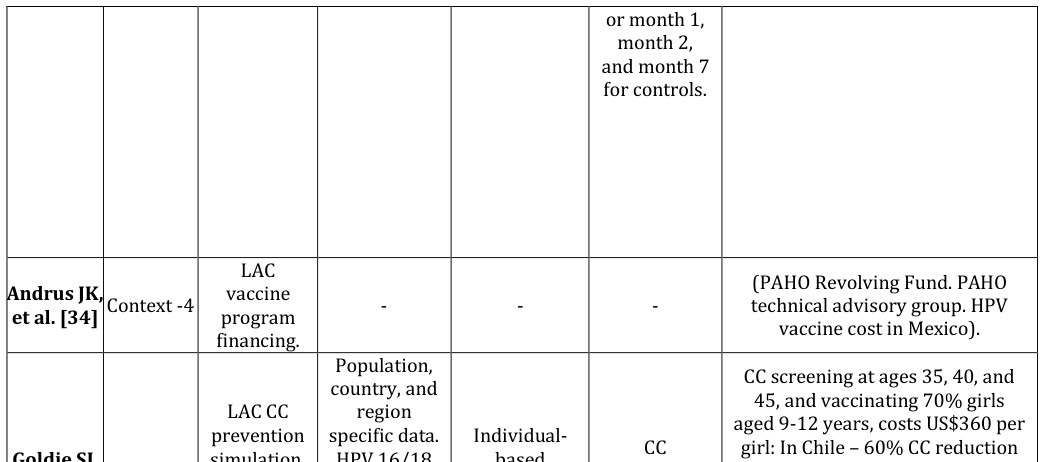
Table 2: Selected Articles on Human Papilloma Virus and Human Papilloma Virus Vaccination.
Cost-effectiveness of HPV Vaccination Programs in the Andean Region
Cost per vaccinated person, and vaccine efficacy for reduction of CC and EGW incidence are major determinants of HPV vaccine cost-effectiveness [24]. HPV2 or HPV4 administered pre-coitarche may reduce CC by 65% in Central and South America [24]. The Pan American Health Organization (PAHO) has led HPV cost-effectiveness analysis workshops for all LAC [9]. One of 5 blinded, placebo-controlled 3-dose international clinical trials of HPV4 included 725 female Colombians and 393 female Peruvians aged 9- 24-years-old who received HPV4 [1]. Placebo adjuvant aluminum vaccine was received by 637 female Colombians and 374 female Peruvians [1]. At 7 months post vaccination series, the per protocol efficacy population (PPE) achieved 92.8% efficacy against cervical intraepithelial neoplasia grade 1 (CIN1) or worse, 95.3% efficacy against cervical intraepithelial neoplasia grade 2 (CIN2) or worse, 92.5% efficacy against CIN3, and 100% efficacy against EGW [1]. Forty-three Colombians out of 6,004 total participants received HPV-16 monovalent vaccine. Pain, swelling, and erythema were the three most common adverse events [1, 9]. While HPV2 and HPV4 have similar efficacy for HPV-16 and -18 etiologic CC and CIN1-3, HPV2 has twice the effectiveness of HPV4 against other HPV- type etiologic CC and CIN1-3 [15]. As HPV-18 occurs in only 2.8% of female Ecuadorian HPV-positive specimens, and HPV-6, -11, 16 and -18 occur .52-.67 times less often in Colombia than in the United States, HPV2 with double the non-HPV-16 and -18
effectiveness, may be more cost-effective in Colombia and Ecuador than HPV4 [25, 26].
Mathematical Cost-Effectiveness Models
The Chilean National Health System Universal Access with Explicit Guarantees Plan (AUGE) ensures treatment of cervical cancer [27]. Using a $210 overall cost of HPV vaccination (or $70 per dose in 2006 U.S.$), which is less than the Chilean per capita GDP of $8,865, the undiscounted cost of HPV vaccination for one birth cohort of 12-years-old Chilean females would be $21 million. When applied to Peru, this model gives an undiscounted HPV vaccination cost for one birth cohort of $45 million [27]. In Chile, the projected incremental cost-utility ratio (ICUR)/incremental cost-effectiveness ratio (ICER) per quality-adjusted life years (QALY) for HPV2:HPV4 is 1:4.7 (116:541) and for life-years saved (LYS) 1:4.9 (147:726) [15]. Therefore, in Chile, HPV2 would be the economically expedient HPV vaccine choice for addition to the existing CC screening program [14]. However, in Colombia, where 37-61% of women age 18-25 years has annual CC screening, HPV4 is cost- effective at US$ 49 or less per dose, whereas HPV2 must cost $2 less [10]. Modeling with HPV9 may yield a different outcome given intentional coverage of five additional HPV types. Pre-coitarche HPV2 vaccination of 82% of Peruvian females would reduce the lifetime risk of cervical cancer by more than 50%, preventing 5,500 cases of cervical cancer, saving over 80,000 life years for one birth cohort [17]. At US$ 5 - 20 per dose, annual HPV vaccination would cost $5 million-$16 million, or from less than $300-$1,300 per year of life saved (YLS), which is less than the 2005 Peruvian per capita GDP of $2,852 in 2009 US$ [17].
School-based HPV Vaccination Programs
Two Bolivian non-governmental organizations (NGOs) successfully applied for donated HPV4 from the Gardasil Access Program (GAP) from 2009 to 2011 [7]. All other support for GAP approved programs comes from the applying nation [7]. The 2009 Bolivian program covered 57 schools, targeting 3,480 9- to 13- years-old females, but achieved 107.4% program coverage by prolonging the vaccination period by two weeks to include unintended school sites, vaccinating 3,739 females at a 96.1% three-dose vaccination rate [7]. The 2010 Bolivian program was both clinic- and school-based, with 258 sites, targeting 30,900 9- to 13- years-old females, achieving 89.3% program coverage, by vaccinating 27,597 females with a 96.2% three- dose vaccination rate [7]. For successful school-based vaccination programs GAP recommends advanced coordination and logistical support, and planned completion of vaccination within the academic year limiting loss to follow-up [7]. Mixed clinic- and school- based vaccination programs are better able to vaccinate persons absent from school on vaccination days, but require greater coordination and logistic support, and more cold chain capacity than do solely school-based vaccination programs [7]. Peru undertook a pilot study of HPV vaccination of fifth grade females 9-years or older with the Program for Appropriate Technology in Health (PATH) in 2007. PATH, working within World Health Organization (WHO) guidelines, selected school based outreach for the Expanded Program on Immunization (EPI) delivery of HPV vaccination in Peru. This was a donated HPV4 school-based vaccination program targeting 8,092 females attending 527 schools and 105 health centers in the Piura region of northwestern Peru in 2008 [12, 28]. Peru simultaneously promoted HepBV for 2- 11-years-old children, and upgraded the cold chain [12]. Cascade training of vaccination program staff included effective communication [12]. Regional planning meetings were held [12]. Radio stations, television, and the print media concurrently advertised each of the three doses of the HPV4 vaccination [13]. Program success depended on health system capacity comprising personnel, physical structures, cold chain, immunization supplies, training, and reporting, without negatively affecting existing vaccination programs [12]. In part due to single dose vial HPV packaging, cold chain capacity was to be increased by up to 103% in Ayacucho, 117% in Piura, and 167% Ucayali [8]. 82.6% of eligible females were vaccinated (95% CI 79.3-85.6), with 95% of vaccinations being school-based [12, 13, 28]. Support of educators accounted for 100% vaccination rates in some schools [29]. In other schools where educators were uninvolved vaccination rates could be as low as 50% [29]. As the consenting process for HPV was different than for HepBV some parents questioned the program legitimacy [29]. However, school-based outreach can cost more than twice health-center based or integrated outreach [30]. The lowest delivery cost per dose of HPV vaccine was $1.44 for Ugandan integrated outreach, contrasted with $3.88 for Peruvian school based outreach [30]. Integrated outreach costs are dependent upon existing program capacity especially for storage and transportation, and simultaneous introduction of other new vaccines [30]. PATH estimates that HPV vaccine introduction costs 5-13% of a national immunization budget, which may be greater than currently provisioned for EPI vaccines. Other program limitations are difficulties tracking receipt of all vaccination doses per person, training cost and time, logistics and expense of vaccination at isolated schools or in homes when doses were missed at school [12]. Following the success of this school- based program, in April 2011 HPV was included in the Peruvian national vaccination schedule [12, 28].
Health Center-Based HPV Vaccination Programs
The Peru CC prevention study (PERCAPS) intended for mothers and daughters, comprised of self-sampling for HPV, and treatment of HPV with cryotherapy for 30- to 45-years-old mothers accompanied by 10- to 14-years-old daughters who received three doses of HPV4 in Manchay (a shanty town outside Lima) and in the Iquitos region of Peru (Table 2) [6].
| Manchay [5] | Iquitos Region [21] | |
|---|---|---|
| 30- to 45-years old mothers, grandmothers, aunts | ||
| Recruited | 323 | 320 |
| Submitted HPV specimen | 312 | 320 |
| High risk HPV positive | 31 | 37 |
| High risk HPV negative | 281 | 283 |
| High risk HPV prevalence rate | 9.9% | 11.5% |
| Received cryotherapy | 29 | 28 |
| Received cervical biopsy | 0 | 2 |
| Adherent with 6-month follow-up | 26 | 16 |
| High risk HPV initial treatment rate | 93.5% | 81.1% |
| 10- to 14-years old female relatives | ||
| Recruited | 352 | 318 |
| Initiated HPV vaccination (trial- or school-based) | 332 | 309 |
| Received two doses of HPV (trial- or school-based) | 323 | 282 |
| Completed three doses of HPV (trial- or school-based) | 300 | 200 |
| Declined | 22 | 4 |
| Pregnant | 0 | 4 |
| Absent | ? | 22 |
| Inaccessible | ? | 14 |
| Not located | 4 | 32 |
| Moved outside area | 2 | 32 |
| Initiators’ 3-dose completion rate | 90.4% | 64.7% |
| Responding participant willingness to participate in a future study | 96.4% | 99.7% |
Table 3: Comparison of Peru cervical cancer screening study (PERCAPS) trials at Manchay, Peru and the Iquitos Table 2: Comparison
Data tabulated from text of [6, 22].
In Manchay trial PERCAPS achieved a 90.6% three dose HPV4 vaccination rate [6]. The second HPV4 dose arrived onsite one month late by which time some study subjects were lost to follow-up [6]. At completion 96.4% of PERCAPS subjects were willing to participate in another study [6]. School-based vaccination was suggested to reduce logistical loss to follow-up from cold chain and other supply issues including delayed vaccine delivery [6]. In the Iquitos region rural and urban trial of clinic-based HPV4 (and school-based HPV2) vaccination, a 64.7% three dose vaccination rate was achieved [31]. The lower completion rate was attributed to flooding of roads and bridges, impaired travel, delayed vaccine delivery, and loss of 64 subjects to follow-up [31].
Tools to improve HPV Vaccination Program Implementation
In Chile, Colombia, and Peru public health insurance can be a mechanism for HPV vaccination. Bolivia’s and Ecuador’s public health systems could consider HPV vaccination as part of system modernizations. Increased public awareness of HPV-associated diseases and the prevention thereof by HPV vaccination through health promotion advocacy programs can improve public reception of HPV vaccination programs [8]. HPV2 vaccination of 82% of one birth cohort of Peruvian females would reduce the lifetime risk of cervical cancer by more than 50%, preventing 5,500 cases of cervical cancer, saving about 2,625 lives [17]. In 2011 the Peruvian Ministry of Health planned to purchase HPV2 for the national vaccination program targeting sequential birth cohorts of 10-years-old females at one-quarter the market price via the PAHO Revolving Fund [32].
Means for Improving HPV Vaccination Rates
Immunization encounter reduction by simultaneous administration of HPV vaccine with either influenza vaccine or with tetanus, diphtheria, acellular pertussis vaccine (Tdap) and meningococcal vaccine (MCV4) eases the logistics of HPV vaccination program implementation while potentially increasing first and second dose HPV vaccine administration rates [33]. Co- administration of HPV9 vaccine, Tdap, and MCV4 achieves equivalent immunogenicity as separate vaccination schedules, with a statistically significant increase in injection site swelling, p = 0.007 [33]. None of the Andean region countries are currently eligible for support from the Global Alliance for Vaccines and Immunizations (GAVI), which works with the United Nations Children’s Fund (UNICEF), the WHO, the World Bank, and other organizations to assist in vaccination delivery in developing countries. The HPV4 vaccine is prequalified by the WHO and available to GAVI at $5 per dose [28]. This price is less than both the $34 per dose cost negotiated by Mexico, and the $120 per dose price in the USA [34]. At $5 per dose, translating to $25 per vaccinated person, HPV vaccination cost is equivalent to other vaccination series and is also less than per capita GDP for all LAC, making further cost-effectiveness redundant [34]. HPV vaccination is further subsidized by GAVI in the most economically disadvantaged nations [35, 36]. Boliva, a low-income country, was previously the only Andean nation qualified for GAVI new vaccine program introduction [9]. Chile is a middle-income country and would not normally qualify for GAVI, which supports the perceived need for Chilean cost-effectiveness studies prior to HPV vaccination program implementation [23, 27]. HPV vaccine is also available for $10-15 per dose via the PAHO Revolving Fund of the WHO established in 1977 for LMIC LAC [30, 34]. Due to PAHO Revolving Fund $40 million working capital LMIC LAC may prepay or reimburse PAHO within 60 days of receipt of vaccine [34]. Of note, PAHO adopted a Regional Strategy and Plan of Action for Cervical Cancer Prevention and Control, within the ProVac Initiative in 2008 [8]. ProVac allows for rapid start HPV vaccination programs [8]. Since 2004 ProVac has worked to improve LAC public health infrastructure, assure availability of appropriate data and analysis thereof for policy formation, promote new vaccination implementation programs, and foster partnerships for attainment of health care goals [9]. Peru has ordered 600,000 doses of HPV vaccine from PAHO [17]. The Peruvian immunization budget was increased by 500% from 2006 to 2010 for the 2011 launch of HPV vaccination [30].
Discussion
Comparative study of national vaccination programs or mathematical models thereof would be facilitated if identical types of data were published. For instance, some authors use discounted and undiscounted costs, total quality-adjusted life years, QALYs gained, and incremental cost-effectiveness ratio (ICER) per QALY gained, whereas other authors use cost per YLS or YLL [17, 27]. Given differing efficacy against non-HPV 16/18 genotypes, in Colombia and Ecuador, and other nations with comparatively low HPV 18 prevalence, HPV2 and HPV9 may be more cost-effective than HPV4 [15]. Given documented pregnancies at 10-years-old, it is recommended that national guidelines permit initiation of HPV vaccination at 9-years-old, which is consistent with manufacturers’ guidelines [31]. Many LAC and LMIC are in regions with drastic seasonal climate and other geophysical variables (earthquake, tornado, monsoon). To preclude interruption of vaccination programs by uncontrollable climate and geophysical variables, vaccination programs should be held in the most stable season. For instance, in Peru the goal should be to start annual vaccination drives simultaneously with the onset of the dry season. If all doses cannot be accommodated within one dry season, the plan should be to give the remaining dose(s) in the following year when the first dose is administered to the next birth cohort. Consideration of multidose vials may reduce demands on cold chain infrastructure. Reduction of HPV background prevalence could be approached in a similar manner to elimination of rubella [9] First, attain high vaccination rates for male and female birth cohorts at 9-years-old, primarily via school based vaccination programs [9] Second, vaccinate those 10- to 26-years-old who were not vaccinated as part of a birth cohort. Third, improve secondary prevention screen and treat programs for cervical cancer that will also serve as vaccination program effectiveness surveillance. Increasing HPV awareness via media campaigns and health care worker promotion emphasizing CC primary prevention, increasing the volume of trained community health workers (CHWs) and health leaders (HLs), coupled with increased cold chain capacity to preclude delays in vaccine delivery at administration sites form part of a health systems strengthening diagonal approach [14, 28]. This requires collaboration with national Ministries of Health who may also participate in the PAHO Directing Council of Ministers of Health [9]. Consistent nationwide use of school-based or integrated clinic- and school-based programs requires collaboration with national Ministries of Education [9]. Funding for the above may be more available if Ministers of Finance are also involved [9]. Consistent consenting processes for all adolescent vaccines will promote the legitimacy of vaccination programs in the community [28]. Consenting may begin in the prior academic year so that signed consents are available at the start of the vaccination academic year [28].
Conclusion
Consistent with scientific literature, varied HPV vaccination cost-effectiveness study methodology precludes direct study comparison. Moreover, increasing acceptance of more affordable 2-dose instead of costlier 3-dose HPV vaccination schedules reduces the direct applicability of much of the existing HPV vaccination cost- effectiveness studies. Nonetheless, irrespective of whether a 2- or 3-dose HPV vaccination program is chosen, the framework for vaccination program implementation remains constant: Program maintenance costs should be reduced. Vaccination program models and supportive international agencies are in place to assist national vaccination program implementation. Political will driving the necessary policy enactment and cooperation between Ministries of Education, Health, and Finance, are crucial for successful implementation and maintenance of Andean nation HPV vaccination programs.
Conflicts of Interest
Potential conflicts of interest. O. B. Nwanodi has ownership of less than $5,000 common stock outside of mutual funds in GlaxoSmithKline (Brentford, United Kingdom) and Merck (Kenilworth, United States).
Acknowledgment
This paper is based on coursework previously submitted to the College of Graduate Health Studies in partial fulfillment of the requirements for the Doctor of Health Sciences Degree, A. T. Still University.
References
-
Perez G, Lazcano-Ponce E, Hernandez-Avila M, García PJ, Muñoz N, et al. (2008) Safety, immunogenicity, and efficacy of quadrivalent human papillomavirus (types 6, 11, 16, 18) L1 virus-like-particle vaccine in Latin American women. Int J Cancer 122(6): 1311-1318.
-
Brown B, Carcamo C, Blas MM, Valderrama M, Halsey N (2010) Peruvian FSWs: understanding HPV and barriers to vaccination. Vaccine 28(49): 7743-7747.
-
Forman D, de Martel C, Lacey CJ, Soerjomataram I, Lortet-Tieulent J, et al. (2012) Global burden of human papillomavirus and related diseases. Vaccine 30(S5): F12-F23.
-
Murillo R, Herrero R, Sierra MS, Forman D (2016) Cervical cancer in Central and South America: Burden of disease and status of disease control. Cancer Epidemiology 44(S1): S121-S130.
-
Soohoo M, Blas M, Byraiah G, Carcamo C, Brown B (2013) Cervical HPV Infection in Female Sex Workers: A Global Perspective. Open AIDS J 7: 58-66.
-
Levinson KL, Abuelo C, Chyung E, Salmeron J, Belinson SE, et al. (2013) The Peru cervical cancer prevention study (PERCAPS): community-based participatory research in Manchay, Peru. Int J Gynecol Cancer 23(1): 141-147.
-
Ladner J, Besson MH, Hampshire R, Tapert L, Chirenje M, et al. (2012) Assessment of eight HPV vaccination programs implemented in lowest income countries. BMC Public Health 12: 370.
-
Bartolini RM, Drake JK, Creed-Kanashiro HM, Diaz- Otoya MM, Mosqueira-Lovón NR, et al. (2010) Formative research to shape HPV vaccine introduction strategies in Peru. Salud Publica Mex 52(3): 226-233.
-
Andrus JK, Lewis MJ, Goldie SJ, García PJ, Winkler JL, et al. (2008) Human papillomavirus vaccine policy and delivery in Latin America and the Caribbean. Vaccine 26(S11): L80-L87.
-
Aponte-González J, Fajardo-Bernal L, Diaz J, Eslava- Schmalbach J, Gamboa O, et al. (2013) Cost- effectiveness analysis of the bivalent and quadrivalent human papillomavirus vaccines from a societal perspective in Colombia. PLOS ONE 8(11): e80639.
-
Lee FH, Paz-Soldan VA, Carcamo C, García PJ (2010) Knowledge and attitudes of adult Peruvian women vis-a-vis Human Papillomavirus (HPV), cervical cancer, and the HPV vaccine. J Low Genit Tract Dis 14(2): 113-117.
-
Penny M, Bartolini R, Mosqueira NR, La Montagne DS, Mendoza MA, et al. (2011) Strategies to vaccinate against cancer of the cervix: feasibility of a school- based HPV vaccination program in Peru. Vaccine 29(31): 5022-5030.
-
Bartolini RM, Winkler JL, Penny ME, LaMontagne DS (2012) Parental acceptance of HPV vaccine in Peru: a decision framework. PLoS One 7(10): e48017.
-
Farmer P, Knaul FM, Shulman LN, Alleyne G, Armstrong L, et al. (2010) Expansion of cancer care and control in countries of low and middle income: a call to action. Lancet 376(9747): 1186-1193.
-
Gomez JA, Lepetic A, Demarteau N (2014) Health economic analysis of human papillomavirus vaccines in women of Chile: perspective of the health care payer using a Markov model. BMC Public Health 14: 1222.
-
Suarez E, Prieto M (2006) Cervical cancer: The Chilean perspective. Int J Gynaecol Obstet 95(S1): S235-S238.
-
Goldie SJ, Levin C, Mosqueira-Lovón NR, Ortendahl J, Kim J, et al. (2012) Health and economic impact of human papillomavirus 16 and 18 vaccination of preadolescent girls and cervical cancer screening of adult women in Peru. Rev Panam Salud Publica 32(6): 426-434.
-
Riethmuller D, Jacquard A-C, St. Guily JL, Aubin F, Carcopino X, et al. (2015) Potential impact of a nonavalent HPV vaccine on the occurrence of HPV- related diseases in France. BMC Public Health 15: 453.
-
Luna J, Plata M, Gonzalez M, Correa A, Maldonado I, et al. (2013) Long-term follow-up observation of the safety, immunogenicity, and effectiveness of gardasil in adult women. PLOS ONE 8(12): e83431.
-
Alemany L, Saunier M, Tinoco L, Quirós B, Alvarado- Cabrero I, et al. (2014) Large contribution of human papillomavirus in vaginal neoplastic lesions: A worldwide study in 597 samples. European Journal of Cancer 50(16): 2846-2854.
-
Sanchez GI, Jaramillo R, Cuello G, Quintero K, Baena A, et al. (2013) Human papillomavirus genotype detection in recurrent respiratory papillomatosis (RRP) in Colombia. Head Neck 35(2): 229-234.
-
Piñeros M, Hernández-Suárez G, Orjuela L, Vargas JC, Pérez G (2013) HPV knowledge and impact of genital warts on self esteem and sexual life in Colombian patients. BMC Public Health 13: 272.
-
Marquez-Calderon S, Lopez-Valcarcel BG, Segura A (2009) Medical societies' recommendations for immunization with human papillomavirus vaccine and disclosure of conflicts of interests. Preventive Medicine 48(5): 449-453.
-
Murillo R, Molano M, Martinez G, Mejia JC, Gamboa O (2009) HPV prevalence in Colombian women with cervical cancer: implications for vaccination in a developing country. Infect Dis Obstet Gynecol 2009: 653598.
-
Mejía L, Muñoz D, Trueba G, Tinoco L, Zapata S (2016) Prevalence of human papillomavirus types in cervical cancerous and precancerous lesions of Ecuadorian women. J Med Virol 88(1): 144-152.
-
Velicer C, Zhu X, Vuocolo S, Liaw K-L, Saah A (2009) Prevalence and incidence of HPV genital infection in women. Sexually Transmitted Diseases 36(11): 696- 703.
-
Colantonio L, Gomez JA, Demarteau N, Standaert B, Pichón-Rivière A, et al. (2009) Cost-effectiveness analysis of a cervical cancer vaccine in five Latin American countries. Vaccine 27(40): 5519-5529.
-
LaMontagne DS, Barge S, Le NT, Mugisha E, Penny ME, et al. (2011) Human papillomavirus vaccine delivery strategies that achieved high coverage in low- and middle-income countries. Bull World Health Organ 89(11): 821-830B.
-
PATH, Instituto de Investigación Nutricional, Ministerio de Salud de Peru, Estrategia Sanitaria Nacional de Inmunizaciones (ESNI) (2010) HPV Vaccination in Latin America Lessons learned from a pilot program in Peru. Seattle, WA: Program for Appropriate Technology in Health.
-
Levin CE, Van Minh H, Odaga J, Rout SS, Ngoc DN, et al. (2013) Delivery cost of human papilloma virus vaccination of young adolescent girls in Peru, Uganda and Vietnam. Bull World Health Organ 91(8): 585- 592.
-
Abuelo CE, Levinson KL, Salmeron J, Sologuren CV, Fernandez MJV, et al. (2014) The Peru Cervical Cancer Screening Study (PERCAPS): the design and implementation of a mother/daughter screen, treat, and vaccinate program in the Peruvian jungle. J Community Health 39(3): 409-415.
-
Vicari A (2011) Peru introduces nationwide HPV vaccination; Argentina announces HPV vaccine introduction. Global Immunization News 1.
-
Schilling A, Parra MM, Gutierrez M, Restrepo J, Ucros S, et al. (2015) Coadministration of a 9-valent human papillomavirus vaccine with meningococcal and Tdap vaccines. Pediatrics 136(3): e563-e572.
-
Andrus JK, de Quadros C, Matus CR, Luciani S, Hotez P (2009) New vaccines for developing countries: Will it be feast or famine? American Journal of Law & Medicine 35(2-3): 311-322.
-
Goldie SJ, Diaz M, Constenla D, Alvis N, Andrus JK, et al. (2008) Mathematical models of cervical cancer prevention in Latin America and the Caribbean. Vaccine 26(S11): L59-L72.
-
Lowy DR, Schiller JT (2012) Reducing HPV-associated cancer globally. Cancer Prevention Research 5(1): 18- 23.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’