Male Breast Cancer: A Disease not to be Forgotten (A Case Report of an Uncommon Histological Subtype with HER Overexpression)
Male breast cancer (MBC) is a very rare malignant neoplasm with an incidence rate of 0.1 to 1%. It is usually detected in men between 60 and 70 years of age. Due to its low incidence, few clinical trials are conducted and few data are available. Generally, the knowledge is extrapolated from the experience with female patients. Treatment and survival for men with breast cancer is similar to that of women with breast cancer stage per stage. We present the case of an 89 years old male patient, with a 9 months history of an invasive non specific mammary adenocarcinoma in the left nipple ulcerating the skin and showing positive hormone receptor and high proliferation index, associated with multiple lenticular group of axillary nodes and a retractile and spiculated latero tracheal opacity. Through a literature review, we analyzed various epidemiological, clinical, histopathological and therapeutic aspects of this rare entity.
Introduction
Male breast cancer (MBC) is a very rare malignant neoplasm with an incidence rate of 0.1 to 1% [1]. It was first described by Halsted in 1907 [2]. Men of any age may develop breast cancer, although it is usually detected in men between 60 and 70 years of age. Radiation exposure, high levels of estrogen, and a family history of breast cancer can increase a man’s risk of developing breast Male Breast Cancer: A Disease not to be Forgotten (A Case Report of an Uncommon Histological Subtype with HER Overexpression) cancer [3]. The general variation of MBC across the globe is similar to female breast cancer (FBC) with higher rates in North America and Europe and lower rates in Asia [4]. These cancers are biologically different from carcinomas of the female breast. However, little is known about its biological and histopathological features, epidemiology, causes, prognosis, ideal management and treatment. Generally, the knowledge is extrapolated from the experience with female patients or a relatively small number of studies in male, mainly case series [5]. Treatment and survival for men with breast cancer is similar to that of women with breast cancer stage per stage. The impression that male breast cancer has a worse prognosis may stem from the tendency toward diagnosis at a later stage [3]. We report here a case of invasive non specific mammary adenocarcinoma in a male breast with HER2 overexpresion.
Case Report
Patient and Observation
An 89-year-old male with no significant past medical history presented with 9 months history of erythematous scaly lesions in the left nipple which were painless and slightly pruritic, gradually increasing in size, bleeding in contact without other associated signs. As he complained of cough and intermittent dyspnea, he consulted first many pneumologists who performed a chest X-ray that objectified the presence of opacity, then realized 3 BK sputum to eliminate a pulmonary tuberculosis, as the treating physician had a suspicion of infective pathology responsible for his symptoms. Then, he referred him to our training to complement support. No history suggestive of breast cancer pathology was elicited. Clinical examination revealed an erythematous plaque of about 3 centimeters with ulcerated center, well limited with irregular contours, bleeding on contact, occupying the nipple areola complex of the left breast, fixed to the underlying structures, with no discharge seen from the nipple and no inflammatory signs around. Axillary examination showed multiple lenticular group of axillary nodes. His physical examination and other organ system evaluation were normal.
Anterior chest X-ray showed a retractile and spiculated latero tracheal opacity occupying the inner half of the left hemithorax associated with adjacent micronodular lesions. A diagnostic breast mammogram was very difficult to achieve because the left breast was very small. However, it showed an ulceration aspect at the left mammary gland next to the nipple, with no real visible circumscribed opacity. A diagnostic breast ultrasound revealed an irregular, hypoechoic and somewhat heterogeneous mass, in the left retro areal area, measuring approximately 2,8 × 2 cm, without abnormal lymph nodes in the left axilla.
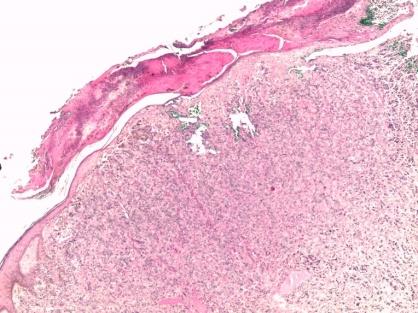
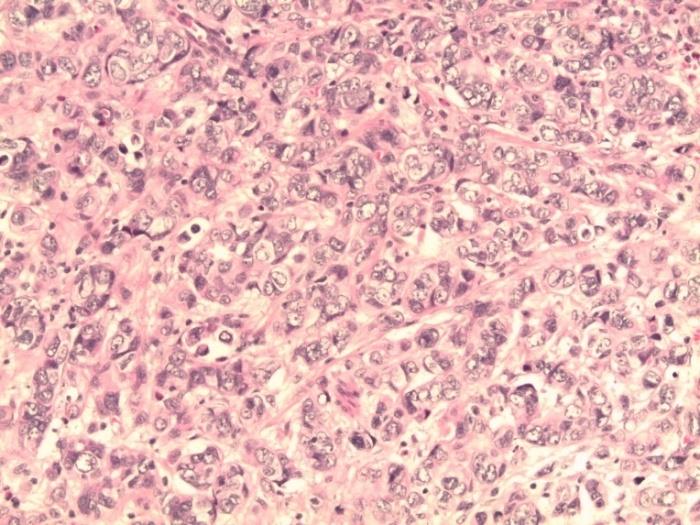
A skin biopsy was performed within the nipple ulceration. Microscopic examination showed a papillomatous epidermis with an ulceration covered with scabs and scales exposing an adenocarcinoma made of spans, leads and Compact Island with rare tubes, which infiltrated the entire thickness of the dermis and the hypodermis. The neoplasic cells were cuboid in shape and had an abundant acidophilic cytoplasm with hyperchromatic nucleoli showing a marked cytonuclear atypia (scored 3). The mitotic index was estimated at 28 mitosis per 10 fields (scored 3). The tumor developed in an abundant fibrous stroma studded with mononuclear inflammatory cells. Lymphatic vascular emboli and tumoral perineural sheathing were observed. The tumor infiltrated the arrecteur muscle of the nipple and infiltrated the epidermal coating. No intraductal cancerous component or normal mammary structures were observed.
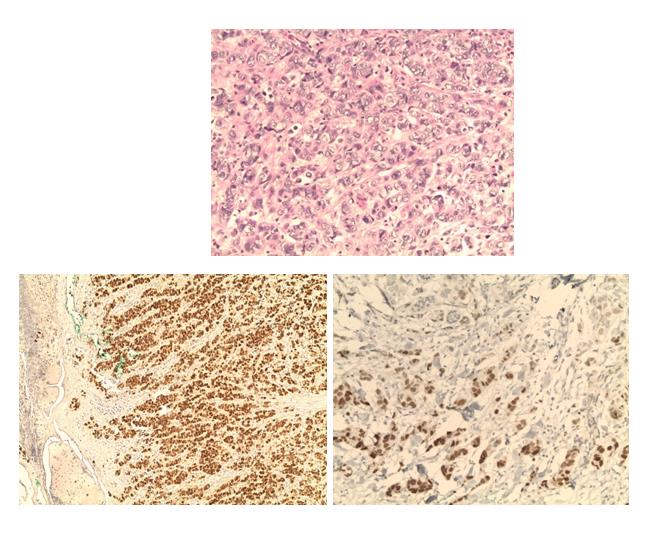
Immunohistochemistry studies showed the tumor cells to be strong and diffusely positive for RE, strongly positive for RP, Ki 67, with incomplete heterogeneous moderate to strong membrane staining for c-erbB2 /HER2. The cells were negative for CK7, CK20, TTF1 and NAPSIN A.
Based on the morphologic and immunohistochemistry findings, a final diagnosis of non specific mammary carcinoma, grade III of Ellis and Elston, ulcerating the skin with hormone positive receptors and high proliferation index was renered. The patient was subsequently referred to the oncology department for additional care.

Discussion
MBC most commonly targets men in the 6th and 7th decade of life [4]. The mean age at diagnosis varies among different studies between 62 and 71 years, which is about 5 to 10 years older than the average age at diagnosis for women [3]. Along with a higher age, men also present with more advanced disease [4]. This might be due to a lack of awareness of the early signs of MBC, which may lead to delayed screening and diagnosis [6]. Despite its rarity, analysis of the Surveillance, Epidemiology, and End
Results (SEER) registry identified an increasing incidence of male breast cancer over the past three decades [7].
The cause of MBC is unclear, however many risk factors were identified [2]. BRCA mutations, and specifically BRCA2 mutations, are a clear causal factor for male breast cancer [7]. However, these genetic mutations only account for a small proportion of MBC occurrence [4]. Men with a family history of breast cancer in a female or male relative have two to three times the risk of developing breast cancer themselves, and as in female breast cancer, the risk of male breast cancer increases with greater numbers of affected relatives [7]. Klinefelter’s syndrome has been associated with a 50-fold increase in risk of MBC [4]. Hormonal imbalance and increased estrogen levels can confer heightened risk for the development of male breast cancer. Specifically, obesity, liver disease, and testicular abnormalities may be linked to male breast cancer risk due to increased levels of circulating estrogen [7]. Physical inactivity, liver cirrhosis, hyperthyroidism, gallstones and diabetes have also been linked to an increased risk of MBC [4].
Most men with breast cancer present with a breast lump. Nipple discharge, ulceration, retraction and localized pain are some other common presenting features [4]. Male breast cancer is usually unilateral, and rarely involves both breasts [8]. Axillary lymphadenopathy was also a common finding in 40-55% of the patients [4]. Mammography and ultrasound are used as a diagnostic aid with the same criteria of malignancy in women [9].
Invasive ductal carcinoma is the predominant histological type of MBC. Papillary carcinoma is the second most frequent subtype in MBC. This is in contrast to invasive lobular carcinoma which is the second most common subtype in FBC. The occurrence of lobular carcinoma in MBC is still rare [4]. The poorly developed lobule formation and relative abundance of ducts in male breasts might explain the scarcity of lobular carcinoma and predominance of papillary patterns among in-situ carcinoma [8].
Hierarchical clustering analyses of gene expression profiles have classified female breast cancer into several intrinsic groups with different clinical outcomes. As high- cost microarray-based studies are not always feasible, immunohistochemical markers have been used as surrogates for classifying breast cancer [8].
MBC was more likely to be hormone-receptor positive (estrogen and progesterone) than female breast cancer [5]. Androgen receptor (AR) positivity is associated with favorable outcomes, especially in patients with Estrogen receptor (ER)-positive tumors. AR expression negatively correlates with expression of Ki-67, TP53 and with lack of expression of cytokeratine 5/6 and E-cadherin. These results are consistent with the fact that AR-positive tumors are well-differentiated, while AR-negative ones metastasize more frequently [1]. Rates of HER2 overexpression in male breast cancer have been variable in different cohorts, ranging from 2 to 45 % [7]. This is likely explained by the small study populations of each study as well as heterogeneity in the included stages and ethnicities and epidemiological differences [6].
Due to the low incidence of MBC, few clinical trials are conducted to assess the effectiveness of cancer treatments in this population. As a general rule, breast cancer in men should be treated similarly to postmenopausal hormone receptor-positive disease in women [5]. Surgery is the mainstay of treatment. RM has been replaced by MRM after retrospective studies suggested the equivalence of both procedures. Extensive chest involvement may be the only exception where RM is preferred. Neoadjuvant treatment depends upon hormonal status of the tumor and also on the inoperable nature of the tumor [4]. Adjuvant treatment of male breast cancer is same as in females’ stage per stage. Given the high prevalence of HR-positive disease, tamoxifen remains the gold standard of adjuvant hormonal therapies [3].
Axillary lymph node status and tumor stage are the two most important prognostic factors for MBC [4]. The symptoms of MBC are similar to those experiences by females with breast cancer following the menopause. However, the lack of awareness of MBC may delay the diagnosis and treatment, which is likely to result in the progression of the illness [2]. In addition, Some studies suggest that MBC has a worse outcome than female breast cancer, because of the small volume of breast tissue in men, which would permit cancer cells easy access to the lymphatic system and direct extension to the muscles and chest wall, and leads to high recurrence rates of cancer. Another explanation could be that MBC is initially diagnosed at a much later age, and that these patients are more likely to have a higher risk of cardiovascular and pulmonary comorbidities. Similarly, because of the advanced age, the use of radiotherapy is more limited in MBC patients compared with in FBC patients [6].
Conclusion
The current study described a rare case of invasive MBC with an uncommon histological form and positive AR. It actually highlights the need of public awareness concerning this disease to diagnose it at an earlier age, a lower stage and hence to improve survival rates.
References
-
Sas-Korczynska B, Adamczyk A, Niemiec J, Harazin- Lechowska A, Ambicka A (2015) Androgen receptor in male breast cancer. Pol J Pathol 66(4): 347-352.
-
Wang WW, Chen L, Ouyang XN (2014) Misdiagnosed male breast cancer with an unknown primary tumor: A case report. Oncology Letters 8(1): 190-192.
-
Aggarwal A, Liu ML, Krasnow SH (2014) Breast cancer in male veteran population: an analysis from VA cancer registry. JCSO 12(8): 293-297.
-
Jamy O, Rafiq A, Laghari A, Chawla T (2015) Male Breast Cancer: a 24 Year Experience of a Tertiary Care Hospital in Pakistan. Asian Pac J Cancer Prev 16(4): 1559-1563.
-
Thuler LCS, Bergmann A (2014) Male breast cancer: clinical-epidemiological characteristics of 1189 Brazilian patients. Aging Male 18(2): 118-123.
-
Hong JH, Ha KS, Jung YH, Won HS, An HJ, et al. (2016) Clinical Features of Male Breast Cancer: Experiences from Seven Institutions Over 20 Years. Cancer Res Treat 48(4): 1389-1398.
-
Ferzoco RM, Ruddy KJ (2016) The Epidemiology of Male Breast Cancer. Curr Oncol Rep 18(1): 1.
-
Zhou R, Yu L, Zhou S, Bi R, Shui R, et al. (2014) Male breast carcinoma: A clinicopathological and immunohistochemical characterization study. Int J Clin Exp Pathol 7(10): 6852-6861.
-
Oger AS, Boukerrou M, Cutuli B, Campion L, Rousseau E, et al. (2015) Male breast cancer: prognostic factors, diagnosis and treatment: a multi-institutional survey of 95 cases. Gynecol Obstet Fertil 43(4): 290-296.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’