Knowledge, Attitude and Practices of Family Planning in Antenatal Women in a Tertiary Care Hospital during COVID-19 Pandemic: Indian Perspective
Introduction: Family Planning is an essential element of the reproductive lifespan of a woman. It modifies and has an important impact on the life of a woman because it leads to increased morbidity and mortality following unwanted pregnancies, increased rates of abortions and further maternal complications. Hence awareness and a proper knowledge of the various available contraceptive choices to the women is important to modify the current scenario. Hence this study aims at studying the knowledge of Antenatal women, their attitude and practices being followed by them with respect to contraception. Methods: A self-administered questionnaire was given to the 100 Antenatal women attending the Outpatient Department of Obstetrics and Gynecology at Grant Government Hospital, Mumbai. Results: The results of this study depicted the importance of education, residential area and effect of COVID pandemic on the further reduction in the use of contraceptive measures available. The main reasons for low acceptance of contraception included Desire of early contraception in 24%, Lack of knowledge of contraceptive methods in 23% and apprehension for side effects of the contraception in 13% of the cases. Among the 15% of the women who were unaware of the available contraceptive methods, were willing to use the barrier contraceptives and IUCD and female sterilization. Conclusion: The results highlight the importance of social awareness and education and women employment in order to increase the use of contraceptive methods available.
Introduction
COVID 19, the global pandemic with its first case notified on December 31, 2019 from Wuhan, Hubei Province of the People’s Republic of China. It was declared as a Public Health
emergency of International Concern on January 30, 2020.
WHO declared it to be a pandemic on 11 March, 2020 thereby requiring a need of various social restrictions, withdrawal of various services with availability of only emergency services following the lockdown.
It is a novel viral disease, developed across the world. A rapid population growth is an encumbrance on resources available of many developing countries. Even though various choices of contraceptive methods are available, still there are higher rates of unwanted pregnancies and population explosion as a result.
In particular, documented disruptions to voluntary family planning and reproductive health care due to competing health priorities, service disruptions, stock outs and lockdowns are significantly impacting reproductive, maternal, newborn, and child health.
A recent World Health Organization (WHO) survey discovered that across 105 countries, 90% have experienced health service interruptions as a result of the pandemic. One of the most commonly disrupted areas includes family planning (FP) services, with 68% of countries reporting service disruptions [1]. In particular, women heightened direct and indirect risks of unintended pregnancy as a result of lockdowns, service disruptions, stock outs, and financial adversities [2, 3].
Family planning is a way of thinking and living that is accepted voluntarily upon the bases of knowledge, attitude, and responsible decisions by couples and individuals [4]. Family planning refers to a mindful effort by a couple to limit or space the number of children they have through the use of contraceptive methods [5].
Family planning deals with reproductive health of the mother, having adequate birth spacing, avoiding undesired pregnancies and abortions, preventing sexually transmitted diseases, and refining the quality of life of mother, fetus, and family as a whole [6].
A woman can get pregnant if one of man’s sperm reaches her egg (ovum). Contraception attempts to stop this either by stopping egg production or by keeping the egg and the sperm apart or by stopping the implantation of the fertilized egg into the uterus. Contraception in the meekest terms is the prevention of pregnancy and contraceptive methods, by definition, are the preventive methods to help women avoid unwanted pregnancies [7].
WHO has developed recommendations on which types of health workers can safely and effectively provide specific family planning methods? WHO based these recommendations on the evidence that a wide variety of providers can safely and effectively provide contraception? Specific competency-based training and sustained educational support help all types of healthcare providers do a better job at providing family planning [8]. In India, the spacing methods of contraception, viz. IUCDs (intrauterine contraceptive devices), OCPs (oral contraceptive pills), and Condoms are available at the public health facilities beginning from the subcenter level. Since OCPs, Condoms, and emergency contraceptive pills are not skill-based services, they are made obtainable through trained ASHAs (accredited social health activists) and FMPHWs (female multipurpose health workers). Permanent methods of contraception viz. vasectomy and tubal ligation are generally accessible at primary health center level or above. They are provided by MBBS doctors or gynecologists who have been trained to provide the services [9].
If healthcare workers do not have an apt knowledge and a favorable attitude to practice family planning, the acceptance level and compliance of family planning services by their beneficiaries from those healthcare workers will be compromised. For primary healthcare physicians to understand the strategy that would be required to promote family planning services they need to know the level of knowledge, attitude of their team workers, and thus having an idea about their practice, ultimately their counseling drive and intent of incentive to beneficiaries.
Materials and Methods
A self-administered questionnaire was served to the 100 antenatal women attending the outpatient department of Obstetrics and Gyanecology at Grant Government Hospital, Mumbai from January 2021 to February 2021 (two months) with the help of Health Care Person. This questionnaire was designed to explore KAPs about the available forms of Family planning methods. The data was analysed with dependant variables to be knowledge, attitude and practices of contraceptive methods and the independent variables being age, residency, religion, educational status, occupation, number of pregnancies and socio-economic status.
Results
Sociodemographic Characteristics of Participants
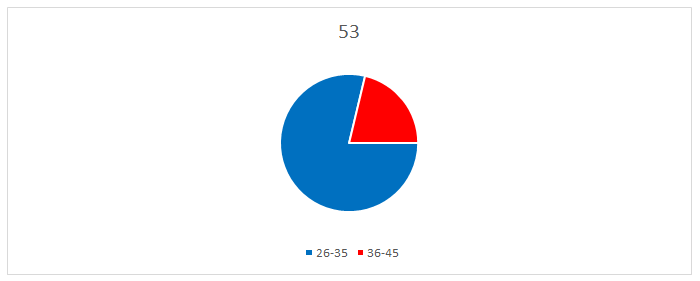
The age wise distribution of cases represented that 53% of the cases were in the age group of 18-25 years, 37% being in the age group of 26- 35 years and 10% of the cases were in the age group of 36-45 years.
| Age (in years) | No. of women | Percentage |
|---|---|---|
| 18-25 | 53 | 53 |
| 26-35 | 37 | 37 |
| 36-45 | 10 | 10 |
Table 2: Age distribution of cases.
The cases were majority Hindu by religion in 40% and Muslim by 60%.
| Religion | |
|---|---|
| Hindu | 40 |
| Muslim | 60 |
| Others (Christian, Buddhist) | 0 |
Table 3: Distribution of cases as per religion.
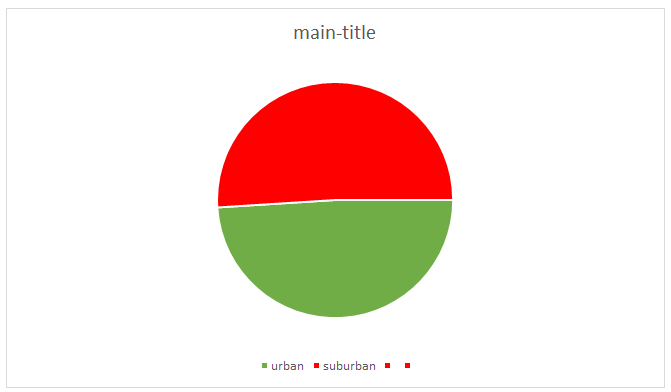
The cases from urban areas that were analyzed were 49% and from suburban were 51%.
| Residential area | No of cases | Percentage |
|---|---|---|
| urban | 49 | 49% |
| suburban | 51 | 51% |
| total | 100 | 100% |
Table 1: Distribution of cases as per residency.
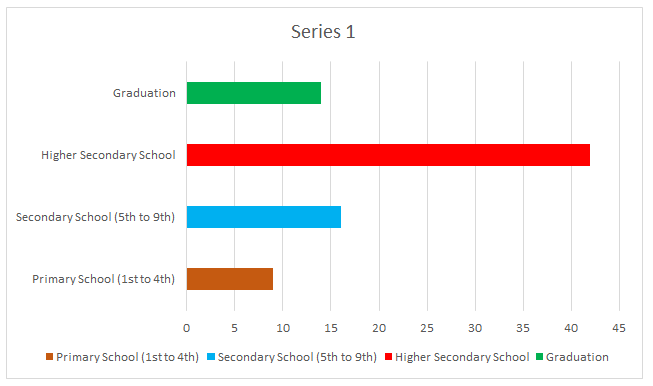
The case distribution analysed as per their educational status revealed that 19% were illiterate and 9% had education till Primary School and majority of the cases were educated till Higher Secondary School.
| Education | |
|---|---|
| Illiterate | 19 |
| Primary School (1st to 4th) | 9 |
| Secondary School (5th to 9th) | 16 |
| Higher Secondary School | 42 |
| Graduation | 14 |
| Post-Graduation | 0 |
Table 4: Distribution of case as per their educational status.
Among these cases, majority were housewives (80% ) followed by daily wage workers (10%) and women working in Private and Government employees being 8% and 2%.
| Occupation | |
|---|---|
| Government Employees | 2 |
| Private Sector | 8 |
| Daily wage workers | 10 |
| Housewives | 80 |
Table 6: Distribution of case as per occupation.
The cases that were analysed included 45% of the primipara women (first pregnancy), 36% being second gravida (with one living child), 14% being third garvida women
| Gravida | No of Cases | Percentage |
|---|---|---|
| Primigravida | 45 | 45% |
| Gravida 2 | 36 | 36% |
| Gravida 3 | 14 | 14% |
| Garvida >3 | 5 | 5% |
Table 8: Distribution of cases as per Gravida.
The knowledge about the contraception was majority assessed amongst the upper lower and lower class.
| Socio – economic status | % of cases |
|---|---|
| Upper class | 2 |
| Upper middle | 6 |
| Lower middle | 15 |
| Upper lower | 42 |
| Lower | 35 |
Table 9: Distribution of case as per their socio- economic status as per Modified Kuppuswami Scale.
Around 85% of the women had some knowledge and heard about contraception whereas about 15% were completely unaware regarding the contraception.
| Knowledge about contraception methods | |
|---|---|
| Known & heard about contraception | 85 |
| No knowledge about any form of contraception | 15 |
Table 10: Distribution of case as per their knowledge about the various contraceptive methods available.
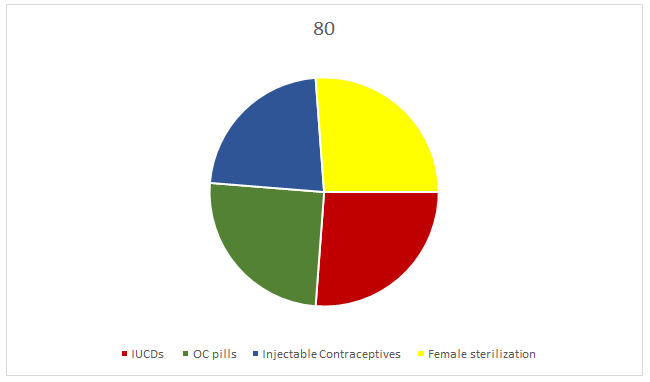
Amongst the women that had knowledge about the
- contraception, 80% knew about the barrier methods available, 72% had acquaintance with IUCD and female sterilization and least common awareness of the OC pills and injectables was seen.
- Knowledge about types of contraceptive methods
- Barrier (Condoms)
- 80
- IUCDs
- 72
- OC pills
- 69
- Injectable Contraceptives
- 62
- Female sterilization
- 72
- Male sterilization
- 43
Table 5: Distribution of case as per their knowledge about
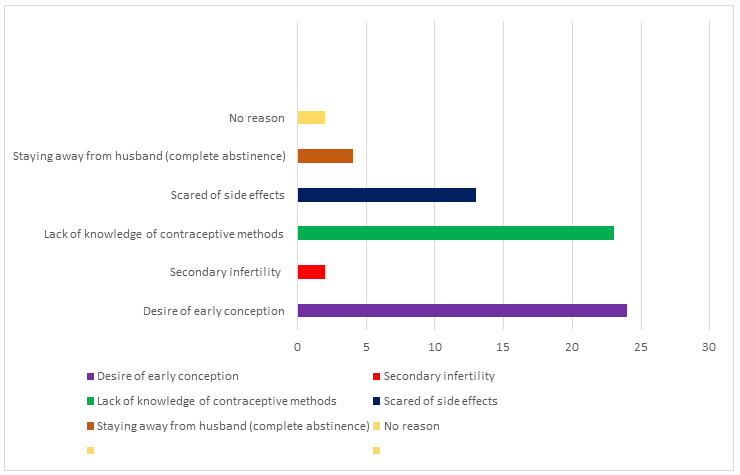
- The main reasons for low acceptance of contraception included Desire of early contraception in 24, Lack of knowledge of contraceptive methods in 23% and apprehension for side effects of the contraception in 13% of the cases.
- Reasons for low acceptance rate of contraceptive methods
- Desire of early conception
- 24
- Secondary infertility
- 2
- Lack of knowledge of contraceptive methods
- 23
- Scared of side effects
- 13
- Staying away from husband (complete abstinence)
- 4
- No reason
- 2
Table 7: Table depicting reasons for low acceptance of
- The contraception counselling is an essential key for controlling the menace of population explosion. This included spreading awareness regarding the various contraceptive methods available, their side effects and the false beliefs regarding their usage.
- Following counselling, the women were assessed regarding the acceptance by them about the various contraceptive methods available which showed that majority accepted barrier methods (34%), PPIUCD in 25%, female sterilization in 22% and 5% accepted the Injectable contraceptive methods
- Acceptance of a contraceptive method after counseling
- PPIUCCD
- 25
- TL
- 22
- Condoms
- 34
- Injectables
- 5
- Not decided
- 14
Table 11: Table showing acceptance of contraceptive
Discussion
Increasing program coverage and access of family planning will not be adequate unless all eligible women have satisfactory awareness or favorable attitude, and correctly and consistently practicing as per their need. Snowballing awareness/knowledge and favorable attitude for practicing family planning activities at all levels of eligible women are The Antenatal women were counselled regarding the use of contraceptive methods available, imparted the knowledge about the availability, benefits and side effects of the aforesaid methods, following which the women were ready to accept the methods. The women showed acceptance to barrier methods and female sterilization. The women were also counselled for the emerging new contraception and emergency contraceptives.
The awareness of MTP Act and impact of legalizing the abortion is increasing the society and the increasing number of service rendered through the government establishment underlines the increasing faith in the system. The chief reason of MTP is failure of contraception. This fact highlights the huge unmet need of contraception and counselling. The permanent method of contraception in the form of Tubal ligation is increasing as a choice of contraception after MTP. Still the religious differences are apparent in availing the MTP services and needs to be addressed tactfully [12].
These women were asked about their knowledge and awareness of contraception and pacing and their wishes regarding further childbearing. After ascertaining their wish, they were counseled regarding the various methods available (cafeteria approach), and the most suitable one for each one were individualised. Primiparas were counseled to rather insert an IUD or injectable contraceptives for birth spacing as it is not patient compliance dependent. Increased emphasis was laid on permanent methods of contraception (tubal ligation and vasectomy) for multiparous women (para 2 and above). Those multiparous women refusing sterilization operations were then counseled regarding the other temporary methods of contraception.
The demographic, socioeconomic, and educational/ professional background of the women and their partners were recorded. Parity and number of antenatal visits of these women, their knowledge/awareness of contraception, their responses to contraceptive counseling, and the reasons for refusal were also charted. A prepared data sheet that included all these information was used to analyze each woman’s data and response [13].
Women’s empowerment is a key factor in promoting contraceptive choice. This empowerment should not only be addressed at the education/employment level but more so at the family/community/religious levels. Involvement of community leaders is essential to overcome the hurdles. Efforts should also be directed at improving male education/ employment and, especially, male awareness [13]. The pandemic that lead to a major national lockdown with availability of only emergency services further limited the percentage of contraceptive methods available.
The National Family Planning Programmes have made available numerous contraception to the population and is encouraging more use of such contraceptive methods.
However still family planning is an important challenge with COVID 19 pandemic, because of the restrictions imposed by the administration.
Conclusion
The results highlight the importance of social awareness, women education and women empowerment in order to increase the use of contraceptive methods available. The use of emergency contraceptives should be encouraged so that the number of unplanned pregnancy thereby leading to increased rates of unsafe abortions can be controlled. Although there are various programs that highlight the importance of family planning, still COVID 19 pandemic with the major challenge of lockdown and restrictions imposed for the containment of the infection and hence the survival of current population is a dilemma situation. Hence the general population in addition to the counselling of the family planning methods, need education like wearing of masks, hand sanitization and social distancing to combat this difficult and challenging pandemic. In order to control one infectious pandemic, we cannot overlook the hidden pandemic of population explosion that waits to further impose threat in our future. A proper mitigation of family planning is of utmost demand, although restraining of COVID 19 pandemic is also important.
References
-
WHO (2020) Pulse survey on continuity of essential health services during the COVID-19 pandemic: Interim report. World Health Organization.
-
Hussein J (2020) COVID-19: what implications for sexual and reproductive health and rights globally?. Sex Reprod Health Matters 28(1): 1746065.
-
(2020) Impact of the COVID-19 Pandemic on Family Planning and Ending Gender-based Violence, Female Genital Mutilation and Child Marriage. United Nations Population Fund.
-
WHO (2007) Standards for Maternal and Neonatal Care. World Health Organization.
-
(2016) Ethiopia Demographic and Health Survey. Federal Democratic Republic of Ethiopia, Central Statistical Agency.
-
WHO (2020) Fact Sheets on Family Planning. World Health Organization.
-
Park K (2002) Park’s Textbook of Preventive and Social Medicine, 17th (Edn.), Banarasidas Bhanot, Jabalpur, pp: 325-358.
-
WHO (2018) Family Planning Global Handbook. World Health Organization.
-
Wani RT, Rashid I, Nabi SS, Dar H (2019) Knowledge, attitude, and practice of family planning services among healthcare workers in Kashmir–A cross-sectional study. J Family Med Prim Care 8(4): 1319-1325.
-
(2011) National guideline for family planning services in Ethiopia. Federal Democratic Republic of Ethiopia Ministry of Health.
-
Bekele D, Surur F, Nigatu B, Teklu A, Getinet T, et al. (2020) Knowledge and Attitude Towards Family Planning Among Women of Reproductive Age in Emerging Regions of Ethiopia. J Multidiscip Healthc 13: 1463-1474.
-
Katke RD, Prabhudesai AA (2016) Socio-epidemiological factors of medical termination of pregnancy: an overview in a tertiary care institute. Int J Reprod Contracept Obstet Gynecol 5(4): 1061-1064.
-
Kiran TU, Katke RD, Mane P, Pimple PG (2016) How empowered are women to choose contraception?. Int J Med Sci Public Health 5(10): 2019-2025.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’