Rare Vaginal Leiomyoma with Rare Microscopic Findings
Leiomyoma is the most common benign tumor of uterus and rarely may be seen in other parts female reproductive system like the round ligament, utero-sacral ligament, inguinal canal and vagina. Only a few examples of fibroid with vaginal origin have been documented in the literature. With only roughly 300 recorded occurrences, vaginal leiomyomas are still a rare condition. These vaginal fibroids arise most commonly from the anterior vaginal wall causing varied clinical presentations. We report a case of vaginal lateral wall fibroid of 8 cm size and extending into paraurethral space. The vaginal mass was surgically excised and histopathology confirmed the diagnosis of leiomyoma with cartilaginous degeneration.
Introduction
Mucus polyps, papillomas, hemangiomas, and leiomyomas are uncommon vaginal tumors. Since Denys de Leyden first identified a case in 1733, there have only been roughly 300 known cases of vaginal leiomyomas, making them a rare entity. The anterior vaginal wall is where these tumors most frequently develop, and they cause a variety of clinical manifestations. They might or might not be connected to leiomyomas in other parts of the body. We present the case of a 29-year-old multipara who was asymptomatic but brought an ultrasonographic report showing several uterine fibroids to the outpatient clinic.
Case Report
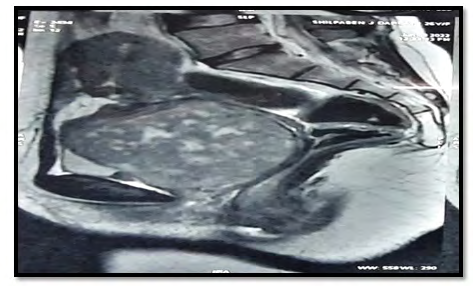
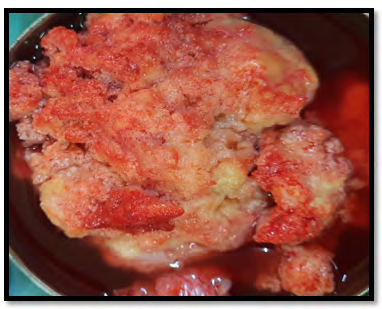
A 29 year-old para 2 live 2 woman with the history of previous two cesarean section history was referred to our outpatient department. She had a complaint of heavy irregular periods and dysmenorrhea for 36 months. She had a history of a mass which is separate from uterus and cervix in which lower border was inaccessible during her 2nd cesarean section .no other significant history otherwise. On examination, she was a medically fit and healthy woman. Abdominal examination was unremarkable and on speculum examination, a solitary mass of 6*6cms noted in the anterior right lateral vaginal wall, vaginal mucosa is stretched over the mass and no other changes noted. Cervix was not visualized on per speculum examination. Pelvic examination revealed normal sized uterus and solitary hard fixed mass of 8x 8 cms with regular margin and smooth surface arising from right lateral vaginal wall anteriorly. Diagnosis of vaginal fibroid made. Cervix was stretched behind the mass. An ultrasound scan showed a heterogenous mass of 8x 8 cms with poor vascularity and speckled calcification with normal looking uterus ovaries and endometrium. We proceeded further with MRI of pelvis, which showed to be a cervical fibroid. In suspicion with malignancy, punch biopsy of the mass was taken which resulted to be a benign mass. Her hemoglobin was 9.2 gram%. Cervical smears had always been normal. After discussion, the only option was surgery through combined vaginal and abdominal approach. At vaginal approach, catheterization done and incision was made on most dependent part away from urethra, fibrous capsule was opened and blunt dissection done and fibroid enucleated. A vaginal fibroid was confirmed. This had the macroscopic appearance and consistency of a degenerated fibroid and was later confirmed by histopathology to be a benign leiomyoma with cartilaginous changes with metaplasia and no signs of atypia. The patient made an uneventful recovery.
Discussion
Neoplasms of the vagina are infrequent and most are benign [1, 2]. A vaginal leiomyoma typically develops in the smooth muscle layer of the vaginal wall. It can arise from the smooth muscle of the rectum, bladder or urethra [3, 4]. Other reported sites of origin include smooth muscle of the vessel walls, mesothelial and embryonic rests. Clinical presentation of these tumors is varied depending upon the site. A posterior vaginal wall fibroid may cause difficulty with bowel or sexual function [5]. These tumors typically develop in the anterior vaginal wall’s midline and are tiny in size. There may be severe urine symptoms such frequent urination, urgency, dysuria, and urinary retention in such circumstances. However, in our case, the presence of the vaginal fibroid was obscured by her menstrual symptoms and the findings of cervical fibroid [6]. Our example demonstrates that vaginal fibroids exhibit typical pathogenic characteristics. The tumors are usually grey white in appearance, firm in consistency and well circumscribed. Microscopically, the tumor consists of a mixture of smooth muscle and a fibrous stroma and the finding were consistent with leiomyoma with cartilaginous metaplasia and secondary changes of hyalinization and calcification. Although, leiomyomas of the vagina are rare, sarcomatous changes can develop [6]. Leiomyosarcomas are seldom seen. Therefore, these should be removed if symptomatic or at the patient’s request to reduce the risk of cancer. It is important to perform a thorough bimanual and per speculum examination. The most effective way to get rid of these lesions is by enucleating the tumor through a vaginal incision, as was done in this instance (Figure 1-3).
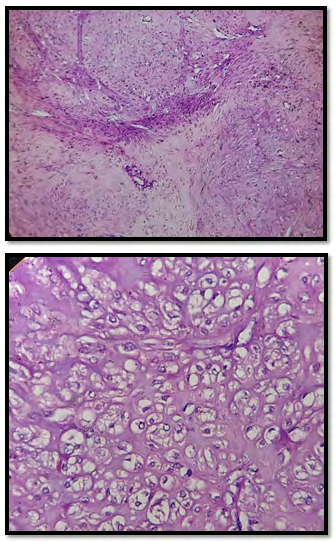
A literature review has been done regarding the subject of the case report “Vaginal Leiomyoma”. The literature review has been limited to a few case reports which have been published within 10 years (Table 1). We found that the most common age group is between 30 to 50 years, it has been also reported in women as 24 years old, and even in the 50 years old postmenopausal age group too. Also noted the clinical presentation was inconstant reliant on the location and size. The most common clinical presentation was found that mass coming out of vagina [7, 8, 9] and pain in the abdomen [8, 10]. In some of the cases also found urinary retention [11], vaginal bleeding [10], foul-smelling blood stained discharge from vagina [6]. Diagnosis is generally tough preoperatively by way of it can be a cervical fibroid but then again scientific and clinical USG and MRI can be used for the diagnosis, where the MRI reflects demarcated solid mass in the images, yet in one case the biopsy was done. Looking at the surgery part most of the management involves surgical vaginal enucleation. Vaginal leiomyoma is histologically consisting of spindle- shaped cells by means of slight or no mitotic activity but none of the literature reported a case of vaginal leiomyoma with histological findings with cartilaginous metaplasia with hyalinization [12, 13, 14, 15, 16, 17, 18, 19, 20].
| Author | Year | Age | Size | Location | Presentation | Diagnosis | Treatment | Reference |
|---|---|---|---|---|---|---|---|---|
| Gupta Mamta, et al. | 2017 | 44 | 6x5cm | Posterolateral vaginal wall | Pain in abdomen, Vaginal bleeding | MRI | Diagnosed as leiomyoma of cervix | [1] |
| He Liang, et al. | 2018 | 47 | 4cm | Bladder | Mass coming out | MRI | Bladder leiomyoma | [2] |
| Richa S, et al. | 2014 | 40 | 6cm | Anterior fornix | Mass coming out, Pain in abdomen | MRI, USG | Vaginal Leiomyoma | [3] |
| Nishat J, et al. | 2021 | 31 | 3x3cm | Anterior vaginal wall | Pain in abdomen | MRI, CLINICAL USG, | Laparoscopy with chromopertubation | [4] |
| Goyal LD, et al. | 2013 | 50 | 10x8cm | Posterolateral vaginal wall | Polymenorrhea, Pain in the abdomen | USG, MRI | Vaginal Myoma | [5] |
| Koranne PS, et al. | 2015 | 35 | 6x5cm | Bladder wall | Pain in abdomen | MRI | Bladder Vaginal Leiomyoma | [6] |
| Hsayaoui N, et al. | 2017 | 24 | 5x5cm | Under urethra | Foul-smelling blood stained discharge from vagina | CLINICAL USG, MRI | Vaginal fibroma | [7] |
| Behura J, et al. | 2020 | 40 | 6x5cm | Between the bladder base and the rectum | Mass coming out, Pain in abdomen | CT, MRI, USG | Vaginal Leiomyoma | [8] |
| Wu Y, et al. | 2015 | 44 | 3x4cm | Between the urinary meatus and the vaginal orifice | Mass coming out | MRI, USG | Vaginal Leiomyoma | [9] |
| Shah M, et al. | 2021 | 48 | 4x2x2cm | Right vaginal wall | Prolapsed vaginal mass | MRI, USG | Vaginal Leiomyoma | [10] |
| Egbe TO, et al. | 2020 | 36 | 13.14x14cm | Anterior vaginal wall | Mass coming out, pain in right iliac fossa | CLINICAL USG, MRI | Vaginal Leiomyoma | [11] |
| Kaba M, et al. | 2016 | 45 | 37x30mm | Away from the urethra and the bladder | Pain in abdomen, Vaginal bleeding | MRI, USG | Vaginal Leiomyoma | [12] |
| Liu Y, et al. | 2021 | 24 | 4cm | Anterior vaginal wall | Mass coming out, urinary retention | MRI, CLINICAL USG | Vaginal Leiomyoma | [13] |
Table 1: Literature review of Vaginal Leiomyoma (Literature published between the years 2013 to 2021).
Conclusion
A rare benign vaginal tumour called a vaginal paraurethral leiomyoma has a wide range of symptoms and a good prognosis. Recurrence and development into a malignant disease are uncommon. The gold standard for diagnosis is histopathological analysis, but MRI and USG can be used to pinpoint the tumor’s size and location. The majority of times, management calls for surgical vaginal excision; however, when it is large and situated high in the vagina, an abdominal approach may be explored.
References
-
Gupta M, Saini V, Jindal R, Kumari S, Nargotra N (2017) Vaginal Leiomyoma: Case Report and Literature Review. Journal of South Asian Federation of Menopause Societies 5(1): 62-65.
-
He L, Li S, Zheng C, Wang C (2018) Rare symptomatic bladder leiomyoma: case report and literature review. Journal of International Medical Research 46(4): 1678-1684.
-
Richa S, Yadav P, Kaur H (2014) Vaginal leiomyoma: a rare presentation. JSAFOG 62(2): 112-113.
-
Jahan N, Jahan S, Akter S, Chowdhury P, Mahmud KF, et al. (2021) Vaginal Leiomyoma, a Rare Variety in a Subfertile Women. Sch Int J Obstet Gynec 4(5): 187-190.
-
Goyal LD, Kaur H, Kaur K, Kaur S (2013) An unusual case of vaginal myoma presenting with postmenopausal bleeding. J Family Reprod Health 7(2): 103-104.
-
Koranne PS, Raut D, Wahane A, Uike P (2015) A rare case of anterior vaginal wall leiomyoma. J Obstet Gynaecol India 65(2): 129-131.
-
Hsayaoui N, Mbarki W, Bettaieb H, El Cadhi Y, Douik F, et al. (2017) Unusual Localization of a Leiomyoma; Vaginal Leiomyoma in a 24 Years Virgin Woman: A Case Report. Obstet Gynecol Cases Rev 4: 110.
-
Behura J, Poonam B, Anjali M (2020) Vaginal leiomyoma, post hysterectomy, mimicking vault prolapse: case report. International Journal of Reproduction, Contraception, Obstetrics and Gynecology 9(11): 4753- 4756.
-
Wu Y, Wang W, Sheng X, Kong L, Qi J (2015) A misdiagnosed vaginal leiomyoma: case report. Urology Case Reports 3(3): 82-83.
-
Shah M, Rachana S, Niranjan KC (2021) Vaginal Leiomyoma: A Case Report. JNMA 59(237): 504.
-
Egbe TO, Kobenge FM, Metogo JAM, Wankie EM, Tolefac PN, et al. (2020) Vaginal leiomyoma: medical imaging and diagnosis in a resource low tertiary hospital: case report. BMC Women’s Health 20(1): 12.
-
Kaba M, Boztosun A, Yazanel KA, Saglam M, Kivrak D, et al. (2016) A vaginal leiomyoma followed as a cystocele for a long time: a case report. J Cases Obstet Gynecol 3(2): 64-67.
-
Liu Y, Wang X, He Y (2021) GnRH analogue followed by surgery in treatment of vaginal leiomyoma-a case report. Medicine (Baltimore) 100(8): e24911.
-
Chakrabarti I, De A, Pati S (2011) Vaginal leiomyoma. J Midlife Health 2(1): 42-43.
-
Shimada K, Ohashi I, Shibuya H, Tanabe F, Akashi T (2002) MR imaging of an atypical vaginal leiomyoma. AJR Am J Roentgenol 178(3): 752-754.
-
Elsayes KM, Narra VR, Dillman JR, Velcheti V, Hameed O, et al. (2007) Vaginal Masses: Magnetic Resonance Imaging Features with Pathologic Correlation. Acta Radiol 48(8): 921-933.
-
Jordanov A, Strateva D, Hinkova N (2014) Vaginal leiomyoma: A case report and review of the literature. Akush Ginekol (Sofiia) 53(8): 33-35.
-
Shadbolt CL, Coakley FV, Qayyum A, Donat SM (2001) MRI of vaginal leiomyomas. J Comput Assist Tomogr 25(3): 355-357.
-
Costantini E, Cochetti G, Porena M (2008) Vaginal para- urethral myxoid leiomyoma: case report and review of the literature. Int Urogynecol J Pelvic Floor Dysfunct 19(8): 1183-1185.
-
Leron E, Stanton SL (2000) Vaginal leiomyoma—an imitator of prolapse. Int Urogynecol J Pelvic Floor Dysfunct 11(3): 196-198.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’