Benign Metastasizing Leiomyoma
Benign metastasizing leiomyoma is a rare condition usually seen in reproductive age women which presented with multiple benign smooth muscle tumors in extra uterine sites, which display unusual growth pattern. In this report, a case of benign metastasizing leiomyoma is discussed.
Walawe Nayaka S* and Karunarathna SMG
Postgraduate Institute of Medicine, University of Colombo, Srilanka *Corresponding author: Sanjaya Walawe Nayaka, Postgraduate Institute of Medicine, University of Colombo, 26/A, Sri Sumanasara Mawatha, Welegoda, Matara, Srilanka, Tel: 0094716422822, ORCID: https://orcid.org/0009-0008-1260-5046; Email: walawenayaka@gmail.com
Introduction
Benign metastasizing leiomyoma (BML) is a rare condition in reproductive age women which demonstrate nonmalignant metastatic phenomenon usually seen after uterine leiomyomas [1]. This displays unusual growth patterns with extra uterine benign-appearing smooth muscle tumors [2]. The mean age of the patient during the initial operation was 38.5 year old [3]. These extra uterine growths are more common in lungs, but sometimes seen in other sites as well such as deep pelvic cavity, retroperitoneal space, heart, inferior vena cava, retroperitoneal lymph nodes, muscular tissues of the limbs, skull and breast [4, 5, 6, 7, 8, 9, 10, 11]. Histologically BML is characterized by a benign history with low mitotic indices, absence of nuclear pleomorphism, and no evidence of invasion despite multiple distant lesions. They are associated with current or past history of uterine leiomyomata and conditions like diffuse peritoneal leiomyomatosis, intravenous leiomyomatosis, diffuse uterine leiomyomatosis. They are usually asymptomatic, but may have symptoms depending on the site of lesions [1]. Pathogenesis of BML is unclear, but theories used to explain the pathogenesis of endometriosis can be used to BML as well [12]. Immunohistochemistry studies found the presence of estrogen, progesterone and luteinizing hormone (LH) receptors in these tumors [13]. Exposure to high estrogen levels associate with BML while regression of BML was found, after pregnancy, menopause, oophorectomy, megestrol, aromatase-P450 inhibitors selective estrogen modulators and gonadotrophin releasing hormone (GnRH) agonists. But several cases of BML in post-menopausal women not on hormone replacement therapy (HRT), can’t be explained with hormone stimulus theory [14]. Most of the BML cases reported in last few years were reported following open or laparoscopic myomectomies and hysterectomies which highlighted the peritoneal seeding [15]. Coelomic metaplasia theory explains the transformation of subcoelomic mesenchymal cells into myofibroblast through the process of metaplasia under the influence of hormones. Lymphatic and vascular spread explains the presence of BML outside the peritoneal cavity due to the tumor cell embolization into the vessels and lymphatics [15].
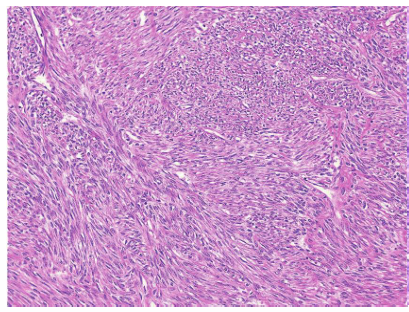
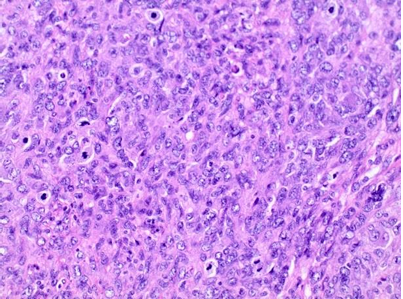
Imaging methods such as ultrasound scan (USS), contrast enhanced computerized tomography (CT) and magnetic resonance imaging (MRI) can be used to diagnose the conditions and assess the response to treatment. Histopathological studies shows show smooth- muscle cell proliferation with isolated mitoses, minimal atypical nuclei, and an absence of coagulative necrosis and pseudocyst formation. The nodules may contain fibroblasts, myofibroblasts, decidual cells, and sporadically, endometrial stromal cells [16].
Immunohistochemistry studies show vimentin, desmin, smooth muscle actin, and muscle- specific actin in the tumors and have a positive expression for estrogen, progesterone, and luteinizing hormone receptors [13].
There is no any standard treatment for the BML due to lack of cases in literature. But ovarian suppression with GnRH agonists, surgical excision or surgical castration have been used in the individual cases.
Even though BML is a benign condition, rarely it may become malignant [16].
Case History
A 36 year old unmarried nulliparous lady presented with 34 weeks size fibroid uterus for the myomectomy. Trans abdominal USS showed multiple uterine leiomyomas origin from the body of the uterus, even though a scan done 11 months ago was perfectly normal. Multiples leiomyomas (more than 30) removed through 3 uterine incisions during the myomectomy and 10 out of them were located within the broad ligament and retroperitoneal space without any connection with the uterus. Rest of the peritoneal cavity appears normal. She had uneventful recovery following surgery. Histology report confirmed the presence of multiple leiomyomas.
She was investigated for lower abdominal pain and right lower limb pain four months after the surgery and found to have soft tissue mass measuring 12cm deep in the pelvis, below the level of cervix which displace the uterus towards the left. MRI scan of the pelvis showed multi lobulated deep pelvic mass with extension into the retroperitoneum and right S1 neural foramen without typical MRI features of uterine fibroids. Plexiform neurofibroma, paraganglioma and leiomyosarcoma were the differential diagnoses suggested by radiologist.
Multi-disciplinary team meeting was arranged with the participation of a general surgeon and the patient and decide to proceed with exploratory laparotomy. She had multiple leiomyomas deep in the pelvis below the level of cervix and pelvic peritoneum which were extended towards the sacrum and retroperitoneal space. Surgery abounded due to the risk of uterine ischemia and hysterectomy following the removal of pelvic mass. Patient was thoroughly explained about the condition and available treatment options. She selected the total abdominal hysterectomy and bilateral salphingo oophorectomy (TAH+BSO) as she didn’t want to suffer anymore and not having fertility wishes. Patient agreed to accept all possible complications of selected treatment modality.
Her abdomen was re-opened two days after the initial surgery and TAH+BSO done with the removal of all deep pelvic and retroperitoneal fibroids. Bleeding continued from pelvic veins following the surgery and decided to pack the pelvis and close the abdomen temporary. Pelvic pack removal was done after 48 hours and routine midline closure done. She had uneventful recovery and histology re confirmed the presence of multiple leiomyomas and immunohistochemistry had not been done. She was started on estrogen only Hormone Replacement Therapy (HRT).
Discussion
Treatment of this patient with BML is very difficult as she was 36 year old and nulliparous. But the important fact is her leiomyomas grow very rapidly, because it took only 11 months to develop 34 weeks size fibroid uterus and 4 months to regrow the fibroids after initial surgery. Pathophysiology for the benign metastasis in this case could be Coelomic metaplasia or direct implantation of leiomyoma tissues after initial surgery. Haematogenous spread is still possible, but lung deposits have to be excluded as it is the commonest site. As she did not have any respiratory symptoms and her pre-operative chest X ray was normal, she was not offered a CT scan of the chest to exclude lung deposits. Performing a myomectomy at initial presentation was justifiable as she was unmarried and still 36 year old. But doing repeated surgeries to rapidly re growing leiomyomas is also a problem as it increases the surgical morbidity and mortality. Other possible treatment options which could have been tried were medical suppression of ovaries or MRI guided focused ultrasonography which could have preserve her uterus. But second option is not freely available in country and safety of using it in this kind of deeply seated retroperitoneal fibroids is not well established. Using uterine artery embolization can’t be justified as most of these fibroids didn’t have a direct communication with uterus. Usage of GnRH analogues can be justified for a short period. As she didn’t have fertility wishes in immediate future she may have to use it for more than six months which she need add back therapy to counteract the post-menopausal symptoms. Selection of surgical castration can be justified in patient’s point of view as she is suffering lot due to the disease and she needs complete recovery from the disease.
Removal of deeply seated pelvic leiomyoma may damage the major pelvic vessels, ureters, pelvic nerves, rectum and bladder. But the main problem was arrest the bleeding from pelvic veins which settled in this patient by pelvic packing. Bilateral internal iliac artery ligation can be done before attempting leiomyoma removal to minimize the bleeding.
Estrogen only HRT was started after surgery to prevent post-menopausal symptoms. But recurrence of the disease with estrogen only HRT is not well established and she need proper follow up to detect the recurrences. Mature oocyte cryopreservation or ovarian tissue cryopreservation could have been tried if the cost is affordable. But patient was not interested on that as she didn’t have fertility wishes in near future.
Conclusion
BML is a rare condition seen in reproductive age women which difficult to treat with surgical excision due to the recurrences under the influence of ovarian hormones. Age of the women, location of the fibroids, symptoms, and fertility wishes have to be considered when deciding the mode of treatment. Lack of evidence on different treatment options due to less prevalence of the disease is a major challenge.
References
-
Radswiki T, Bell D, Muzio BD (2022) Benign metastasizing leiomyoma. Reference article, Radiopaedia.org.
-
Rivera JA, Christopoulos S, Small D, Trifiro M (2004) Hormonal manipulation of benign metastasizing leiomyomas: report of two cases and review of the literature. J Clin Endocrinol Metab 89(7): 3183-3188.
-
Barnaś E, Książek M, Raś R, Skręt A, Skręt-Magierło J, et al. (2017) Benign metastasizing leiomyoma: A review of current literature in respect to the time and type of previous gynecological surgery. PLoS One 12(4): e0175875.
-
Rao AVC, Wilson J, Sylvester K (2008) Pulmonary benign metastasizing leiomyoma following hysterectomy: a clinicopathologic correlation. J Thorac Onco 3(6): 674- 676.
-
Taubert HD, Wissner SE, Haskins AL (1965) Leiomyomatosis peritonealis disseminata; an unusual complication of genital leiomyomata. Obstet Gynecol 25: 561-574.
-
Takemura G, Takatsu Y, Kaitani K, Ono M, Ando F, et al. (1996) Metastasizing uterine myoma: a case with cardiac and pulmonary metastasis. Path Res Pract 192(6): 622- 629.
-
Koh DM, Burn PR, King DM (2000) Benign metastasizing leiomyoma with intracaval leiomyomatosis. Br J Radiol 73(868): 435-437.
-
Abell MR, Littler ER (1975) Benign metastasizing uterine leiomyoma. Cancer 36(6): 2206-2213.
-
Horiuchi K, Yabe H, Mukai M, Morioka H, Udagawa Y, et al. (1998) Multiple smooth muscle tumors arising in deep soft tissue of lower limbs with uterine leiomyomas. Am J Surg Pathol 22(7): 897-901.
-
Alessi G, Lemmerling M, Vereecken L, Waele LD (2003) Benign metastasizing leiomyoma to skull base and spine: a report of two cases. Clin Neurol Neurosurg 105(3): 170- 174.
-
Jo JH, Lee JH, Kim DC, Kim SH, Kwon HC, et al. (2006) A case of benign metastasizing leiomyoma with multiple metastasis to the soft tissue, skeletal muscle, lung and breast. Korean J Intern Med 21(3): 199-201.
-
Kuo T, London SN, Dinh TV (1980) Endometriosis occurring in leiomyomatosis peritoneal is disserminata: ultrastructual study and histogenetic consideration. Am J Surg Pathol 4(2): 197-204
-
Danikas D, Goudas VT, Rao CV, Brief DK (2000) Luteinizing hormone receptor expression in leiomyomatosis peritonealis disseminata. Obstet Gynecol 95(6 Pt 2): 1009-1011.
-
Funakoshi Y, Sawabata N, Takeda S, Hayakawa M, Okumura Y, et al. (2004) Pulmonary benign metastasizing leiomyoma from the uterus in a postmenopausal women: report of a case. Surg Today 34(1): 55-57.
-
Al-Talib A, Tulandi T (2010) Pathophysiology and possible latrogenic cause of leiomyomatosis peritonealis disseminata. Gynecol Obstet Invest 69(4): 239-244.
-
Bekkers RL, Willemsen WN, Schijf CP, Massuger LF, Bulten J, et al. (1999) Leiomyomatosis peritonealis disseminata: does malignant transformation occur? A literature review. Gynecol Oncol 75(1): 158-163.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’