Challenges and Opportunities Confronting Factors of Partograph Utilization in Governmental Health Institutions of Addis Ababa, Ethiopia, 2022: Qualitative Study
The commencement of pregnancy requires close medical care. However, the inability of pregnant women to maintain optimal health result to pregnancy complications. This study sought to assess knowledge and associated factors on obstetric danger signs among pregnant women attending antenatal care at Tumu Government Hospital. A cross-sectional design adopted a simple random sampling technique to recruit 399 participants. A structured questionnaire was developed to collect data. Study data were analysed using Statistical Package Social Sciences (27) and analysed descriptively and inferentially with an alpha value <0.05 as significant. About 17% of participants had poor knowledge of obstetric danger signs. Factors such as occupation [p=0.001] associated with poor knowledge on obstetric danger signs. First trimester [p=0.012], Second trimester [p=0.001], Multigravida [p=.006] and Previous skilled birth [p=0.0001] significantly predicted poor knowledge on obstetric danger signs. About 17% Pregnant women had poor knowledge on obstetric danger signs. Awareness of pregnant women through more intensive health education programs would help avert the complications associated with obstetric signs. Further studies are recommended to examine the role of traditional practices in the emergence of obstetric danger signs among pregnant women in the community.
Introduction
Background of the Study
Partograph is a graphic record of progress of labor, maternal and fetal condition plotted against time for intrapartum monitoring. Its aim is to provide a pictorial overview of labor, to alert obstetric care providers about deviations in maternal, fetal condition and progress of labor/1/. It is a practical method when employed in a busy labor room with many cases, but limited personnel to screen for abnormal labor. With its use, there is no need to record labor events repeatedly. It helps predict deviation from normal progress of labor and supports timely and proven intervention. It also helps to show any deviation from the normal to the person conducting labor [1, 2].
Ethiopia is still one of those developing countries with an estimated maternal mortality ratio of 420/100,000 in 2013. World Health Organization recommends using the partograph to monitor labor and delivery, with the objective of improving health care and reducing maternal and fetal morbidity and mortality [1, 3]. Although the partograph is a simple and inexpensive tool that prevents maternal deaths and complications due to obstructed or prolonged labor, it is not as widely implemented as it should be. Caregivers may resist using the tool if they have insufficient knowledge and do not fully understand why they have been asked to use the tool. Non-availability of preprinted partograph has also been reported as a cause for non-utilization [3]. Filling the partograph is also seen as an additional task for a busy health worker in such a situation and may not be motivated to complete the partograph. However, the challenges to the implementation of the partograph, including insufficient knowledge, non-availability of preprinted partograph and workload pressure, can all be addressed with further education on the purpose of the partograph and local managerial support [3]. According to a study in African countries, the utilization of the partograph is poor despite preparing the tool that is simple and inexpensive for intrapartum monitoring of labor [4, 5]. Data across Africa have shown that, the partograph is not used at all or not used correctly despite that evidence that it is the best available tool for quality management of labor [6]. Studies done in Nigeria reported that only 25% to 33% of caregivers surveyed were using the partograph for routine monitoring of labor [3, 5]. The study of Tanzania also indicated that, only 74% of maternity clients were monitored by partograph [4]. Different studies in Ethiopia revealed low utilization of the partograph [7, 8].
The study conducted in north shoa zone shows that the utilization of partograph was 40.2% utilized partograph during labor [9]. Partograph was used only 13% of labors observed and 37% of facilities assessed referral and zone hospital where more likely than District hospital to use partograph for management of labor [10].
The study of public health facility in Addis Ababa showed that, 112(57.3%) of the obstetric caregivers utilized partograph to monitor labor. Compared to those working in hospital (34.4%) [11]. A recently published study conducted in Addis Ababa, Ethiopia also revealed trends in utilization of partograph. Is 69 % and non-utilization 31 % according to Nevertheless, working in public health centers than hospital had shown significant association with good knowledge of the partograph. The lack of preprinted partograph in the health institutions, being a general practitioner, poor knowledge and attitude towards partograph were the reason for not using partograph during labor; however, all these challenges to the use of the partograph can be resolved by provisions of pre-service and on the job training on partograph [6]. Generally, there are only few investigations on partograph utilization rate and contributing factors among healthcare professionals done in Ethiopia. And findings of the available studies also showed contradiction. Contrasting the rest of studies conducted in Ethiopia, some findings, for example study conducted by USID [10] presented that, more than half of the respondents utilize partograph. As well, WHO [11] revealed that, participants’ utilization of the partograph was in general good.
Sub-Saharan Africa had the highest maternal mortality ratio at 500 maternal deaths per 100,000 live births. According to a systematic analysis of progress towards Millennium Development Goal 5 more than 50% of all maternal deaths in 2008 were in only six countries (India, Nigeria, Pakistan, Afghanistan, Ethiopia, and the Democratic Republic of the Congo) [10].
Most of the maternal deaths around the world could have been prevented by improving women’s access to good- quality reproductive health care and effective interventions. Using of Partograph for labouring mother is one of the best interventions recommended by WHO to improve this quality of life of the mother and the foetus. It also decreases maternal and foetal mortality as well as morbidity. But it is poorly implemented in developing country [11].
Reasons for not using Partograph by obstetric care givers were the level of knowledge, exposure to training and socio- demographics like service year, age, sex and work places. It is expected that utilizing of Partograph significantly affects the quality of the delivery care system. Utilization of Partograph and documentation of the key events also poor as evidenced from 340 reviewed delivery records in Jimma hospital 274 (80.6%) files had Partograph attached. And utilized in only 19 (6.9%) of the records and some of foetal, labour and maternal parameters were correctly documented in 10.5% [7].
This may be due to that obstetric care givers may simply record after the labour process have been finished which is neither the mother’s nor the fetal’s life is saved. Thus, using the partograph needs align to the progress of the labour which is at the active first stage of labour and when the cervical dilation is 4cm. The next problem is that the overcrowded of the delivery unit and lack of adequate number of professionals which makes them too busy, thus the obstetric care givers are not properly monitor each labouring mother by using partograph. Even though the government and nongovernmental organization are tried to enforce the health professionals to use partograph in order to decrease maternal mortality it is not met the point as needed. The Millennium Development Goals (MDGs) also have focused renewed attention on infant and maternal mortality [12]. In the town a little information is available regarding different factors of partograph utilization. This study intends to answer whether the partograph that are used to monitor mothers in labour are used to the standard via observing with the aim of assessing the correct use of the partograph for mothers in labour in Addis Ababa. Even though other studies show only the quantitative part but this study used quantitative data by triangulating with observation to dig out the real factors that affects partograph utilization.
So the result of this study helps to inform the institutions participating in this study about factors that affect partograph use and ways of increasing partograph utilization. And also it informs on areas where supervision strategies need to be enhanced as it relates to instruction on partograph, its purpose, correct use at labour follow-up and referral from health center to hospital.
In addition, the results from this study contribute to the understanding extent of utilization of partograph among obstetric care givers. Moreover, the findings from this study could provide baseline information for further studies on the use of partograph and quality care in the labour wards in selected institutes, and in Addis Ababa health facilities in general.
Method and Materials
Study Area and Period
The study was conducted in governmental health institutions of Addis Ababa, Ethiopia. Addis Ababa is the capital city of Ethiopia as well as the seat of the African Union and different international offices. It covers an estimated area of 174.4 square kilometers. This region has an estimated density of 5,535.8 people per square kilometer based on 2007 census of the central statistical agency of Ethiopia. The total population of Addis Ababa as the projected estimation for the year 2014 was 3.55 million. The number of females in reproductive age group constitutes 35.5% of the total population of Addis Ababa. There are 106governmental health institutions and 11 referral hospitals; the total number of midwifes working in public health institutions is 1,017 (Addis Ababa food medicine and health care administration authority annual review meeting unpublished 2017/2018) and the study was conducted from February - June 2022.
Study Design
Institutional based qualitative study design method was conducted.
Totally 68 labours were observed by selecting them purposively. Two cases from each hospital and from each health center were observed (of those who were in the sample in quantitative parts) whether they use the Partograph in obstetric ward/unit, during active first stage of labour while they follow a laboring woman and how they use and fill parameters on the chart, by using structured checklist which was adapted from WHO.
In-depth interview was conducted among purposively selected 68 key informants from each public health institute to explore specific factors or reasons and difficulties that keep health workers from using Partograph.
Operational Definitions
Obstetric Care Givers
A certified health personnel who provided care for the woman during labor and delivery.
Data Collection Tools and Procedures
Both facilitators and supervisors were given one day of intensive training before the actual data collection day about the aim of study, procedures and data collection techniques going through the questionnaires, ways of collecting the data clarification will be given in basic skill of communication with the study participants.
Those obstetric care givers who had been practicing partograph routinely to monitor all laboring mother was considered as partograph utilize and those who had not been practicing, who were practicing sometimes and occasionally was considered as not utilize.
Quality Assurance
The quality of the data was assured through careful design and pre-testing of the questionnaire. Proper training of the interviewer and supervisor’s cloth supervision of the data collectors and proper handling of the data were made monitor frequently additional data in the field and during data completed questionnaire will be examined for its be done carefully by the principal investigator and experienced data clerk after cleaning the data.
Data Analysis
It was analysed and narrated by using open code, Ethical Consideration After approval of the proposal and getting Ethical clearance for the study was obtained from, Tirunesh Beijing Hospital research center review board committee and legal letter was given to authorized body. The purpose of the study was explained to respondents and verbal informed consent was obtained from participants. Confidentiality of information was maintained by omitting any personal identifier from the questionnaires. The collected data was kept in the form of file in secure place where no one can access it except the investigator.
Results
More than three fourths (75.3%) of the obstetric care providers were knowledgeable about partograph. Almost all (99.8%) of the participants were learned about Partograph at college or university. Again two thirds (70%) of them received on the job training on Partograph. About (97.3%) respondents know that the important of partograph to prevent obstetric complications while 2.7% respondents do not know this. This difference also in line with some respondent’s idea as follow: • I think partograph is not that much important in our country rather it is used for developing country. Even if we use partograph according to the standard, almost all laboring mothers will be crossed the action line and they will suffer for unnecessary interventions.
According to the response of the respondent, the majorities of participants had a good understanding of the progress of labour and were able to examine women in labour according to the powers, the passage and the passenger during poor progress of labour. It is important that active phase of labour be monitored to assess if there is progress in the labour process and to detect problems promptly. These responses illustrate this point:
- The pregnant woman in labour will not be progressing well if she crossed the action line of the Partograph and the presenting part does not descent with each contraction.
- Progress of labour is determined by progressive cervical dilatation, further descent of the presenting part and good uterine contractions. If there is a problem with any of these then there will be poor progress of labour.
These indicate that participants had knowledge of the progress of labour, and they would be able to examine the pregnant woman in labour looking at the powers, the passage, the passenger, and the patient (woman in labour) to identify the cause of the poor progress of labour and notify the doctor early.
Some participants, however, have shown that they did not know progress of labour with regards to the cervical dilatation:
- I expect the cervix of a primigravida to dilate at a rate of one centimeter two (2) hourly while the cervix of a multipara is to dilate at a rate of two (2) centimeters two (2) hourly.
- I expect the cervix to dilate at a rate of one (1) centimeter per hour regardless of whether it is of a primigravida or of a multipara.
Based on these responses such participants would provide the standard obstetric care and thus put the pregnant woman in labour at risk of postpartum hemorrhage and puerperal sepsis. It is likely that these participants would continue to monitor progress of labour until it might be too late as this would be normal to them.
This study showed that some of participants lacked skills to analyze and interpret findings documented on the Partograph. This places the woman in labour at risk of prolonged labour which may lead to further complications.
- Sometimes I will progress the woman in labour even when she has crossed action line without referring her if the mother and the foetus seems normal.
- If I find a Partograph that I feel that the cervical dilatation and descent are not plotted correctly or is spoiled I will put in a new sheet of the Partograph and start plotting my findings.
Attitude of Respondents towards Partograph Utilization
Most of obstetric care givers (84.9%) of them agreed that Partograph can reduce maternal and newborn death. And 78.0% of obstetric care givers agree that Partograph is necessary to improve quality of care.
In qualitative part, participants also mentioned that the Partograph may have quality-of-care benefits that go beyond effective labour monitoring and management. The Partograph on its own does not address all aspects of quality of care, but it can play an important role. Like that Partograph can enhance communication among providers, increase interaction between providers and the laboring women, promote continuity of care across providers, and encourage teamwork. One of the participants indicated that.
Using Partograph practically is necessary to identify maternal and foetal complication but most of us not using it according to the standard. Even if practically some of us have difficulty in assessing and interpreting the finding to document on the graph.
Partograph Utilization
Practice of using Partograph was also assessed among 68 clients by direct observation in the sampled health institutions when health care providers were attending women in labour. Of those observed cases all 100% have Partograph sheet attached to their card. Only 73.3% filled almost all parameters in Partograph, of which 36.4% fill in the right time according to WHO criteria while the rests were filled the parameter but not in the right time. Like foetal heart rate and uterine contraction should be counted every 30 minute if there is no foetal and maternal complication, only five out of eighteen parameters on the Partograph (client name, foetal heart rate, uterine contraction, time and cervical dilatation) were completed properly of those who used Partograph whole parameters on the partograph.
Reasons for Not Using the Partograph
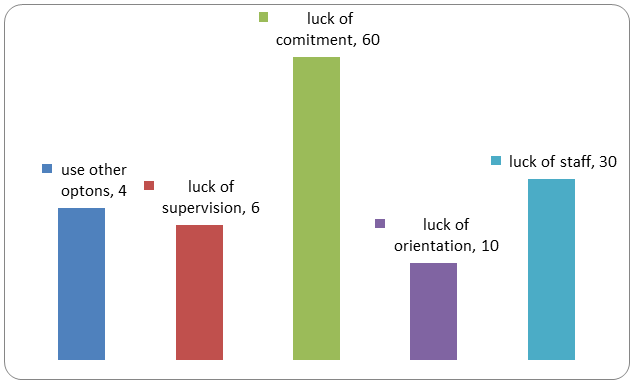
The main factors that were reported by the respondents as influencing against effective use of the Partograph was lack of commitment 60(54.5%) followed by luck of staff 30(27.3%).
Almost all of the respondents during interview mentioned the same idea and said that health care providers did not use Partograph consistently because of different things like work load, lack of commitment, negligence and also some of them do not appreciate the importance of Partograph. On the other hand they indicate skill incompetency and lack of supportive and facilitative supervision. Using Partograph consistently need a great commitment and strong supportive supervision and enough staff. • As far as the mother and fetal condition is normal, following with a Partograph every 30 minutes is not practical and we forget that we need to document.
Some respondents from hospital stressed on the problems of referral system and some of women in labour were referred from health centers as emergency case arrived at hospital without proper documentation of Partograph. Even if they referred without drawing cervical dilatation and patterns of foetal heart beat on partograph which is difficult to provide crucial information about the preceding hours or days of that labour. And they mentioned verbally as follow: • We can just say it is negligence or lack of supervision. Sometimes there is enough time to observe and follow with a Partograph according to the standard but we don’t do it.
The qualitative study participants agreed that this tool is necessary at all levels to follow a labouring mother and control any deviation from normal. However, health workers surfaced some challenges they faced on the theoretically accepted level of cervical dilatation at 4cm. This is because if it started early at 4cm some clients may cross action line despite of any abnormal sign on both mother and foetus. So it may mislead or hurry the concerned person to take unnecessary intervention.
Participants agreed that health professionals need to know more about Partograph training, experience, competence, management, and supervision. Senior clinicians have to be included in the training on paragraph promoting and appreciating staffs that were used the tool correctly and consistently needs encouragement.
Most participants indicated that a shortage of staff affects the utilization of the Partograph and may result in incorrect monitoring pregnant of women in labour.
This sentiment was verbalized variously as follows:
- Participant from health center said that the problem is that most of the time we are only 3 obstetric givers in a shift and mostly 3 up to 5 labouring mothers came per day, so we will be expected to monitor all the women in the labour ward until the next shift comes in.
- A participant from hospital said that “If we use Partograph according to the standard, we will spent the whole time on one labouring mother and the rest labouring mothers may not get the service for example contraction should be counted every 30 minute for 10 minutes this is not practical when we follow more than two labouring mothers at the same time.
- The problem is that if one woman delivers and complicates I will have to spend more time on that complicated delivery and will miss monitoring the other women on due time.
Discussion
This study focused on obstetric care givers in public health institutions of Addis Ababa, Ethiopia, specifically, at delivery units. Findings from the study may therefore be regarded as a window that provides a glimpse into current utilization of paragraph and associated factors within the study area.
As well as study conducted in Addis Ababa before five years (69%) was greater than the results of this study, this difference may also that due to the difference in sampling technique [8]. The other possible explanation could be different in data collection procedure. This implies that even though the Partograph is a simple and inexpensive tool which prevents maternal deaths and complications due to obstructed or prolonged labour, it is not as widely implemented as it should be.
On the other hand, the result of this study is slightly lower than the study done in west Showa Oromia region (84.6%) This discrepancy might be due to different in place of the study and the different strategies in Partograph utilization, different level of knowledge and attitude of care providers towards Partograph. Moreover this study conducted on midwives, nurses, health officers and medical doctors but a study on west Showa Oromia region conducted only on a single profession of midwifery with a great chance to be trained on Partograph than other professions.
In this study client name, foetal heart rate, uterine contraction, time and cervical dilatation were completed properly but time of rupture of membrane 88.3%, status of amniotic fluid 95%, and moulding of foetal head 90% recorded but most of them are not in the right time. Most of the obstetric care givers fill the Partograph after the Mather is giving birth which is used for neither the mother nor the foetus; this is revealing of poor monitoring of parameters on the Partograph against standards. In the present study the reasons for not using Partograph during labour were; using different monitoring tools other than Partograph, lack of commitment, lack of supervision and lack of orientation on how to use the Partograph being used at the institution. This finding is more or less consistent with the study in Nigeria, Addis Ababa and west Showa Oromia region.
In this study work place i.e. working in Hospitals makes professionals less likely to use Partograph than those health caregiver working at heath center (AOR= 24.57, CI: 7.64- 78.99) this is also consistent with the study done in west Showa Oromia region. This may be because health workers at health centers use Partograph as a guide to take action early since should have adequate evidence/justification even to refer the labouring women to Hospital for better management. Furthermore, they had less client load and most of them received recent training. In contrast, health workers from Hospitals may be overconfident and neglect to monitor the labouring mother by using Partograph tools since they think that encase if the mother got complications they can easily manage the complication at their own premises without wasting time for transporting to other facilities.
On the other hand professionals who work in an institute which have adequate staff were more likely use partograph than those professionals who work in an institute which have no adequate staff (AOR=15.73, CI= 5.18-47.79). This may be due to that if adequate staff is available in health institute they use partograph properly. Indirectly it shows that if there is a crowdedness of labouring mother and if there is lack of staff in an institute then the professionals have no time to use partograph to follow each labouring mother.
Commitment of obstetric caregiver also one factor identified by this study by which obstetric care givers which have commitment to use partograph were more likely to use partograph than those professionals who have no commitment to use partograph (AOR= 12.74, CI=4.69- 34.62). This may be due to those professionals who have commitment are more self-initiated than those who have not commitment. Accordingly during observation there were incomplete and poor recording of parameters on the Partograph against the recommended standards of WHO parthograph that reflect poor commitment and skills of birth attendances on the use of a Partograph. Even though they fill some parameters on partograph they didn’t measure it on the right time. Out of 66 obstetric care givers observed when they attend labour 44 were fill almost the all parameters of which only 16 of them fill in the right time. This shows that there is high discrepancy between the quantitative part reported and the real utilization of partograph.
Respondent’s attitude on analysis, 69.8% had favorable attitude above mean value whereas 30.2% had unfavorable attitude below mean toward Partograph utilization which misleads management as the progress of labour and the partograph alert line are not aligned in most pregnant woman may be leads to unnecessary interventions while the condition of both mother and foetus were in normal condition.
Strength and Limitations
Strength of the Study
Being qualitative research methodology made it more strong.
Limitation of the Study
It cannot establish cause and effect relationships.
Conclusion
This study showed that utilization of partograph among obstetric care givers is high which indicates there is a better use of partograph to care the laboring mother. In this study, lack of staff and commitment also significantly associated with partograph utilization. But observationally mostly it was not plotted according to WHO standards. Despite the reported use of partograph, observation findings indicated that continues monitoring of maternal and foetal condition was lacking. Most providers put the partograph paper in the client card after they complete the delivery procedure only to fulfil the format for the sake of reporting and some of the parameters plotted only once. This will then put women and their fetus in danger.
Recommendation
To Addis Ababa Regional Health Bureau (AARHB)
Adequate number of obstetric care givers should be presented to each public health institution.
To Stake Holders
- Monitoring and supervision of obstetric staff to ensure appropriate use of the Partograph should been given highest priority by every hospital administrator.
- The hospital administrators and HC leaders should motivate and appreciate those obstetric care givers who use partograph routinely.
To Obstetric Care Providers
• Every labouring mother should be monitored by partograph according to WHO criteria in the right time. Which needs a great commitment
Declaration
Ethical Approval and Consent to Participate
Ethical approval and clearance were obtained from research and ethical committee of Tirunesh Beijing Hospital research center and Addis Ababa research and emergency management directorate Institutional Review Board. Informed written consent was obtained from all study participants. Participants were informed about the objective of the study. After information is provided about purpose of the study, confidentiality of the information and all the participants were reassured of the anonymous (unnamed), and as personal identifiers was not used. The study was also carried out following relevant guidelines and regulations according to the Helsinki declaration.
Availability of Data and Materials
All data included in this manuscript can be accessed from the corresponding author upon request through the email address.
Competing Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent for Publication
Not applicable
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Acknowledgements
We would like to thank Mr. Zelalem Ayalew and Mr. Belay Getahun for their constant input during the development of this research thesis. And our heartfelt thanks and appreciation also goes to the study participants, hospitals involved in this study, to my family and friends who provide with helpful information and essential materials during this thesis preparation.
References
-
WHO (1994) World health organization partograph in management of labor. Lancet 343(8910): 1399-1404.
-
Fawole A, Adekanle DA (2008) Knowledge and utilization of the partograph among obstetric care giversIn south west Nigeria. African Journal of Reproductive Health 12(1): 22-29.
-
Kunnal K, Shinde VBB, Rashmi K (2012) Study of course of labor by using modified who partograph. International Journal of Biomedical and Advance Research 3(5).
-
Oldapo OT, Olatunji AO, Daniel OJ (2006) Knowledge and use of partograph among health care personnel at the peripheral maternity centers in Nigeria. J Obstet Gynaecol 30(6): 538-541.
-
Fawoel AO, Adekanle DA, Hunyinbo KI (2010) Utilization of the partograph in primary health care facilities in south western Nigeria. Nigerclinpract 13(2): 200-204.
-
Mrinal N, Cohopade M (2010) A study to assess the effectiveness of instructional module for nurses on use of partograph during labor in selected district hospital at Bijapur, Katnastak state, TulzaBhavani college of Nursing.
-
Wamwana EB, Ndavi PM, Gichangi PB, Karanja JG, Muia EG, et al. (2007) Qualityof record keeping in the intra-partum period at the provincial general hospital, kakamega, kenya. East Africa medical journal 84(1): 16- 23.
-
Yisma E, Dessalegn B, Astatine A, Fesseha N (2013) Knowledge and utilization of partograph among obstetric care givers in public health institutions of Addis Ababa, Ethiopia. BMC pregnancy and childbirth 13(17): 1-9.
-
Plotkin M, Tibaijuka G, Currie S, Lacoste M (2010) Quality of care for prevention and management of common maternal and newborn complications: A study of 12regions in Tanzania. Maternal and child health integrated program, pp: 54.
-
USID (2013) Percent of deliveries in which a partograph is correctly used.
-
World Health Organization (2012) Maternal mortality.
-
Yisma E, Dessalegn B, Astatkie A, Nebreed F (2013) knowledge and utilization of partograph among Obstetric care givers in public health institution of Addis Ababa, Ethiopia, BMC pregnancy and child birth 13: 17.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’