A Randomized Controlled Trial to Compare Intraveous Ferric Carboxymaltose with Oral Iron for Treatment of Post-Partum Anemia
Objectives: To compare the efficacy of ferric carboxymaltose (FCM) with oral iron in management of post-partum anemia. Materials and Methods: A total of 230 post-partum women aged >18 years having Hb level <10 g/dl on post-natal day 1 were randomized to receive either oral iron (ferrous fumarate tablets 200 mg for 06 weeks) or intravenous FCM (dose calculated by Ganzoni’s Formula, total iron dose = [actual body weight x (15 - actual Hb)] x 2.4 + iron stores). Demographic, obstetric and hematological profile (Hb and serum iron profile) was estimated at the time of enrolment. The women were followed up after six weeks. Non-complying women were excluded from the study. Change in Hb levels, serum iron profile and number of women achieving Hb>10 g/dl was noted. Data was compared using Chi-square and Independent samples ‘t’-test respectively. Results: A total of 218 women (107 in FCM and 111 in oral iron group) completed the study. Mean age of women was 26.67±4.31 years. Mean pre-intervention Hb level was 9.11±0.62 and 9.15±0.61 g/dl respectively in FCM and oral iron groups (p=0.630). At follow-up these values were 11.11±0.89 and 10.78±0.88 g/dl respectively in the corresponding groups (p=0.006). Mean change in Hb level and number of women achieving targeted Hb level were significantly higher in FCM as compared to that in oral iron group (p<0.05). Serum iron reserves were also found to be significantly higher in FCM as compared to oral iron group. Conclusion: Intravenous FCM had an edge over oral iron in management of post- partum anemia.
Shivani*, Nair VG and Rai G
Introduction
Anemia in reproductive age women is quite common with almost every third woman in reproductive age group having anemia [1]. Nutritional deficiencies, particularly malnutrition and anemia are quite common during pregnancy in throughout the world. Its prevalence in developed countries is 14%, in developing countries 51%, whereas in India, it varies from 65% to 75% [2, 3]. India witnesses a high prevalence of anemia in reproductive age women both during and after pregnancy [4, 5, 6].
Anemia during post-partum phase is an important determinant of not only the maternal health but that of child’s health too as exclusive breastfeeding is recommended and is the solitary source of nutrition for the child [7].
Oral ferrous iron remains to be the primary choice for management of mild-to- moderate anemia but it has been seen to produce mixed results [8, 9]. One of the issues with oral ferrous iron is frequency of its intake. Owing to a limited bio-absorbability of iron through oral route, oral ferrous iron supplementation needs to be given in split dosages requiring twice or thrice daily intakes [10]. Being a prolonged regimen requiring frequent intake of oral ferrous iron, a number of women fail to maintain regularity in its intake, resulting in less promising results. In the recent years, some alternative, that require fewer dosages, to be administered on weekly intervals have emerged as a promising choice. Ferric carboxymaltose, a formulation having low pH [5, 6, 7] and physiological osmolarity has been seen to be effective for management of anemia for upto six months of post-partum life [11]. It is one of the most suitable alternatives for safe administration even in high single doses over shorter time periods (single dose up to 1000 mg over 15 min) thus giving it an edge over other parenteral preparations [12]. Despite being used clinically for the last two decades, it has not yet been established as the standard treatment for management of post-partum anemia owing to lack of clinical evidence in form of randomized clinical trials in different populations. Hence, this prospective randomized-controlled trial was carried out to compare the safety and efficacy of ferric carboxylase for management of post-partum anemia in comparison with oral iron supplementation.
Material and Method
This prospective randomized controlled trial was carried out at a tertiary care centre in North India after obtaining approval from the Institutional Ethics Committee. A total of 230 post-partum women with hemoglobin level <10 g/dl on post-natal day 1 were enrolled in the study using a purposive sampling method applying continuous variable, non-inferiority design with wastage factor of 15%. Unwilling women, those having history of tuberculosis, systemic or endocrine disorders, hemoglobinopathies and hypersensitivity to iron were excluded from the study.
At enrolment, age, obstetric history, details regarding index pregnancy and mode of delivery were noted. Hematological parameters like serum hemoglobin, platelet count, mean corpuscular volume (MCV), mean corpuscular hemoglobin concentration (MCHC), serum iron reserves (ferritin, total iron binding capacity and iron) were also assessed.
The women were then randomized to the two study groups as follows:
- Intravenous FCM Group (n=115): In this women all the patients delivering on odd number dates were enrolled till the completion of sample size. Women in this group received intravenous FCM (dose calculated by Ganzoni’s Formula, total iron dose = [actual body weight x (15 - actual Hb)] x 2.4 + iron stores).
- Oral Iron Group (n=115): In this women all the patients delivering on odd number dates were enrolled till the completion of sample size. Women in this group received oral iron (ferrous fumarate tablets 200 mg for 06 weeks) The intervention was carried upto six weeks.
After six weeks of intervention, the women were called for follow-up. Non-complying women, those failing to turn up on within one week of scheduled follow-up were excluded from the study.
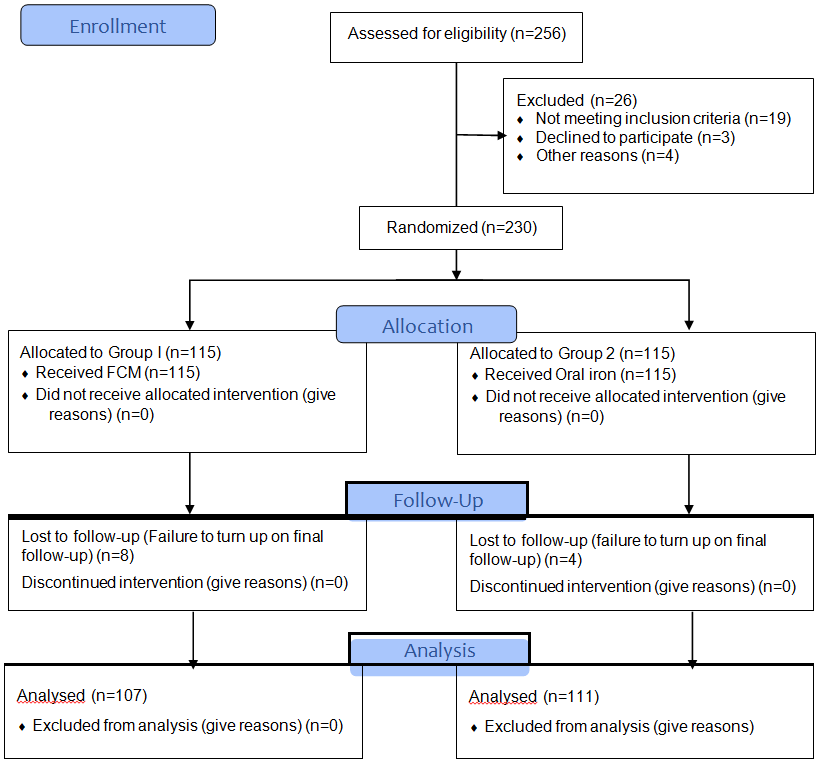
During the course of intervention, a total of 15 women in each group discontinued treatment. A total of 8 women in i.v. FCM group and 4 in oral iron group failed to turn up at last follow-up.
A total of 218 women were available for follow-up at six weeks –107 in intravenous FCM and 111 in oral iron group (Figure 1).
At final follow-up, all the women were assessed for change in hemoglobin and serum iron profile. Adverse effects, if any, were also noted.
Number of women achieving Hemoglobin level >10 g/dl were also noted in both the groups.
Data Analysis
The data was analyzed using IBM SPSS Stats 21.0 software.
Data has been depicted as numbers and percentages or mean/median and standard deviation/ interquartile range. Chi-square test was used for comparison of qualitative and Independent samples ‘t’-test were used for comparison of continuous data. Non- parametric data was compared using Mann-Whitney U test.
Results
Age of women ranged from 19 to 42 years, mean age of women was 26.67±4.31 years. Median gravida was 2. There were 68 (31.2%) women having abortion history, 18 (8.26%) preterm, 35 (16.06%) unbooked and 92 (42.2%) caesarean deliveries. Mean platelet count, MCV and MCHC values were 229±100 thousands/cumm, 74.1±4.5 fl and 34.8±5.32 g/ dl respectively in i.v. FCM and 218±101 thousands/cumm, 74.1±4.12 fl and 35.0±4.18 g/dl respectively in oral iron group. Mean serum ferriting, TIBC and S. iron levels were 25.1±2.03 ng/ml, 517.6±31.11 µg/dl and 38.9±7.33 µg/dl respectively in i.v. FCM and 25.3±2.22 ng/ml, 517.0±24.95 µg/dl and 37.0±6.53 µg/dl respectively in oral iron group. Statistically, there was no significant difference between the two groups for age, obstetric profile, baseline hematological parameters and iron profile (p>0.05) (Table 1).
| SN | Variable | I.V. FCM (n=107) | Oral Iron (n=111) | Total (n=218) | Statistical significance |
|---|---|---|---|---|---|
| 1 | Mean age±SD (Range) Years | 26.26±4.32 (19-39) | 27.05±4.27 (19-42) | 26.67±4.31 (19-42) | t=1.361; p=0.175 |
| 2 | Median Gravida (IQR) | 2 (1, 3) | 2 (1, 3) | 2 (1, 3) | z=0.355; p=0.722 (Mann- Whitney U test) |
| 3 | Abortion history | 34 (31.8%) | 34 (30.6%) | 68 (31.2%) | c2=0.033; p=0.855 |
| 4 | Multiple fetuses | 0 (0%) | 3 (2.7%) | 3 (1.4%) | c2=2.932; p=0.087 |
| 5 | Preterm delivery (<37 weeks) | 9 (8.41%) | 9 (8.11%) | 18 (8.26%) | c2=0.007; p=0.935 |
| 6 | Unbooked delivery | 15 (14.02%) | 20 (18.02%) | 35 (16.06%) | c2=0.647; p=0.421 |
| 7 | Caesarean delivery | 38 (35.51%) | 54 (48.65%) | 92 (42.20%) | c2=3.853; p=0.050 |
| 8 | Mean Platelet count ±SD (Range) thousands/cumm | 229±100 (26-532) | 218±101 (38-584) | 223±4.33 (26-584) | t=0.798; p=0.426 |
| 9 | Mean MCV±SD (Range) fl | 74.1±4.54 (61-83) | 74.1±4.12 (64-87) | 74.1±4.33 (61-87) | t=0.112; p=0.911 |
| 10 | Mean MCHC±SD (Range) g/dl | 34.8±5.32 (26-84) | 35.0±4.18 (26-71) | 34.9±4.77 (26-84) | t=0.251; p=0.802 |
| 11 | Mean Serum ferritin±SD (Range) (ng/ml) | 25.1±2.03 (10-48) | 25.3±2.22 (10-29) | 23.0±5.35 (10-48) | t=0.098; p=0.924 |
| 12 | Mean TIBC±SD (Range) µg/dl | 517.6±31.11 (352- 591) | 517.0±24.95 (405- 583) | 502.9±32.40 (352- 583) | t=0.035; p=0.973 |
| 13 | Mean S. Iron±SD (Range) µg/dl | 38.9±7.33 (25-58) | 37.0±7.53 (9-49) | 37.9±7.47 (9-58) | t=1.820; p=0.070 |
| SN | Hb Level | I.V. FCM (n=107) | Oral Iron (n=111) | Total (n=218) | Statistical significance |
| 1 | Pre-intervention Mean Hb±SD (Range) g/dl | 9.11±0.62 (7.1-9.9) | 9.15±0.61 (7.0-9.9) | 9.13±0.61 (7.0-9.0) | t=0.482; p=0.630 |
| 2 | Post-intervention Mean Hb±SD (Range) g/dl | 11.11±0.89 (8.5-13.8) | 10.78±0.88 (8.6-13.3) | 10.94±0.90 (8.5-13.8) | t=2.762; p=0.006 |
| 3 | Mean change in Hb±SD (Range) as compared to baseline (g/dl) | 2.00±1.02 (-0.6-4.90) | 1.63±0.98 (-0.60-4.70) | 1.81±1.02 (-0.60-4.90) | t=2.741; p=0.007 |
| 4 | Mean % Change in Hb levels as compared to baseline±SD | 22.48±12.44 (-6.12- 58.11) | 18.24±11.71 (-6.51- 55.95) | 20.33±12.23 (-6.52- 58.11) | t=2.592; p=0.010 |
| 5 | No. of women achieving Hb >10 g/dl | 99 (92.5%) | 86 (77.5%) | 185 (84.9%) | c2=9.60; p=0.002 |
Table 1: Comparison of Age and Obstetric Profile of women in two study groups.
Before intervention, mean Hb level was 9.11±0.62 g/ dl in i.v. FCM and 9.15±0.61 g/dl in oral iron group, thus showing the difference between two groups not to be significant (p=0.630). At six-weeks follow-up, mean Hb level was significantly higher in i.v. FCM group (11.11±0.89 g/dl) as compared to that in oral iron group (10.78±0.88 g/dl) (p=0.006). Mean change in Hb was 2.00±1.02 g/dl in i.v. FCM as compared to 1.63±0.98 g/dl in oral iron group (p=0.007).
During the intervention period, mean change in Hb level was 22.48±12.44% in i.v. FCM as compared to 18.24±11.71% in oral iron group (p=0.010). Significantly higher proportion of women in i.v. FCM group (92.5%) as compared to oral iron group (77.5%) achieved Hb level >10 g/dl after the intervention (p=0.002) (Table 2).
At follow-up, mean serum ferritin, serum iron and transferrin saturation were significantly higher and TIBC levels were significantly lower in i.v. FCM as compared to oral iron group (p<0.05). However, there was no significant difference between the two groups for MCV and MCHC levels (p>0.05) (Table 3).
| SN | Parameter | I.V. FCM (n=107) | Oral Iron (n=111) | Statistical significance |
|---|---|---|---|---|
| 1 | MCV (fl) | 87.05±5.50 | 85.64±5.97 | t=1.812; p=0.071 |
| 2 | MCHC (g/dl) | 33.77±2.09 | 33.63±2.09 | t=0.482; p=0.631 |
| 3 | Serum ferritin (ng/ml) | 33.79±5.38 | 31.23±5.31 | t=3.521; p=0.001 |
| 4 | TIBC (µg/dl) | 310.10±54.14 | 335.14±65.65 | t=3.065; p=0.002 |
| 5 | S. Iron (µg/dl) | 95.24±19.90 | 86.71±7.67 | t=3.354; p=0.001 |
| 6 | Transferrin saturation (µg/dl) | 82.13±14.73 | 77.94±14.80 | t=2.098; p=0.037 |
Table 2: Comparison of hematological parameters at follow-up between two study groups (Mean±SD).
Mean increment in serum ferritin and serum iron levels and mean decline in TIBC levels was significantly higher in i.v. FCM as compared to oral iron group (p<0.05) (Table 4).
| SN | Parameter | I.V. FCM (n=107) | Oral Iron (n=111) | Statistical significance |
|---|---|---|---|---|
| 1 | Serum ferritin (ng/ml) | 10.62±7.34 | 8.46±6.48 | t=2.302; p=0.022 |
| 2 | TIBC (µg/dl) | -193.10±60.61 | -167.44±66.69 | t=2.970; p=0.003 |
| 3 | S. Iron (µg/dl) | 56.38±20.62 | 49.68±17.85 | t=2.571; p=0.011 |
Table 3: Between group Comparison of Change from baseline in Serum Ferritin, Iron and TIBC at follow-up.
No serious side effect was noted in either of two groups. None of the drop-outs were because of adverse effects of the drugs.
Discussion
In the present study, we observed a better treatment response in i.v. FCM as compared to oral iron group. Clinical response rate in terms of achievement of Hb >10 g/dl was 92.5% in i.v. FCM as compared to 77.5% in oral iron group. Simultaneously, improvement in iron profile was also significantly higher in i.v. FCM as compared to oral iron group. Both oral iron as well as i.v. FCM were safe and well-tolerated. Ferric carboxymaltose (FCM) is a novel iron complex that can be administered intravenously and has reportedly been found to be safe- and well-tolerated apart from being effective in the treatment of iron-deficiency anaemia [13]. It has been found to produce a faster and better treatment response in management of post-partum anemia as compared to oral ferrous sulphate in earlier studies too [14, 15, 16, 17, 18].
In the present study, following six weeks of intervention, mean increment in Hb level was 2.00±1.02 g/dl in i.v. FCM as compared to 1.63±0.9 g/dl in oral iron group. However, in an earlier study, Van Wyck DB, et al. [14] found mean time taken for an increment of 2 g/dl in Hb level in FCM group to be only 7 days as compared to 14 days in oral iron group [14]. In the present study, however, we did not make mid-intervention assessments for hemoglobin levels and made assessment at 6 weeks only. However, compared to the present study, where mean increment in Hb level at the end of six weeks was only 2 g/dl in FCM and 1.63 g/dl in oral iron group, Rathod S, et al. [19] observed this increase to be much higher in both FCM (4.4 g/dl) as well as oral iron (2.13 g/dl) groups following similar duration of intervention [19]. The reason for this could be inclusion of a high proportion of patients with severe anemia (Hb<7 g/dl) in their study. In the present study, baseline Hb level of study population was 9.13±0.61 g/dl whereas in their study population mean baseline Hb level was <8 g/dl. Thus, in the present study, despite having a relatively less severe anemic patients, we found a similar trend of change depicting a superiority of FCM over oral iron over the same duration of intervention. With respect to magnitude of change in Hb levels and their trends, the findings of the present study close to the observations of Damineni and Thunga who observed a mean increase of 3.23 g/dl in FCM as compared to 2.25 g/dl in oral iron group following six weeks of intervention [20]. Another study by Chawla S, et al. [18] reported the mean increment in Hb level to be 3.76 g/dl in FCM as compared to 2.48 g/dl in oral iron group [18]. Compared to these studies, the present study did not yield equivalent increment in either of two groups despite showing trends similar to theirs. The probable reason for this could be difference in general dietary pattern or difference in population characteristics. The present study had a high proportion of women having an abortion history (31.2%), moreover a sizeable proportion of patients were unbooked (16.1%) and had a high proportion of those who underwent caesarean delivery (42.2%). These complications might have an impact on the recovery pathways too, depicting a relatively less striking treatment response in both the study groups. Differences in intervention method may also interfere with the overall performance of intervention. Incidentally, there are tremendous differences in intervention methods in different studies. In the present study, we used (dose calculated by Ganzoni’s Formula, total iron dose = [actual body weight x (15 - actual Hb)] x 2.4 + iron stores) for intravenous FCM and (ferrous fumarate tablets 200 mg for 06 weeks) for oral iron supplementation. Chawla S, et al. [18] in their study gave 200 mg ferrous sulfate one tablet daily in the oral iron group and one dose of 1000 mg FCM stat in 250 ml of normal saline over 15 min in the intravenous group. [Error! Bookmark not defined.] Vanobberghen F, et al. [17] used 1000 to 2000 mg FCM – in one or two doses in the intravenous group and three dried ferrous sulphate tablets of 200 mg containing 60 mg of elementary iron and 5 mg of folic acid every morning for 3 months in the oral iron group. [Error! Bookmark not defined.] Damineni and Thanga on the other hand used single dose 1000 mg FCM in the intravenous group and 100 mg twice daily ferrous ascorbate in the oral group [20]. These differences in the drug regimens could result in differences in the treatment response.
As far as treatment response (in terms of achievement of Hb level >10 g/dl) is concerned, the present study found it to be 92.5% in FCM as compared to 77.5% in oral iron group. Vanobberghen F, et al. [17] in their study targeted Hb level 11 g/dl as the primary treatment outcome and achieved it in 82% of FCM as compared to 79% in oral iron group [17]. Compared to their study, relatively higher treatment success rate in the present study could be owing to a lower cut-off, however, in the present study, the difference between FCM and oral iron group was much higher (92.5% vs 77.5%) as compared to their study (82% vs 79%).
In the present study, we found that simultaneous to a higher increase in serum Hb levels in the i.v. FCM as compared to oral iron group, the increase in iron reserves was also significantly higher in i.v. FCM as compared to that in the oral iron group. This is in agreement with the observations made by workers too [12, 16, 18, 20]. The differences in change in iron profile of the patients in the two intervention groups tend to describe the underlying mechanisms for maintaining hemoglobin levels as a result of intervention.
The findings of the study thus depict that i.v. FCM is a viable and safe alternative to oral iron supplementation for management of post-partum anemia. The present study was limited to study of clinical outcomes only. Further studies, targeting the patient satisfaction and acceptability of two intervention methods are recommended.
Conclusion
Intravenous FCM was found to be a better and safer alternative to oral iron supplementation for treatment of post-partum anemia. Further studies on larger sample size covering aspects such as economic costs, patient acceptability and satisfaction are recommended.
References
-
World Health Organization (2021) Anaemia in Women and Children: WHO Global Anaemia Estimates, 2021 Edition.
-
Marahatta R (2007) Study of anaemia in pregnancy and its outcome in Nepal medical college teaching hospital, Kathmandu, Nepal. Nepal Med Coll J 9(4): 270-274.
-
Kalaivani K (2009) Prevalence and consequences of anaemia in pregnancy. Indian J Med Res 130(5): 627- 633.
-
Ganapathi KC, Kumar KS (2017) A cross-sectional study of anemia among women of reproductive age group (15- 49 years) in a rural population of Tamil Nadu. Int J Med Sci Public Health 6(3): 524-529.
-
Kalaivani K, Ramachandran P (2018) Time trends in prevalence of anaemia in pregnancy. Indian J Med Res 147(3): 268-277.
-
Selvaraj R, Ramakrishnan J, Sahu SK, Kar SS, Laksham KB, et al. (2019) High prevalence of anemia among postnatal mothers in Urban Puducherry: A community- based study. J Family Med Prim Care 8(8): 2703-2707.
-
Britton C, Cormick FMM, Renfrew MJ, Wade A, King SE, et al. (2007) Support for breast feeding mothers. Cochrane Database System Review 24(1): CD001141.
-
Mello-Neto JM, Carvalho-Rondo PH, Oshiiwa M, Morgano MA, Zacari CZ, et al. (2013) Iron Supplementation in Pregnancy and Breastfeeding and Iron, Copper and Zinc Status of Lactating Women From a Human Milk Bank. J Trop Pediatr 59(2): 140-144.
-
Jorgensen JM, Yang Z, Lönnerdal B, Chantry CJ, Dewey KG, et al. (2017) Effect of iron supplementation during lactation on maternal iron status and oxidative stress: A randomized controlled trial. Matern Child Nutr 13(4): e12394.
-
Stoffel NU, Cercamondi CI, Brittenham G, Zeder C, Geurts- Moespot AJ, et al. (2017) Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials. Lancet Haematol 4(11): 524-533.
-
Kaur R, Kant S, Haldar P, Hamed F, Singh A, et al. (2021) Single Dose of Intravenous Ferric Carboxymaltose Prevents Anemia for 6 Months among Moderately or Severely Anemic Postpartum Women: A Case Study from India. Curr Dev Nutr 5(7): 078.
-
Breymann C, Gliga F, Bejenariu C, Strizhova N (2008) Comparative efficacy and safety of intravenous ferric carboxymaltose in the treatment of postpartum iron deficiency anemia. Int J Gynaecol Obstet 101(1): 67-73.
-
Lyseng-Williamson KA, Keating GM (2009) Ferric carboxymaltose: a review of its use in iron-deficiency anaemia. Drugs 69(6): 739-756.
-
Van Wyck DB, Martens MG, Seid MH, Baker JB, Mangione A, et al. (2007) Intravenous ferric carboxymaltose compared with oral iron in the treatment of postpartum anemia: a randomized controlled trial. Obstet Gynecol 110(2): 267-278.
-
Seid MH, Derman RJ, Baker JB, Banach W, Goldberg C, et al. (2008) Ferric carboxymaltose injection in the treatment of postpartum iron deficiency anemia: a randomized controlled clinical trial. Am J Obstet Gynecol 199(4): 1- 7.
-
Mokshadayini S, Nanda S (2019) Safety and Efficacy of Ferric Carboxy maltose Therapy in Post-Partum Women with Iron Deficiency Anemia. International Journal of Science and Research 8(6): 283-286.
-
Vanobberghen F, Lweno O, Kuemmerle A, Mwebi KD, Asilia P, et al. (2021) Efficacy and safety of intravenous ferric carboxymaltose compared with oral iron for the treatment of iron deficiency anaemia in women after childbirth in Tanzania: a parallel-group, open-label, randomised controlled phase 3 trial. Lancet Glob Health 9(2): 189-198.
-
Chawla S, Tangri MK, Srivastava AK, Bhardwaj D, Indu, et al. (2022) Randomized controlled trial to compare injection ferric carboxymaltose and oral iron in reducing postpartum anemia: A multicenter, pilot study. J Mar Med Soc 24(1): 42-46.
-
Rathod S, Samal SK, Mahapatra PC, Samal S (2015) Ferric carboxymaltose: A revolution in the treatment of postpartum anemia in Indian women. Int J Appl Basic Med Res 5(1): 25-30.
-
Damineni SC, Thunga S (2016) IV Ferric Carboxymaltose Vs Oral Iron in the Treatment of Post-partum Iron Deficiency Anaemia. J Clin Diagn Res 10(11): 8-10.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’