A Postmenopausal Woman with a Clitoral Mass
Although clitoral inclusion cyst is rare, it can cause a variety of bothersome symptoms and possible malignancy. The objective of this article is to present a surgical management option for a clitoral epidermoid inclusion cyst in a postmenopausal woman.
Introduction
An epidermoid cyst is benign and thought to be the result of implantation of superficial epidermal tissue into the dermis or subcutaneous tissue. They are commonly found on any body parts covered by skin. They are also rarely seen in the clitoral or vulvar region; most often associated with prior trauma or surgery to the area, usually female genital mutilation in the under developing countries. A variety of benign and malignant tumors can involve the clitoris [1, 2, 3, 4]. An epidermal inclusion cyst of the clitoris without a history of trauma is uncommon. The prognosis after surgical treatment is usually good with no recurrence or malignant transformation reported till date [2]. Spontaneous clitoral epidermal inclusion cysts are rare with an unclear etiology and their impact on later sexual function has not been described well [3]. The surgical treatment of clitoral inclusion cyst is simple and effective [4, 5]. This case report presents a surgical management option for a postmenopausal woman with clitoral epidermoid inclusion cyst [2, 4, 5].
Case Presentation and Management
Presentation
A 76-year-old Caucasian postmenopausal woman presented at Urogynecology clinic for vaginal bulge. She was unsure how long she had the vaginal mass. She denied the difficulty of urination or pain around the vaginal bulge. She had two normal vaginal deliveries and denied any history of gynecologic cancers, abnormal PAP smear or mammogram in the past. Her past medical history was significant for anal cancer status-post surgical management (complicated by deep vein thrombosis in the lower extremities), chemotherapy and radiation therapy; Migraine headache, bowel dysfunction and Barrett’s esophagus. Her past surgical history included anal cancer surgery, laparoscopic cholecystectomy, and knee replacement. She denied use of illegal drugs, alcohol, or current smoking. She reported that she was recently re-married, and her vaginal bulge was interfering with her sexual intercourse.
The patient had already obtained renal and transvaginal ultrasounds prior to the visit: which were within normal limits: normal kidneys without mass, 4.9 centimeters (cm) of small atrophic uterus with endometrial lining of 3 millimeters. Both ovaries were atrophic, and no free fluid was noted in the pelvis. Vital signs at intake visit were all within normal limits. Physical examination revealed atrophic vulva with a 3 cm x 2.5 cm cystic but formed mass right under the clitoris (Figure 1). Patient denied pain to touch on the mass. No rash, erythema, edema, or lesions were noted on the overlying skin layer. No lymph nodes swelling was noted on both inguinal areas. No clinical pelvic organ prolapse was observed.

Evaluation with Imaging
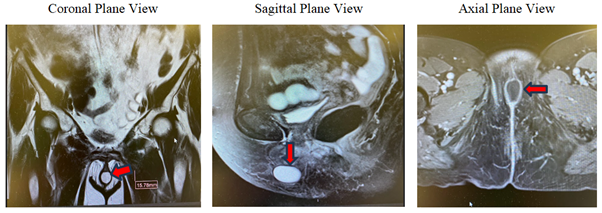
For further evaluation, Magnetic Resonance Imaging (MRI) of pelvis was obtained. The images showed that there was a well-circumscribed lesion at the midline of the lower vagina interposed between the labia majora measuring 2.5 x 1.5x 2.0 cm with T2 signal hyperintensity and T1 signal hypointensity with peripheral enhancement associated restricted diffusion (Figure 2). No mural nodularity of septations in the mass were noted. In addition, no evidence of pelvic lymphadenopathy of inguinal hernia was noted. The possible diagnosis of the clitoral mass by the radiologist was noted to be “clitoral epidermoid inclusion cyst”.
Surgical Planning
The findings were discussed with the patient: although the risk of this mass being malignant is very low, since the patient was bothered by the presence of the vulvar mass (considering newlywed status), mutual decision was made to proceed for the excision of the clitoral mass. Common surgical risks/benefits/alternatives of the planned procedures:
exam under anesthesia, excision of clitoral mass, clitoral hood reconstruction, possible biological graft placement, cystoscopy with simple cystometrogram were discussed in depth, including but not limited to bleeding, infection, pain, voiding dysfunction, decreasing sensual pleasure or loss of sexual sensation from the clitoris, etc. The patient voiced understanding and signed the consent form with a witness present.
Steps of Surgical Management
After appropriate preoperative testing and clearance by her other medical providers, the patient was taken to the operating room, where a time out was performed to confirm the correct patient and procedure. Sequential compression devices were placed on the lower legs and turned on. Gentamycin 80 milligrams (mg) and Flagyl 500 mg were given intravenously as prophylactic antibiotics, as the patient was allergic to the penicillin family. The patient was positioned in dorsal lithotomy with care not to hyperflex

A Lonestar self-retaining retractor was placed for better visualization of the surgical field (Figure 5a). Using a 25-gauge needle, a total of 2 millimeters (ml) of 1 percent lidocaine with epinephrine was injected in the midline of the cyst submucosally without disrupting the underlying cyst, for hemostasis and hydrodissection. A 1.5cm vertical incision was made over the epithelial layer over the cyst, using #15 blade. Then the overlying tissue edges were gently retracted using Allis clamps. The cystic capsule was noted to be very thin. The entire cyst was completely shelled out, using sharp dissection using Iris scissors and electrocautery, and blunt dissection (Figure 5b). The entire cyst sac was sent to pathology. (Figure 5c) for the entirely excised cystic mass. Excellent hemostasis was reassured from the surgical site. The base was irrigated using sterile water. The dead space was closed in multiple interrupted or hyperextend at the hips and knees, using Allen stirrups. The Bair hugger was placed to maintain control of core body temperature. The intraoperative physical exam revealed the clitoral mass with atrophic surrounding tissue (Figure 3). The possible dorsal nerve of clitoris and perineal nerve pathways were mapped using a marker pen (Figure 4), per Wu C, et al. [6] General anesthesia with a laryngeal mask airway was induced without difficulty. She was then prepped and draped in the normal sterile fashion. A foley was inserted in a sterile fashion.
stitches using # 4-0 reabsorbable suture. The clitoral hood was reconstructed using # 3-0 reabsorbable suture in multiple interrupted stitches. A urinary Foley catheter was removed, and cystoscopy was performed using a 70-degree scope with sterile water as a distention medium. Normal findings were noted in the bladder and urethra except for atrophic mucosa and mild glomerulation. The cystoscope was removed under direct visualization and the bladder was emptied. All instruments were removed from the surgical field and the patient was placed in a supine position. In’s and out’s were noted. All needles, laps, and instrument counts were correct x3. The patient was extubated and was taken to the recovery room in stable awake condition. In the recovery unit, the patient was able to void successfully after the urinary catheter removal and went home the same day without any issues.



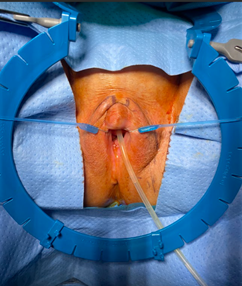
Figure 5a: Longstar retractor placement Figure 5b: Shelling out the cystic mass Figure 5c: Excised entire cystic mass.


Figure 6a: 2 weeks postoperative state Figure 6b: 6 weeks postoperative state Figure 6: Postoperative Photos after clitoral cystic mass excision and clitoral hood reconstruction At 6 weeks postoperative visit, the patient recovered well and was very satisfied with surgical outcome. Normal anatomy of clitoris/clitoral hoods were noted with normal sensual sensation in/around the clitoris. The patient resumed sexual intercourse without issues. See Figure 6b for the final presentation.
Figure 7a (magnification 100x) Figure 7b (magnification 400x)
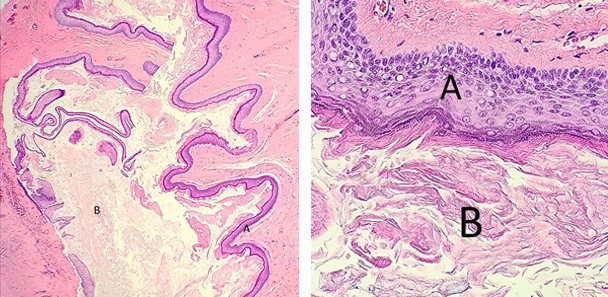
A: Stratified squamous epithelium lining, B: Loose keratin flakes
Discussion
Although it is rare, it is not uncommon to encounter clitoral inclusion cysts with history of local trauma or genital mutilation, especially in the under developing countries [1, 2, 3, 4, 5]. However, it is not common to have spontaneous clitoral inclusion cysts in the absence of trauma or genital mutilation [5].
A variety of cysts/masses can be found in the female genital area, with or without symptoms. Clinicians should be able to differentiate between clitoral cysts/masses and clitoromegaly, which may be due to hormonal causes. Although a clinical exam can be sufficient in differentiating the cyst/mass from clitoromegaly, imaging (i.e. MRI) may be warranted to evaluate the characteristics of the cyst/mass, before planning surgical excision.
A variety of cystic masses can occur in female external genitalia which may be vaginal, paraurethral, vulvar or clitoral. Clitoral masses are uncommon but can be benign or malignant. Benign tumors include leiomyoma, pseudo-lymphoma, fibroma, angiokeratoma, hemangioma, hemangiopericytoma, granular cell tumor, and neurofibroma. Malignant tumors reported include endodermal sinus tumor, carcinoma, sarcoma, schwannoma, lymphoma, rhabdomyosarcoma, epithelioid hemangioendothelioma, or rarely secondary metastasis [4].
Besides the patient’s request for a cosmetic reason, the patient in this case report underwent surgical excision to ensure the non-malignant nature of the clitoral mass, considering her history of anal cancer and radiation therapy. It is important to counsel the patient before surgical management about the possible surgical impact on sexual function, undesired cosmesis, recurrent urinary tract infection, clitoral scarring, psychological impact, and recurrence. To minimize damaging the dorsal nerve of clitoris, perioperative sensory mapping could be also considered to perform [6].
Declaration of Patient Consent
The author certifies that she had obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published, and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial Support and Sponsorship
Nil.
Acknowledgement
The author would like to thank Cassandra Simpson, DO at Inspira Network OBGYN residency program, and Ashley Lentini, MD, Department of Pathology at Inspira Medical Center, Vineland, NJ for helping to obtain the pathology slides.
Conflicts of Interest
There are no conflicts of interest.
References
-
Ibrahimi A, Kallat A (2021) Epidermoid cyst of the clitoris. Pan Afr Med J 38: 59.
-
Prasad I, Sinha S, Bharti S, Singh J, Dureja S (2022) Epidermal Inclusion Cyst of the Clitoris: A Case Report. Cureus 14(9): e29066.
-
DiCarlo-Meacham AM, Dengler KL, Snitchler AN, Gruber DD (2020) Clitoral Epidermal Inclusion Cyst Leading to Anorgasmia: A Case Report and Literature Review. J Pediatr Adolesc Gynecol 33(3): 321-323.
-
Rouzi A, Sindi O, Facharzt BR, Ba’aqeel H (2001) Epidermal clitoral inclusion cyst after type I female genital mutilation. Am J Obstet Gynecol 185: 569-571.
-
Rouzi AA (2010) Epidermal clitoral inclusion cysts: not a rare complication of female genital mutilation. Hum Reprod 25(7): 1672-1674.
-
Wu C, Damitz L, Karrat KM, Mintz A, Zolnoun D (2016) Clitoral Epidermal Inclusion Cyst Resection with Intraoperative Sensory Nerve Mapping Technique. Female Pelvic Med Reconstr Surg 22(3): e24-e26.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’