Association of Maternal Serum Gamma-Glutamyltransfetase Level at First Trimester as a Predictive Biomaker of Gestational Diabetes Mellitus
Introduction: The prevalence of GDM is increasing globally. GDM is associated with many maternal and fetal complications. Hence identifying and treating maternal hyperglycemia is beneficial for both mother and baby. Proper monitoring of women is necessary during pre-conceptional and early pregnancy period to prevent GDM and its complication. Objective: To assess the level of maternal serum Gamma-glutamyltransferase (GGT) as predictor of Gestational Diabetes Mellitus (GDM). Methods: A Prospective cohort study was carried out at Department of Obstetrics and Gynaecology, Dhaka Medical College Hospital, Dhaka from January 2021 to December 2021. Total sample size was 144. Pregnant women attending Obstetric OPD, DMCH at her 1st trimester (8 -12 weeks) without the evidence of GDM, DM, or any comorbid condition and drugs that affects blood glucose level. Data regarding demographic profile, medical and family history (history of chronic hypertension, diabetes mellitus, autoimmune disease, and CKD) were recorded. Obstetric history regarding gravity, parity, past obstetric history was documented. Then a complete physical examination of the subjects including height, weight, blood pressure level was carried out with an appropriate procedure. Period of the gestation was confirmed by recording CRL in early USG. Patient’s fasting blood sugar and 2hrs after 75- gram glucose at first trimester was measured. Results: In the current study 144 pregnant women, at their first trimester (8-12 week) were included, but during follow up about 12 patients were dropped out due to mid trimester abortion, migration to another place and so on. Most of them were primi (56.1%) housewife (75%), had completed their secondary education (59.1%), and about 61.4% belong to middle class family. The clinical parameter like BMI 25.80±4.56kg/m2, gestational age at delivery 38.09±1.28 weeks. The mean ±SD BMI 27.52±4.72 kg/m in GDM group 25.40±4.46 kg/m in Non GDM group. The mean ± SD birth weight was 3.07±0.37 kg in GDM group and 2.86±0.33 in Non GDM group. The difference was statistically non- significant (p>0.05) between two groups. Among 45.45% subjects had GGT level <10 U/L,34.09% had 11-20 U/L and 20.45% had GGT >20 U/L. Among total 132 respondents 25 respondents (18.94%) developed GDM. The total population divided in two groups, Group I (GDM) and Group II (non GDM). Shows that in group A (GGT ≥12.5 U/L) total respondents were 61, GDM developed in 29.50% (n=18), GDM not developed in 70.49% (n=43). On the Other hand in Group B (GGT <12.5 U/L) total respondents were 71, GDM developed in 9.85% (n=07) and GDM not developed in 90.14% (n=64) and p value was 0.004. Conclusion: The result of our study indicated that pregnant women with high GGT (>12.5 U/L) at booking visit had greater risk of developing GDM (72%).Sensitivity, Specificity, PPV ,NPV of this diagnostic test was 72% , 59.81%, 29.50%, 90.14% respectively and accuracy is 94.69%. Among these 132 respondents, those having GGT>12.5IU/L relative risk (RR) of development of GDM is 3.01. As measurement of GGT is easy, inexpensive and easy to carry out, it can be used as a predictive biomarker who are at increased risk for the subsequent development of GDM.
Introduction
Diabetes is the most common metabolic complications of pregnancy. The prevalence of GDM increasing globally because of obesity and sedentary work. About 3 to 25 % of total pregnancies are affected by GDM, mainly attributed to advanced maternal age and the rising prevalence of obesity [1, 2]. Prevalence of GDM varies significantly among different populations, ethnicities as well as with diagnostic criteria. Some population-based studies conducted in Bangladesh at different time points have revealed an increasing trend of GDM prevalence ranging from 6% to 14% [3]. Hyperglycaemia first detected at any time during pregnancy should be classified as either gestational diabetes (GDM) or diabetes mellitus in pregnancy. This condition usually returns to normal after pregnancy and those who have persistence glucose intolerance will develop type 2 Diabetes Mellitus (DM) [4]. GDM threatens the life of gestational women, fetuses and newborns and often give rise to pregnancy complications such as macrosomia, polyhydramnios, gestational hypertension and neonatal complications and adverse perinatal outcomes and increase risk of development of type 2 DM in both mother and her children [5]. Pregnancy is characterized by increase in insulin resistance and decrease in insulin sensitivity which is counteracted by compensatory hyperinsulinaemia. A pregnant woman who is not able to increase her insulin secretion to overcome the insulin resistance, develop GDM. Both insulin resistance and β cell dysfunction exist in individual who develop GDM [6]. Different studies suggest that oxidative stress plays an important role in the physiology of GDM [7]. In order to increase the effectiveness of early prenatal prediction for GDM a number of serum biomarkers have been reported that could be used in combination with data from maternal characteristics and medical history. These biomarkers are either markers of placentation [Pregnancy Associated Plasma Protein A (PAPP-A), and placental growth factor (PlGF)] or inflammatory markers (C-reactive protein, tumor necrosis factor-α) organ derived markers (gamma glutamyltransferase, adiponectin). The current approach of diagnosis and treatment during the late second or early third trimester of pregnancy fails to prevent the pathology that is already well established and the adverse effects on long term outcomes [8]. If an effective first trimester predictor tests were available, the damage accumulated during the clinically occult phase (before 24-28 weeks) may be avoided by early intervention, such as nutritional counseling, guided exercise [9] or even pharmacological therapy eg Metformin [10]. There are ample evidences that increased gamma glutamyltransferase level is a risk factor for the development of Metabolic Syndrome, impaired glucose tolerance and type 2 DM [11]. GGT is useful to predict the development of type 2 diabetes mellitus [12]. GGT levels have been reported to be correlated with insulin sensitivity. So, we aimed to find out the relation between GGT level in early pregnancy and development of GDM.
Materials and Methods
Study design: Prospective cohort study Study Place: Department of Obstetrics and Gynaecology, Dhaka Medical College Hospital, Dhaka. Period of study: January 2021 to December 2021. Study population: Pregnant women attending Obstetric OPD, DMCH at her 1st trimester (8 -12 weeks) without the evidence of GDM, DM, or any comorbid condition and drugs that affects blood glucose level Sample size: So, total sample size was 144.
Inclusion Criteria
- Pregnant women at first trimester (8-12 weeks) of pregnancy attending in obstetric OPD, DMCH who were agreed to participate, recruited in the study.
- Age between 18 and 35 years of age.
- Singleton pregnancy
- Informed consent for inclusion in the study.
Exclusion Criteria
- Known diabetic or diagnosed at first trimester.
- H/O GDM in last pregnancy
- Family H/O DM.
- Obese BMI>35 kg /m2.
- Women with systemic disease (HTN, Collagen Vascular Disease, Heart Disease, Renal disease, Chronic liver disease)
- H/o taking Alcohol and some drugs that affects GGT (phenytoin, Phenobarbital, Acetaminophen, OCP)
- Fetal abnormalities, as the possibility that those patients might have option for a pregnancy termination existed and data collection would thus be incomplete.
- Pregnancy with extreme of age (<18 years, >35 years)
Study procedure
Pregnant women, attending the outpatient department of DMCH for routine ANC, who fulfilled the mentioned selection criteria, were selected by purposive convenience sampling. The purpose and procedure of the study was discussed with them individually. After obtaining informed consent the women were interviewed by the researcher herself for the purpose of collection of data. Data regarding demographic profile, medical and family history (history of chronic hypertension, diabetes mellitus, autoimmune disease, and CKD) were recorded. Obstetric history regarding gravity, parity, past obstetric history was documented. Then a complete physical examination of the subjects including height, weight, blood pressure level was carried out with an appropriate procedure. Period of the gestation was confirmed by recording CRL in early USG. Patient’s fasting blood sugar and 2hrs after 75- gram glucose at first trimester was measured. An additional 3 ml of blood was draw in conjunction of FBS sample to measure GGT. Then the blood was allowed to clot, and serum was separated by centrifugation at room temperature for 20 minutes at the speed of 2000-3000 r.p.m. The laboratory of Biochemistry and Molecular Biology Dept. used Siemens Atellica solution version 1.25.1.4163001 analyzer machine for GGT analysis. This test was conducted at Department of Biochemistry and Molecular Biology, BSMMU. The participants were followed up at each visit they were clinically evaluated. At 24 – 28 weeks blood was collected for OGTT. If it is found normal, then repeat OGTT was done at 32-36 weeks. WHO criteria for diagnosis of GDM is FBS 5.1-6.9 mmol/L, 2hrs after 75gm glucose plasma glucose level 8.5 – 11.0 mmol/L. If GDM developed, then patient should be followed up two weekly or more frequently if needed. All collected data were shown and discussed with the respective guide weekly for feedback and necessary correction before implementation. Analysis and write up was shared with the guide as well. Statistical analysis was done by statistician.
Data analysis
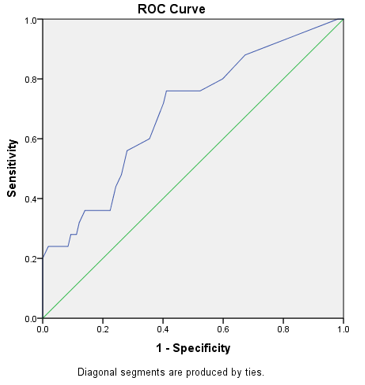
Collected data were kept in a master sheet followed by entry for back up support in excel, after initial editing & cleaning the furnished data were transferred for statistical analysis into SPSS for Windows (IBM SPSS Statistics for Windows, version 25.0, Armonk, NY: IBM Corp.) software. For analyses, results were presented as mean ± standard deviation (SD) for quantitative variables and as absolute frequencies and percentages for categorical variables. Comparison was done by Chi-Squared (X2) test and unpaired t – test where necessary. A probability p value of <0.05 considered statistically significant. Area under ROC (Receiver Operator Curve) used to find the predictive values of GGT for GDM. Negative predictive value was calculated along with sensitivity and specificity.
Results
In the current study 144 pregnant women, at their first trimester (8-12 week) were included, but during follow up about 12 patients were dropped out due to mid trimester abortion, migration to another place and so on. The findings derived from the data analysis are given below:
| Characteristics | Number of Patients | Percentages % |
|---|---|---|
| Age Category | ||
| < 20 | 24 | 18.2 |
| 21 – 30 | 85 | 64.4 |
| >30 | 23 | 17.4 |
| Parity | ||
| 0 | 74 | 56.1 |
| 1 | 41 | 31.1 |
| 2 | 14 | 10.6 |
| 3 | 3 | 2.3 |
| Occupation | ||
| Housewife | 99 | 75 |
| Working | 33 | 25 |
| Educational Status | ||
| Illiterate | 1 | 0.8 |
| Only can sign her name | 9 | 6.8 |
| Primary education | 44 | 33.3 |
| Secondary education and above | 78 | 59.1 |
| Socioeconomic status | ||
| Lower | 28 | 21.2 |
| Middle | 81 | 61.4 |
| Upper | 23 | 17.4 |
Table 1: Demographical distribution of the study population (N=132).
Table 1 shows the general characteristics of study subjects. Most of them were primi (56.1%) housewife (75%), had completed their secondary education (59.1%), and about 61.4% belong to middle class family.
| Characteristics | Mean ± Standard Deviation | Range |
|---|---|---|
| Weight (Kg) | 60.31 ± 10.27 | 38 –88 |
| Height (m) | 1.53 ± 0.09 | 1.24 - 1.68 |
| 2 BMI (kg/m ) | 25.80 ± 4.56 | 18.41 – 34.34 |
| CRL at booking (mm) | 51.32 ± 10.4 | 36 – 77 |
| GGT (U/L) (at 8-12 weeks) | ||
| <10 | 7.47 ± 1.28 | 2- 10 |
| 11-20 | 14.31 ± 2.65 | 11 – 20 |
| >21 | 26.89 ± 5.30 | 21 – 42 |
| Gestational age at delivery (weeks) | 38.09 ± 1.28 | 34 – 40 |
Table 2: Distribution of clinical parameter of study population (N=132).
Table 2 shows mean and SD of clinical parameter like BMI 25.80±4.56kg/m2, gestational age at delivery 38.09±1.28 weeks.
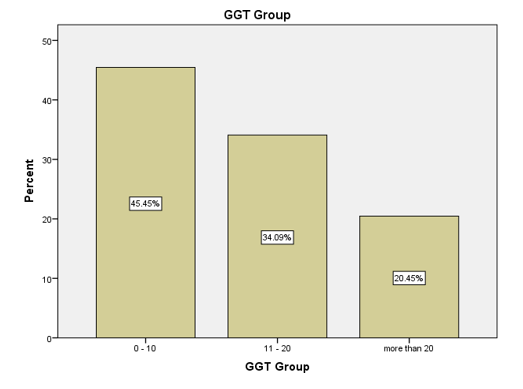
(Figure 1) shows about 45.45% subjects had GGT level <10 U/L,34.09% had 11-20 U/L and 20.45% had GGT >20 U/L.
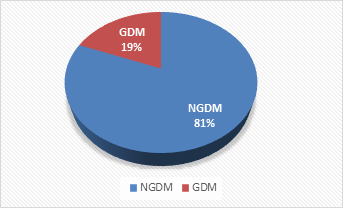
Figure 2 shows that among total 132 respondents 25 respondents (18.94%) developed GDM. The total population divided in two groups, Group I (GDM) and Group II (non GDM).
| Characteristics | GDM Group In =25 | Non GDM G roup II n=107 | P-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| 2 BMI (kg/m ) | 27.52 ± 4.72 | 25.40 ± 4.46 | 0.217 |
| Range (Min, Max) | (20.40, 34.24) | (16.41, 33.29) | |
| Gestational age at delivery | 38.00 ± 1.44 | 38.11 ± 1.24 | 0.296 |
| Range (Min, Max) | (34, 40) | (34, 40) | |
| Birth Weight | 3.07 ± 0.37 | 2.86 ± 0.33 | 0.118 |
| Range (Min, Max) | (2.1, 3.9) | (2.1, 3.8) |
Table 3: Maternal factor& pregnancy outcome of GDM and non GDM. P value reached from unpaired t-test.
The mean ±SD BMI 27.52±4.72 kg/m in GDM group 25.40±4.46 kg/m in Non GDM group. The mean ± SD birth weight was 3.07±0.37 kg in GDM group and 2.86±0.33 in Non
GDM group. The difference was statistically non- significant (p>0.05) between two groups.
| Characteristics | Group IG DM n= 25 | Group II Non GDM n=107 | Total | P-Value | ||
|---|---|---|---|---|---|---|
| n | % | n | % | 0.004 | ||
| Group A | ||||||
| GGT ≥12.5 U/L | 18 | 29.50% | 43 | 70.49% | 61 | |
| Group B | ||||||
| GGT<12.5U/L | 07 | 9.85% | 64 | 90.14% | 71 | |
| Total | 25 | 107 | 132 |
Table 4: Association of development of GDM with serum GGT at cut off value 12.5 U/L. Chi square test was done to measure the leve
Table 4 shows that in group A (GGT ≥12.5 U/L) total respondents were 61, GDM developed in 29.50% (n=18), GDM not developed in 70.49% (n=43). On the Other hand in Group B (GGT <12.5 U/L) total respondents were 71, GDM developed in 9.85% (n=07) and GDM not developed in 90.14% (n=64) and p value was 0.004 .
| Screening Test | Group I GDM | Group II Non GDM | Total |
|---|---|---|---|
| Group A | |||
| GGT ≥ 12.5 | 18 (a) | 43(b) | 61 (a + b) |
| Group B | |||
| GGT< 12.5 | 7 (c) | 64 (d) | 71 (c + d) |
| Total | 25 (a + c) | 107 (b + d) | 132 (a + b + c + d) |
| Value | 95% CI | ||
| Sensitivity | 72% | 66.2 % to 78.13 % | |
| Specificity | 59.81% | 52.80 % to 66.72 % | |
| Positive Predictive value | 29.50% | 23.67 % to 36.31 % | |
| Negative Predictive value | 90.14% | 84.60 % to 95.73 % | |
| Accuracy | 94.69% | 88.65 % to 96.07 % |
Table 5: Sensitivity, specificity, PPV and NPV of serum GGT in prediction of GDM (N=132).
| Screening Test | Group I GDM | Group II Non GDM | Total | RR |
|---|---|---|---|---|
| Group A | ||||
| GGT≥12.5 | 18 (a) | 43(b) | 61 (a + b) | |
| Group B | 3.01* | |||
| GGT<12.5 | 07 (c) | 64(d) | 71 (c + d) | |
| Total | 25 (a + c) | 107 (b + d) | 132 (a + b + c + d) |
Table 6: Relative Risk (RR) of development of GDM with GGT≥12.5 U/L and GGT level <12.5 U/L (N=132). *RR shows strong relation Ta
Discussion
This prospective cohort study was done to find out the association of maternal serum gamma- glutamyltransferase (GGT) level at first trimester as a predictive biomarker of gestational diabetes mellitus (GDM). A total number of 144 patients were included in this study from obstetrics and fetomaternal medicine outpatient department of Dhaka medical college hospital, Dhaka. Meanwhile twelve (12) patients among them dropped out due to abortion, migration, non-compliance and so on. So, this study was carried out on 132 women with viable pregnancy after fulfilling all the inclusion criteria and exclusion criteria. The demographic characteristics of the study subjects shown in Table 1. Most
of the respondents were primi (56.1%) housewife (75%), had completed their secondary education (59.1%), and about 61.4% belonged to middle class family. The GGT level range for LFT is 5 – 27 U/L in reproductive age of female population. Most of the population in our study had GGT level below 10 U/L. In our study GGT level was performed at 8-12 weeks of pregnancy. About 45.45% subjects had GGT level <10 U/L, 34.09% had 11-20 U/L and 20.45% had GGT level >20 U/L. Then these participants followed up monthly according to standard ANC. Tan PC; Aziz AZ; Ismail IS in 2012 [13] conducted a study regarding GGT, ALT, AST level and the diagnosis of GDM in University of Malaya and showed GGT level has been increase with the age (>35.8 years) and BMI (>35.2 kg/m2). In our study Most of the respondents (85%) were from 20-30 years of age as well as regarding BMI median value was 25.85±4.56. In this study we restricted inclusion age above 35 years and BMI above 35kg/m2. So, the influence of confounding factors were limited. Nanda S, et al. [14] in King College Hospital, UK conducted a study, Prediction of GDM by maternal factors and biomarkers at 11 to 13 weeks, where they demonstrated that after Logistic regression in prediction of GDM there were significant contribution from maternal age, BMI, racial origin, previous history of GDM and delivery of macrosomia neonates. In my study maternal mean weight at booking in group I (63.59±8.02) was higher than mean weight of group II (59.54±10.62), mean BMI of group I (27.52±4.72) was greater than group II (25.40±4.46). But all these differences are not statistically significant as (p>0.05) in two group comparison. Many studies have reported that pre-coceptional BMI, obesity, adverse pregnancy outcome, parity are associated with higher prevalence of GDM and independent risk factors of GDM [11, 15, 16, 17]. In this study, mean (±SD) of BMI was 27.52±4.72 kg/m2 in group I and 25.40±4.46kg/m2 in group II. So, BMI was higher in GDM group than non GDM group. Sneha BS [5] in Diabetes care show BMI were 26.00±6.5kg/m2 in GDM group and 23.7±4.6kg/m2 in non GDM group, which is consistent with the current study. Among these 132 populations we did OGTT at their 24-28 weeks of pregnancy and 32-36 weeks of pregnancy. We found 25 (18.94%) patients were developed GDM which categorized by WHO criteria of GDM diagnosis. These patients labeled as Group I GDM n=25 (18.94%) Group II non GDM n=107 (8 1.06%). In this current study Box plot (median, interquartile range and range) of GGT level to non GDM and GDM populations shows clearly that the median value of GGT level was increased in GDM group in comparison with non GDM group. Correa PJ, et al. [18] conducted a case control study regarding First trimester prediction of GDM using plasma biomarker where others plasma biomarker including GGT showed increased median value in GDM group. In this study ROC curve of GGT level showed that Area under Curve (AUC) of GGT level is 0.689, 95% CI (0.572- 0.806). Optimum predictive value was calculated from the coordinates of the curve table. According to Youden Index the best cutoff value was 12.5 U/L with sensitivity 72% (95% CI 66.2%-78.13%) and specificity 59.81% (95% CI 52.80%-66.72%), PPV 29.50%, NPV 90.14% and Accuracy 94.69%. Gulhane Military Medical faculty, Turkey, Alanbay I, et al. [11] calculated predictive GGT level for GDM from ROC curve. When GGT cut off was set at 10 U/L the sensitivity was 86% and specificity 37% were found. Alanbay I, et al. [11] in their study showed GGT threshold was found as 16 U/L with performing ROC analysis. Considering predictive value of GGT level the study population divided into two group. Group A ≥12.5 U/L (n=61) and group B <12.5 U/L(n=71). Rao JP, Jayakantrhan RV [19] showed correlation between S.GGT level and GDM. In this study, GDM rate was 12% whereas worldwide incidence varied from 3% to 25% and among the GDM group, 16% had low GGT and 84% had high GGT. Similarly In our study group GDM rate was 18.94% (n=25) having 72% (n=18) high GGT and 28% (n=07) had normal GGT level. This association showed GDM were significantly higher among group A (GGT>12.5 U/L) with P value .004. In this study Relative Risk (RR) of development of GDM in group A (GGT ≥12.5 U/L) was 3.01, which showed strong positive association. Tan PC, et al. [13] in China did a study regarding GGT and diagnosis of GDM and found RR was 1.35. In the time of turning the pyramid of obstetric care, early screening of GDM with timely intervention is desirable. Early disease identification may reduce the adverse fetal and maternal consequences of that disease. Detection of GGT level is cost effective easily available test so that easily could be used as a first trimester predictor. Women at risk for GDM identified in first trimester of pregnancy could follow the lifestyle modifications earlier than usual pregnancy. Large scale prospective study involving diverse group of population are warranted to clarify the association between first trimester GGT level and development of GDM.
Conclusion
The result of our study indicated that pregnant women with high GGT (>12.5 U/L) at booking visit had greater risk of developing GDM (72%).Sensitivity, Specificity, PPV ,NPV of this diagnostic test was 72% , 59.81%, 29.50%, 90.14% respectively and accuracy is 94.69%. Among these 132 respondents, those having GGT>12.5IU/L relative risk (RR) of development of GDM is 3.01. As measurement of GGT is easy, inexpensive and easy to carry out, it can be used as a predictive biomarker who are at increased risk for the subsequent development of GDM.
Limitations
Like other studies the present study was also not flawless. Although optimum care has been tried by the researcher in every step of this study, some limitations still exist: • Limited sample size was a major limitation.
- The data of the study collected from DMCH only; therefore, there might be an issue of generalization of the study findings. The result of the study might not be reflecting the exact picture of the country.
- The present study was conducted at a very short period of time.
Recommendations
Further studies on a large scale are recommended for the well establishment of the fact that GGT in maternal serum at first trimester is a good predictor for diagnosis of GDM. So that, people like ours can get the benefit of this low cost, easily available and user-friendly biomarker.
Awareness should be developed among obstetricians towards prediction and early intervention of pregnancy complication by using different biomarkers.
References
-
Vandorsten JP, Dodson WC, Espeland MA, Grobman WA, Guise J M, et al. (20130 NIH consensus development conference: diagnosing gestational diabetes mellitus. NIH Consens State Sci Statements 29(1): 1-31.
-
Zhao D, Shen L, Wei Y, Xie J, Chen S, et al. (2017) Identification of candidate biomarkers for the prediction of gestational diabetes mellitus in the early stages of pregnancy using iTRAQ quantitative proteomics. Proteomics Clinical applications 11(7-8).
-
Jesmin S, Akter S, Akashi H, Al-Mamun A, Rahman MA, et al. (2014) Screening for gestational diabetes mellitus and its prevalence in Bangladesh. Diabetes research and clinical practice 103(1): 57-62.
-
Moore TR, Mouzon SH, Catalano P (2014) Diabetes in pregnancy. In: Creasy RK, Resnik R, Iams JD, Lockwook CJ, Moore TR, Green MF, editors. 2014 CREASY & RESNIK’S Maternal-fetal Medicine. 8th(Edn.), Philadelphia: Elsevier, pp: 988-1021.
-
Sridhar SB, Xu F, Darbinian J, Quesenberry CP, Ferrara A, et al. (2014) Pregravid liver enzyme levels and risk of gestational diabetes mellitus during a subsequent pregnancy. Diabetes Care 37(7): 1878-1884.
-
Moore TR, Mouzon SH, Catalano P. Diabetes in pregnancy. In: Creasy RK, Resnik R, Iams JD, Lockwook CJ, Moore TR, Green MF, editors. 2014 CREASY & RESNIK’S Maternal- fetal Medicine. 8th (Edn.), Philadelphia: Elsevier, pp: 988- 1021.
-
Lappas M, Hiden U, Desoye G, Froehlich J, Hauguel-de Mouzon S, et al. (2011) The role of oxidative stress in the pathophysiology of gestational diabetes mellitus. Antioxidants & redox signaling 15(12): 3061-3100.
-
Monteiro LJ, Norman JE, Rice GE, Illanes SE (20160 Fetal programming and gestational diabetes mellitus. Placenta 48(1): S54-S60.
-
Simmons D, Devlieger R, van Assche A, Jans G, Galjaard S, et al. (2017) Effect of Physical Activity and/or Healthy Eating on GDM Risk: The DALI Lifestyle Study. The Journal of clinical endocrinology and metabolism 102(3): 903-913.
-
Ainuddin JA, Karim N, Zaheer S, Ali SS, Hasan AA (2015) Metformin treatment in type 2 diabetes in pregnancy: an active controlled, parallel-group, randomized, open label study in patients with type 2 diabetes in pregnancy. Journal of diabetes research 2015: 325851.
-
Alanbay I, Coksuer H, Ercan M, Keskin U, Karasahin K, et al. (2012) Can serum gamma-glutamyltransferase levels be useful at diagnosing gestational diabetes mellitus?. Gynecological endocrinology 28(3): 208-211.
-
Gautier A, Balkau B, Lange C, Tichet J, Bonnet F, et al. (2010) Risk factors for incident type 2 diabetes in individuals with a BMI of <27 kg/m2: the role of gamma- glutamyltransferase. Data from an Epidemiological Study on the Insulin Resistance Syndrome (DESIR). Diabetologia 53(2): 247-253.
-
Tan PC, Aziz AZ, Ismail IS, Omar SZ (2012) Gamma- glutamyltransferase, alanine transaminase and aspartate transaminase levels and the diagnosis of gestational diabetes mellitus. Clinical biochemistry 45(15): 1192- 1196.
-
Nanda S, Savvidou M, Syngelaki A, Akolekar R, Nicolaides KH (2011) Prediction of gestational diabetes mellitus by maternal factors and biomarkers at 11 to 13 weeks. Prenatal diagnosis 31(2): 135-141.
-
Khalil NA, Fathy WM, Mahmoud NS (2017) Screening for Gestational Diabetes Among Pregnant Women Attending a Rural Family Health Center- Menoufia Governorate- Egypt. Journal of Family Medicine and Health Care 3(1): 6-11.
-
Zhu WW, Yang HX, Wang C, Su RN, Feng H, et al. (2017) High Prevalence of Gestational Diabetes Mellitus in Beijing: Effect of Maternal Birth Weight and Other Risk Factors. Chinese medical journal 130(9): 1019-1025.
-
Kong M, Liu C, Guo Y, Gao Q, Zhong C, et al. (2018) Higher level of GGT during mid pregnancy is associated with increased risk of gestational diabetes mellitus. Clinical endocrinology 88(5): 700-705.
-
Correa PJ, Venegas P, Palmeiro Y, Albers D, Rice G, et al. (2019) First trimester prediction of gestational diabetes mellitus using plasma biomarkers: a case-control study. Journal of perinatal medicine 47(2): 161-168.
-
Jyothi R, Rajini V (2019) Correlation between serum gamma glutamyl transferase and gestational diabetes mellitus in pregnancy. Journal of Evidence Based Medicine and Healthcare 6(9): 650-652.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’