A Study of the Registrar Review Clinic of Cheltenham
Medical practise is about innovation, invention and discovery. The Registrar Review Clinic (RRC) was set up to reduce pressures in other department where obstetrics and Gynaecological patients are seen, especially in the out-patient clinics where patients wait for months before been seen in the Gynaecological Out-Patient Department (GOPD) or wait for hours before been seen in other busy units like the Accident and Emergency, Early Pregnancy and Fetal Assessment Clinic (EPAC), Gynaecology Wards, etc. It is a fast-track clinic for benign non-emergency cases so that patients are attended to faster and earlier, and appropriate referral made quicker or earlier if that is the appropriate course of action. The experience of Cheltenham General Hospital in 2007 was studied and analysed in this study performed in 2008 and is now presented.
Abbreviations
TAH-Total Abdominal Hysterectomy; RSO-Right Salpingo-Oophorectomy; BSO-Bilateral Salpingo- Oophorectomy Respectively; CEA-Carcino-Embryonic Antigen; BHCG-Beta Human Chorionic Gonadotrophin; LIF and RIF-Left and Right Iliac Fossa Respectively; RPOC- Retained Products Of Conception; IUCD-Intrauterine Contraceptive Device; DNA-Did Not Attend; NAD-Nothing abnormal discovered: HVS/LVS-High And Low Vaginal Swab Respectively; ERPC-Evacuation of Retained Products of Conceptions; A&E-Accident and Emergency CA-125-Carcinoma Antigen 125.
Introduction
This is essentially a review rather than an audit. RRC in the Obstetrics and Gynaecology department of the Cheltenham General Hospital (CGH) of Gloucestershire Hospital NHS Foundation Trust was started essentially to bridge the gaps between A&E, EPAC and Gynaecological Wards. The purposed of setting up this unit was to cut down emergency in-patient admissions and to reduce the breaches of the four hour Waiting Rule by A&E patients. Patients are attended to, reviewed and investigated. They may be discharged; followed-up; referred to other units or even admitted. The RRC started in September 2004. The clinic had operated three times a week but the present version of the clinic started in September 2006 and had operated every day from Monday to Friday. It draws its population of patients from mainly General Practitioners (GP), A&E, Wards, etc. Patients are attended to between 14:00 to 16:00 hours with one scan slot at 15:20 only. The total daily attendance slots for patients to be attended to are 5 commencing at 14:00 hours. The average number of patients seen daily is 2. The scan slot at 15:20 each of the weekdays on many occasions are usually taken up by patients from EPAU or Wards if there was no patient for RRC clinic requiring a scan. The RRC keeps a register where patients are booked from GP or other units and this is reviewed daily Monday to Friday by the Gynaecology- on-call team for the evening (pm) shift. At the end of the day, the attending staff writes a summary of the consultation of each patient to his/her GP. The attending staff who attend to patient at the RRC are Senior House Officer (SHO), Nurse Practitioner (NP), Registrars and Consultants, with similar communication hierarchy when needed as seen in other types of patient care delivery system or network.
Aim/objectives
To review of its role of the RRC in the overall dispensation of patients’ care. To review its impact in the overall chain and network of patients’ care at this unit for which it is only a part off. This impact is largely in reducing the pressures in other Units and GOPD’s waiting list.
Materials and Methods
The diary of the RRC for 2007 was reviewed and considered during the study. I then studied the proforma of the RRC review in June 2005(RRC Review, 2005). From the old proforma, we designed a more expansive, elaborate and up-to-date proforma which was used in this study. I studied the Early Pregnancy Assessment Clinic audit of March 2003 (EPAC audit, 2005) to assess how the EPAC works and how it relates to other Units including RRC in the overall dispensation of patients care delivery. This newly prepared up-to-date study proforma contained appropriate patient’s personal and demographic data. 245 case notes were identified and this constitutes the target population for this study. This was followed by a systematic review of 50 case notes out of 245, twice, to ensure accuracy and consistency in the data collated. The 50 case notes were selected at random without any element of bias. These 50 case notes constitute the study population for this review. Literature search was extensive and this included the following: typing “invested clinics” on Google search, did not yield significant information. However, typing “innovative clinics” on Google search, yielded the study from Bolton Hospital UK (Royal Bolton General Out patient Audit, 2010), while typing on Google search “new clinics bridging the gaps,” yielded infusion clinics in Canada (Kashyap M, 2007 and Heart Failure Clinic of Texas USA (Christus Hospital News, 2013), among others.
Results/findings
Number of patients/attendance for the year 2007 was 245. This 245 constitute the target population of this study.
| Attendance | |
|---|---|
| January | 15 |
| February | 19 |
| March | 23 |
| April | 18 |
| May | 29* |
| June | 35* |
| July | 20 |
| August | 21 |
| September | 13 |
| October | 20 |
| November | 18 |
| December | 14 |
Table 1: Target Population.
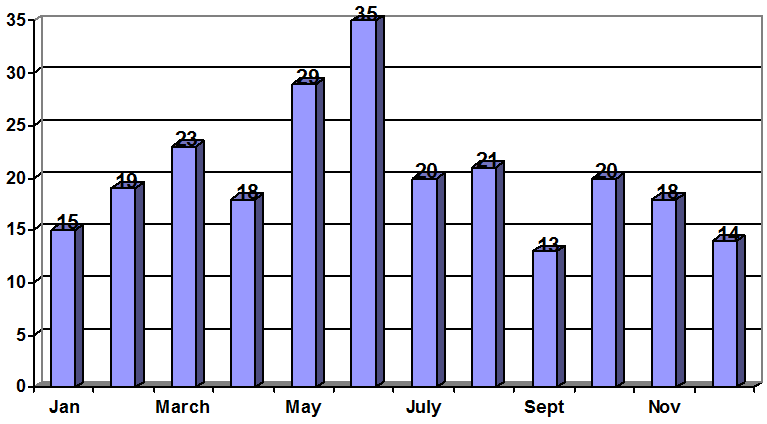
Graph 1: Target Population.
Hospital Admissions 2005 –2007
| Emergency | 2005 | 2006 | 2007 | |||
| Emergency | Admissions | A&E attends | Admissions | A&E attends | Admissions | A&E attends* |
| Emergency | 555 | 548 | 606 | |||
| Elective | Inpatients | 620 | 601 | 624 | ||
| Day cases | 1185 | 1181 | 1280 | |||
| TOTAL | 2360 | 557 | 2330 | 589 | 2510 | 630 |
Table 2: Hospital Admissions 2005 –2007.
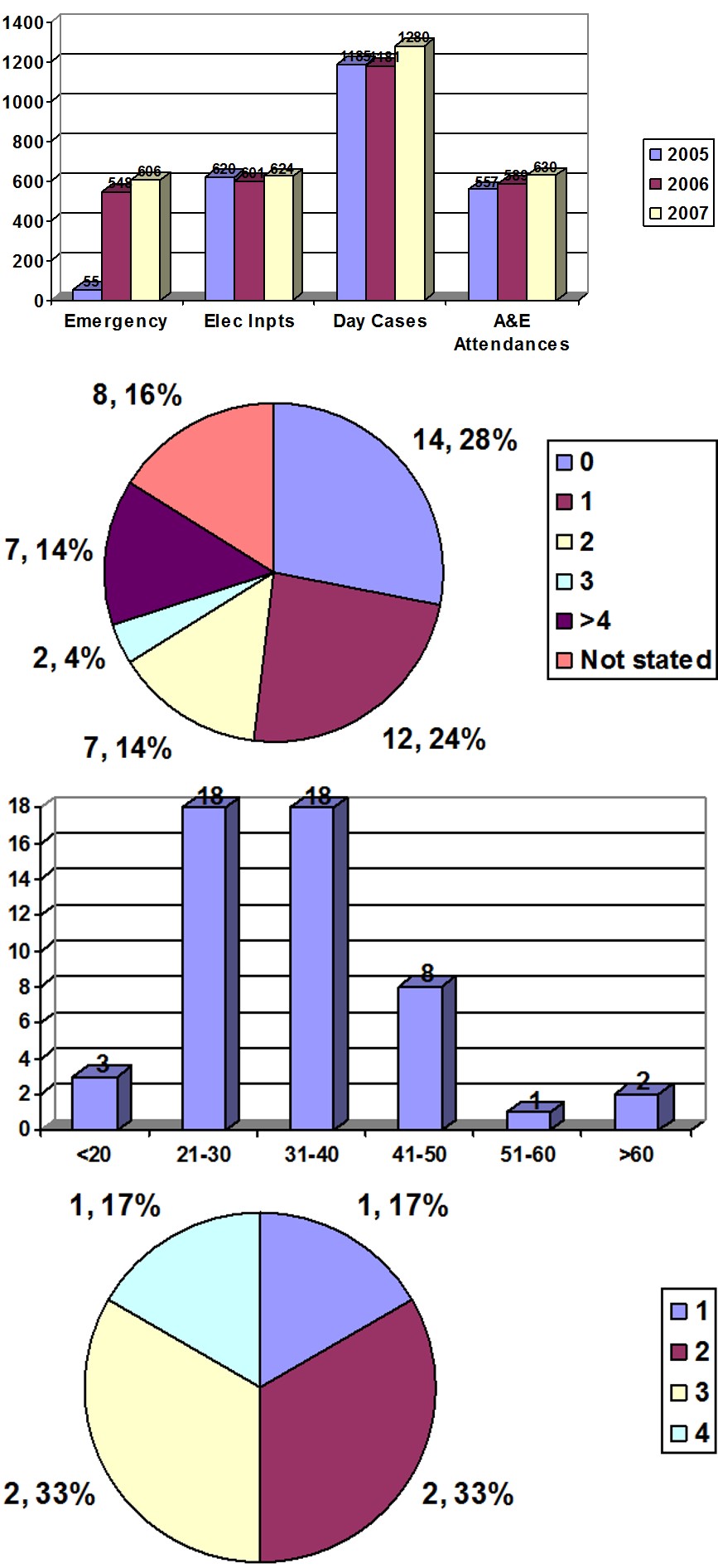
Graph 2: Hospital Admissions 2005 –2007.
| Age group | Number of patients |
|---|---|
| <20 | 3 |
| 21-30 | 18* |
| 31-40 | 18* |
| 41-50 | 8 |
| 51-60 | 1 |
| >60 | 2 |
Graph 3: Age Group.
| Number of patients | |
|---|---|
| 0 | 14* |
| 1 | 12 |
| 2 | 7 |
| 3 | 2 |
| >4 | 7 |
| Not stated | 8 |
Graph 4: Parity.
| 51-60 | 1 |
| >60 | 2 |
Graph 5: Gravidity (If Pregnant).
| PV bleeding in early pregnancy | 18* |
|---|---|
| Abdominal pain/cramps/LIF/RIF | 20* |
| Ectopic/early pregnancy | 7 |
| Menorrhagia/menstrual problems | 1 |
| Sore/swollen vulva | 2 |
| Hydrosalpinx | 1 |
| Feeling unwell | 2 |
| Perineal boils/groin/labial abscess | 4 |
| Early pregnancy/missed period | 1 |
| PV discharge | 1 |
| Ovarian cyst | 2 |
| Groin pain | 1 |
| Constipation | 1 |
| Bartholin’s abscess | 2 |
| Post TAH/BSO/RSO problems | 2 |
| Post op follow up | 1 |
| Shelf pessary fell off | 1 |
| GP | 26* |
| A&E | 18* |
| Wards | 5 |
| EPAC | 1 |
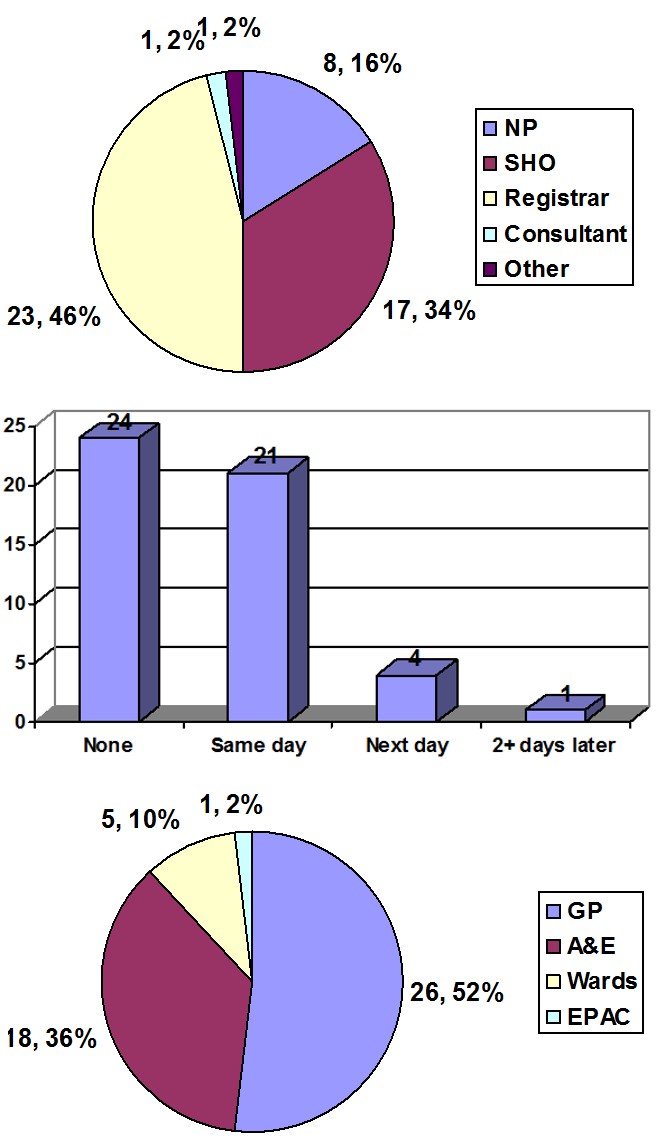
Graph 7: Sources of Referral.
| NP | 8 |
|---|---|
| SHO | 17* |
| Registrar | 23* |
| Consultant | 1 |
| Other staff | 1 |
| Low bhcg | 1 |
| Pregnancy test positive | 2 |
| Negative pregnancy test | 4 |
| Scan NAD | 1 |
| Ectopic pregnancy | 1 |
| Per vaginal(PV) bleeding | 6 |
| Cystocele/2nd degree utero-vaginal prolapse | 1 |
| No shelf pessary seen | 1 |
| Rising bhcg | 2 |
| Fibroid in pregnancy | 1 |
| No PV bleeding | 1 |
| Pelvic mass | 1 |
| Previous cyst not seen | 1 |
| IUCD in situ | 1 |
| Abscess | 2 |
| wound infection | 2 |
| Mass in the fundus | 1 |
| Tender right groin | 2 |
| Coil related problem | 1 |
| Fibroid uterus | 2 |
| Thick endometrium | 1 |
| Urinary Tract infection | 3 |
| RPOC on scan | 1 |
| Tender RIF/LIF | 4 |
| Cervical polyp | 1 |
| Intrauterine pregnancy | 1 |
| PV bleeding | 2 |
| Resolving Bartholin’s | 2 |
| Resolving vault haematoma | 1 |
| Tender epigastrium | 1 |
| Polycystic ovarian syndrome | 1 |
| Vulva granulation tissue | 1 |
| No RPOC on scan | 4 |
Table 10: Attended by Groups.
Graph 8: Attended by Groups.
| Scan | Number of patient | |
|---|---|---|
| Groin pain | 1 | |
| Constipation | 1 | |
| Bartholin’s abscess | 2 | |
| Post TAH/BSO/RSO problems | 2 | |
| Post op follow up | 1 | |
| Shelf pessary fell off | 1 |
Graph 9: Scan Performed.
| Full blood count | 16 |
|---|---|
| HVS/LVS | 4 |
| Bhcg | 3 |
| CEA | 1 |
| Group &Save | 7 |
| Pregnancy test | 4 |
| Urea& Electrolyte | 4 |
| urinalysis | 4 |
| Liver Function Test | 2 |
| CA-125 | 1 |
| Midstream Urine | 3 |
| Blood cultures | 1 |
| Stool analysis | 1 |
| Wound swab | 1 |
| C- reactive protein | 4 |
Table 9: Other Investigations.
| Counselling/reassurance/discharge | 13* |
| Ferrous sulphate | 2 |
| antibiotics | 6 |
| Mefenamic/tranexamic acid | 4 |
| Combined pill | 2 |
| Pain relief | 3 |
| Follow up RRCeg Rev clinic+/- scan,+/- bhcg | 7 |
| Insert shelf pessary | 1 |
| Add on operation list | 1 |
| Buscopan | 1 |
| ERPC | 2 |
| Follow up + oral Feso4 | 1 |
| Remove suture | 1 |
| Ring pessary | 1 |
| Incision & Drainage | 2 |
| GOPD follow up +/- scan | 7 |
| Pregnancy Test | 1 |
| Continue on POP | 1 |
| Low bhcg | 1 | Phone patient with plan | 1 |
| Pregnancy test positive | 2 | Remove suture | 1 |
| Negative pregnancy test | 4 | Admit for treatment | 1 |
| Scan NAD | 1 | Marsupialization | 1 |
| Ectopic pregnancy | 1 | Increases fluid intake | 1 |
| Per vaginal(PV) bleeding | 6 | Try another pill | 1 |
| Cystocele/2nd degree utero-vaginal prolapse | 1 | Lactulose | 1 |
| No shelf pessary seen | 1 |
| Fibroid in pregnancy | 1 | Yes | No |
| No PV bleeding | 1 | 6* | 44 |
| Pelvic mass | 1 |
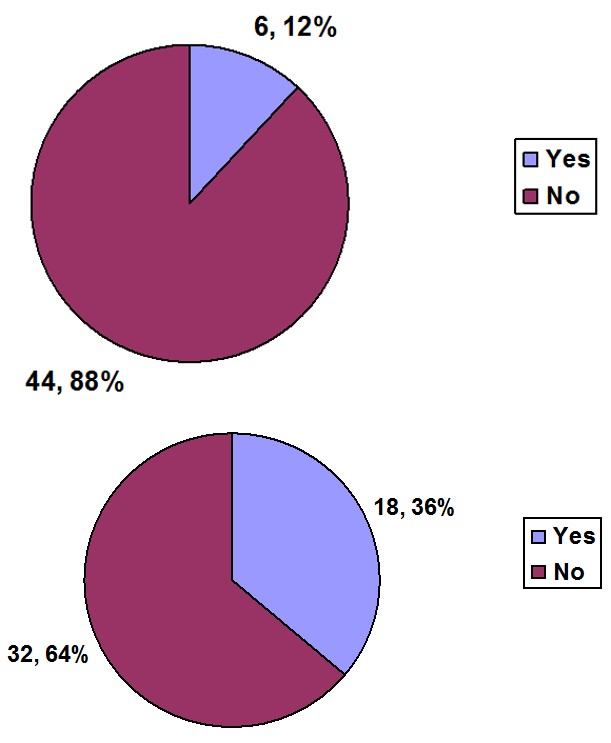
| Yes | No |
|---|---|
| 6* | 44 |
Table 12: A&E Involved Some Point.
| Out of hours | Not out of hours | Self-referral | Mode of referral not stated |
| 8 | 42 | 12 | 2 |
Table 15: EPAC and Gynaecological Wards.
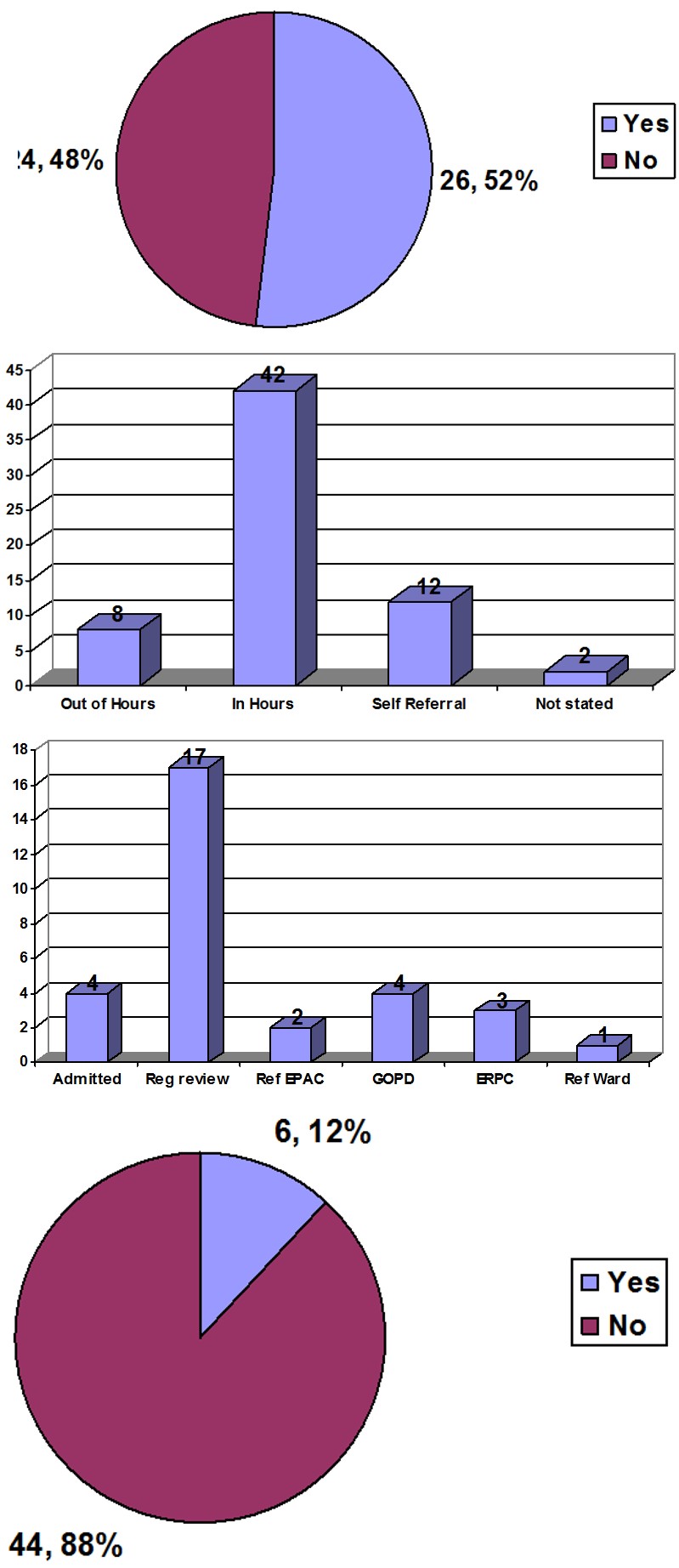
Graph 15: EPAC and Gynaecological Wards.
| es | No |
| 6* | 44 |
Graph 16: Admitted.
| I &D | 1 |
| Unwell | 1 |
| Observation | 1 |
| ERPC | 1 |
| Marsupialisation | 1 |
| Laparoscopy | 1 |
Table 19: Reasons for Admission.
| Yes | No/discharge to GP |
| 26 | 24 |
Graph 18: Follow-Up/Referral/Admitted.
| Admitted | 4* |
| RRC follow-up | 17* |
| Referrer to EPAC | 2 |
| GOPD | 4 |
| Evacuation of Retained Products of Conception | 3 |
| Refer to the Ward | 1 |
Table 16: Outcome of first visit.
Graph 19: Outcome of first visit.
| Discharged | 24* |
|---|---|
| GOPD | 7 |
| Admitted | 6 |
| Refer to ward | 1 |
| GP follow up | 1 |
| Evacuation of retained products of conception | 3 |
| DNA follow up | 3 |
| Antenatal Clinic | 1 |
| Emergency Operation list | 2 |
| Laparoscopy | 1 |
| Future operation/surgery | 1 |
| Follow-up | 11 |
Table 18: Overall Outcome.
| Yes | No |
| 1 | 49 |
Table 21: Referred to Other Specialties.
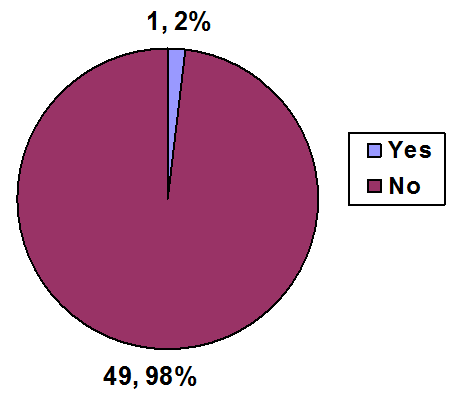
Graph 21: Referred to Other Specialties.
Discussion and Comparisms
This study was more detailed than the first review of June 2005 (Sundar SS, Smith L, Clark F, and Reddy K). A total of 178 patients were seen in RRC, according to Sundar SS et al. According to this review, the RRC helped prevent impatient admissions in 73 patients. However, the author was not able to reproduce exactly how this was achieved. For the year 2007, the RRC attended to 245 patients (target population), out of which 18 patients out of 50 (study population) were referred from the A&E. Thus about 88.2(18x245/50) patients (36%) would have been seen in A&E for the year 2007. The highest attendance was in June 2007 (35 patients) and next was in May 2007(29 patients). The author was not able to find out the reason for this. Most of the patients attended were in the age groups 21-30 and 31-40. Most of the patients are nulliparous; 14 of the study population (50) and 68.6 of the target population (245) which is 28%.
The most common complaint from the patients was lower abdominal pain followed by bleeding PV/PV bleeding in early pregnancy. The commonest source of referral was from GPs (26/50), or 127.4 of the target population (52%), followed by A&E (18/50), which is 28% of the study or target population. Most patients were attended to by Registrars (23/50) or 46% of the study or target population. Most patients did not have scan (24/50), while 21/50 had scan. Most patients only needed counselling and reassurance (13/50), 26%. 6/50 had other teams involved in their care and 6/50 appeared to have been admitted for justifiable reasons. 24/50 were discharged, 117.6 of the target population or 46% while 17/50, 83.3 of the target population or 34%, had follow-ups/seen more than once in RRC. The A&E saw a total of 630 patients for 2007. These patients would have been seen in the overbooked GOPD or busy and overstretched A&E unit. Current trend after this study; In 2010, Royal Bolton Hospital staff (Royal Bolton General Outpatient Audit, 2010) had a perception that the workload capacity of outpatient clinics was being pushed to overloading and the team wanted to know why. They wanted to ensure that outpatient departments were offering the safest and highest possible quality care to their patients. A team then conducted an audit of its general outpatient clinics aimed at understanding the barriers preventing a smooth process of appointment booking and treatment. The key areas identified were: Patient wait time; they needed to reduce new patient waiting times for appointment. Poorly managed clinic lists and appointment bookings; there was observation that clinic appointments were under utilised and overbooked. Double booking appointments; their booking system failed to capture changes properly to highlight unwanted appointments. This led to gaps and the notion that patients were not attending.
Case note management; different ways of looking after case notes led to delays, duplicated information gathering and created dissatisfaction for patients and staff. By addressing these issues, the staff aimed to eliminate waste within the system and improve productivity to see more patients sooner and safer. Some highlights from their study were as follows: Better outpatient bookings; changes to how staff handled cancellations reduced rework from 1,004 hours per month to 141 hours per month. Improving use of appointment vacancies; use of general surgery slots improved by 45%, well above the initial target of 15%. Centralising outpatient case notes; a new process for storing and preparing notes centrally released the equivalent of 90 hours per week of band 2 times. The team and hospital, after initial audit and later a subsequent one, embarked on a one-year cycle of improvement, which spanned from April 2010 until March 2011. The author argues, that this lengthy, labour intensive and complicated approach to the problems can be done in a simpler, perhaps more efficient and cost effective way by initiating a more specialized innovative clinic like the Gynaecology RRC of Cheltenham, to deal with the whole problems in the General Out Patient Department. A similar but different scenario was played out in Canada (NE oncology issue, 2007), where due to inherent delays and lengthy and complex bureaucratic processes, newer drugs such as nanoparticle albumin-bound (NAB) paclitaxel3 that have been approved by Health Canada and clinical practice guidelines for breast cancer treatment could take anywhere from 6 to 24 months to gain government funding approval. This led to the establishment of innovative Infusion Clinics to bridge the gaps. Christus Hospital in South East Texas St. Elizabeth (Christus Hospital News, 2013), found out that it was falling through the care gap and embarked on the establishment of a new Heart Failure clinic to bridge the gap and deal with the following; administering and reviewing laboratory work and results, providing consultations with a registered dietician, making medication adjustments and offering varied educational seminars on heart healthy nutrition, spiritual care and stress management. This innovative clinic also serves as a community resource for those with heart failure. In a year, from November 2012, its inception, to October 2013, it guided patients through the care process, helping patients learn and understand their disease. It also attended to 100 patients with heart failure with greater care and success.
Documentation
In the case notes studied, there were errors and omissions in documentation found during the study, and the author are of the view that these errors have medico- legal significance. In the patients’ register: Patents were recorded with single name, or as first name only, some were stated as simply; “a lady” or “one lady”. There were names with no dates of birth, wrong dates of birth and wrong hospital numbers making it very difficult to trace their case notes. Again, the author is of the view that these errors have medico-legal significance and accordingly recommends a careful, accurate, thorough and detailed documentation.
Recommendations
- Documentations should be improved in the patients’ case note to include good history and demographics. Also brief basic details of patients’ personal and demographic data should be put in the booking register namely; names, hospital number (if available), date of birth, main complaint and other helpful and relevant clinical information.
- Leaflet given to patient/GPs briefly and simply explaining what the clinic is all about and what it does.
- Poster in the clinic briefly explaining to patients that they may have to wait for a while before been attended to because of the nature of the clinic.
- To assist to proper concise clinical documentation the author had drafted a provisional form with basic patients’ personal and demographic data that may assist the unit and the department. The consultants would normally approve it before putting it into clinical use.
- The Unit to conduct a review in 2 years and compare with this and previous study.
Summary
It is clear that the 245 patients in 2007 seen and properly reviewed in the RRC could have been seen or attended to at other Units like GOPD, EPAC and A&E. Thus, it is sensibly and logical to infer that while the RRC has reduced pressures on other units it also provides opportunities for learning, training and research.
References
-
Sundar SS, Smith L, Clark F, Reddy K (2005) Registrar Review Clinic Review Cheltenham General Hospital, Gloucestershire NHS Foundation Trust, Cheltenham, Gloucestershire, UK.
-
EPAC Audit (2003) Cheltenham General Hospital Gloucestershire NHS Foundation Trust, Cheltenham, Gloucestershire, UK.
-
Royal Bolton General Outpatient Audit (2010) Innovation to Improve Efficiency; The Health Foundation.
-
Kashyap Meenakshi (2007) Infusion Clinics Bridge the gap: NE Oncology issue, New Evidence.
-
Christus Hospital News (2013) Christus Hospital Southeast Texas St Elizabeth, Texas USA.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’