Testicle Evanescent in Pediatric Urology: Laparoscopic Management
Testicular regression syndrome or evanescent testis is a clinical condition that arises from atrophy and disappearance of normal testis in the fetal period. Anatomically it is characterized by a spermatic cord with no identifiable macroscopically testicular tissue. The absence of a testicle in a man 46XY is usually unilateral and arises from a twist or an intrauterine or perinatal stroke. The clinical case of male 2 years 6 months old, a product of the second pregnancy, which comes to evaluation, is presented cryptorchidism left. On physical examination, genital according to age and sex, good gonadal development, normal penis and foreskin, right testicle in scrotal sac, about 12 mm, left no palpable. It inguino-escrotal ultrasound with left empty scrotal sac, no left testicle, right scrotal sac with normal testicle is identified. MRI was performed showing only right testicle in the scrotum. Diagnostic laparoscopy was performed, finding in the groin area on the right side the path of vas deferens normally and gonadal vessels of good caliber in the inguinal ring, on the left side, vas deferens was found dead-end and absence of gonadal vessels and the inguinal ring closed. Laparoscopy is the most effective and most widely accepted for non-palpable testicle therapeutic diagnostic method because it provides access to the abdominal cavity and high visibility, with the known advantages of laparoscopy in terms of postoperative recovery, also applicable to pediatric patients.
Introduction
Testicular regression syndrome or evanescent testis is a clinical condition that arises atrophy and disappearance in the fetal testis normal period [1]. The presence of cord structures is evidence of presence of the testis in early fetal life. When associated with a blind spermatic cord, this entity is called evanescent testicle syndrome in urological literature; anatomically it is characterized by a spermatic cord with no identifiable macroscopically testicular tissue [2]. The absence of a testicle in a man
46XY is usually unilateral and arises from a twist or an intrauterine or perinatal infarction [3]. Testicular regression syndrome occurs in less than 5% of cases of cryptorchidism, it is not a common condition. In non- palpable testes testis evanescent occurs in 35% to 60% of cases. A review of the Children's Hospital of Philadelphia on non-palpable testes showed that 41% (187) of 447 children had remaining atrophic or testicular absence, so we can deduce that is a common phenomenon that is not diagnosed and therefore it is rarely treated. Etiology and pathophysiology: Hormonal and mechanical factors have been implicated in testicular descent, but so far there is no specific factor that has been clearly identified in the pathogenesis of non-palpable testes syndrome, testicular regression has been explained as a result of thrombosis, torsion or endocrine disease, recent studies strongly support a vascular accident or antenatal torsion on the endocrine disease, as undescended testes completely tend to be more prone to twisting during fetal and perinatal period [4]. This hypothesis is supported by the presence of hemosiderin-laden macrophages and venous congestion and myocardial bleeding secondary to torsion. On the other hand evanescent patients with unilateral testicular germ cells show less or some suggestive condition endocrinopathy- in the undescended testicle [4]. Testicular regression was observed in association with genetic abnormalities such as chromosome microdeletions and has been found persistence of Müllerian structures subsequent birth in children with evanescent testicle. In addition, the early loss of both testicles cause genital ambiguity, yet the association of genetic factors necessary for testicular descent, anorchidism and evanescent testicle have not been well established. In most cases the evanescent testis tends to be sporadic and occurs in patients with familial history or not. And recently reports have been found in association with other defects including mental retardation in chromosomally normal siblings or several members of the same family, suggesting a genetic basis in some patients [5]. Clinical manifestations of evanescent testicle may be associated with embryological sequence and can be classified as early and late fetal and early middle and late neonatal embryo. It may be unilateral or bilateral less frequently, with partial or complete absence of testicular tissue and in most cases with normal external genitalia. Patients are usually male phenotype; the spectrum can range from normal male unilateral non-palpable cases with micropenis phenotypically male to female or phenotypically [6, 7]. The phenotype likely to depend on the extent and timing of intrauterine accident. On the other hand the evanescent testicle of embryonic origin has been considered clinical part of the 46XY gonadal dysgenesis, in association with micropenis and uni- or bilateral crypthorquidism. The degree of genital masculinization depends on the length of testicular function to its evanescence [8]. Have reported some degree of sexual ambiguity in familial cases has recently been found a heterozygous loss (V355M) in the SF1 gene in a patient with testicular evanescent.
Clinical Case
Male patient 2 years 6 months old, a product of the second pregnancy, a mother of 34, healthy, father of 38 years with rheumatoid arthritis, normal pregnancy, obtained via vaginal delivery, birth weight 2900 g, height 46 cm; history of sporadic infections upper airways. Go to valuation cryptorchidism left. On physical examination, genital according to age and sex, good gonadal development, normal penis and foreskin, right testicle in scrotal sac, about 0.5 cm, non-palpable left. Ultrasound was performed inguinoescrotal where left empty scrotal sac is observed, no left testicle; right scrotal sac with testis (Figure 1) is identified.
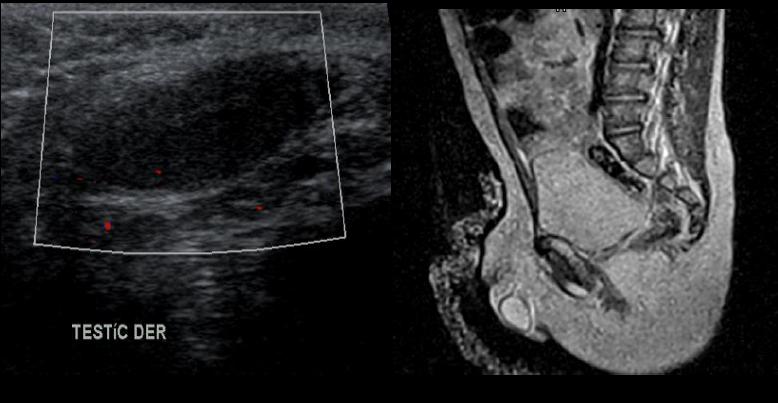
MRI was performed showing only right testicle in the scrotum (Figure 2).
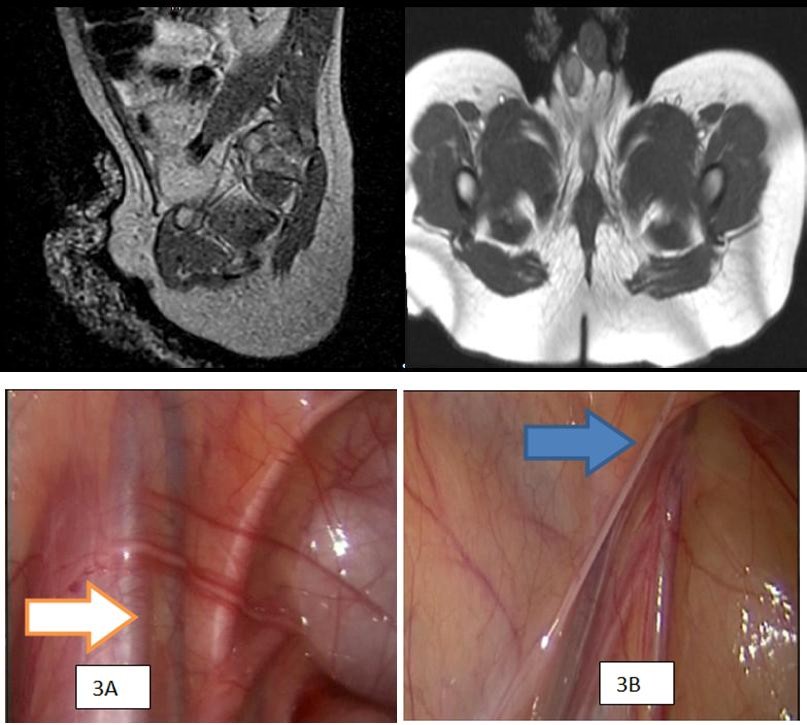
Figure 2: IRM with absence of the left testicle (arrow) 2B) Inguinal region with absence left testicle. It was decided to perform diagnostic and therapeutic laparoscopy no palpable and visible imaging in left testicle. The surgery was performed under general anesthesia in the operating room. The patient was prepared with nasogastric and urinary catheter. The pneumoperitoneum with carbon dioxide is performed using the open technique with Hasson technique, with intraperitoneal introduction of a 5 mm port under direct vision with minimal incision of the umbilical region. Intraabdominal CO2 pressure was 12 mm Hg or less for the trocar placement. Through this umbilical port 5 mm lens attached to a camera and vision is performed on the video monitor it was introduced. Constituted the first step in the exploration of the peritoneal cavity, and then video- laparoscopic under control, two 5-mm ports for instrumentation on each side at the level of the mid- clavicular line were introduced. the anatomical references, such as lateral bladder ligaments, iliac vessels, also the right side he found the path of the vas deferens normally and gonadal vessels of good quality in the inguinal ring (Figure 3A) were found, across the left side, the closed inguinal ring (Figure 3B) vas deferens was found dead-end and absence of gonadal vessels, as well.
Figure 3A: Right spermatic cord is visible the confluence of the deferent cordon and gonadal vessels. Figure 3B: Left inguinal region which no gonal vessels are appreciated.
The left vas deferens is flashed, and the trocars were removed under direct vision. The operative time was 28 minutes, the bleeding was minimal, there were no complications during the procedure or early or late postoperative.
Discussion
The non-palpable testicle when associated to the lack of testis is known as evanescent testis or testicular regression syndrome, which is characterized by partial or total absence of testicular, unilateral or bilateral tissue with or without epididymis or cord structures in a patient 46 XY. Laparoscopic surgical exploration is the method of choice today, as it allows orchidopexy when feasible or to resect the remaining. We report the case of a pediatric patient wherein the therapeutic diagnostic approach for non-palpable testicle testicle proved to be aevancescente where only the blind vas deferens was found in the absence of testicular tissue. There is a high risk of malignant transformation in intra-abdominal testicles, especially when associated with abnormal external genitalia and chromosomal abnormalities. A testicular tumor may appear after a orchidopexy, however today it is unclear risk with evanescent testicles. On the one hand, it is true that shares the same pathophysiology and risks that cryptorchidism, however the controversy is focused on the waste and remnants of testicular germ tissue, since theoretically indicate a potential long-term malignancy. Found viable germ cells from 0% to 16% in different series, based on this, some authors removed the remains routinely but others do not accept this indication because no testicular tissue remnants found in a large percentage [9]. Clinically unilateral non-palpable testes can be associated with evanescent testicles, cryptorchidism, retractile testes with testicular agenesis or. Laparoscopy has been widely used to distinguish these conditions over open surgery [10]. Laparoscopy and minimally invasive surgical method was introduced as a screening method in children in the early years of the 1970s by Steven Gans. In childhood age does not limit the application of laparoscopy because now it has opticians, trocars and surgical material from 1.7 mm in diameter and can be performed even in neonates. In the pediatric use of laparoscopy as an exploratory procedure it is highly profitable and in some cases irreplaceable [6, 10]. The main advantages of laparoscopic surgery described are the early postoperative recovery by minimizing postoperative pain, less restriction on postoperative activities, in some cases the most aesthetic scar and other better visualization of the operative field. When a testis is not palpable, the vas deferens and the spermatic vessels are visualized out of the internal inguinal ring and when only remnants are found, they can be removed. Several series report ranges from 90%to 95% non-palpable location laparoscopic testis. There are some criteria that have been proposed for the accurate diagnosis of evanescent testicle. 1) Testis not palpable during examination under anesthesia, 2) Viewing blind spermatic vessels and terminals, without displaying deferential vessels and spermatic vessels, 3) glasses deferential blind with closed internal inguinal ring. Therefore inguinal exploration requires only if the internal inguinal ring is open laparoscopy, but does not require further exploration if they are hypoplastic vessels and closed inguinal ring.
Conclusion
The evanescent testicle represents a diagnostic challenge variable incidence or even unknown. Minimally invasive surgery is an effective alternative in pediatric patients if performed in hospitals with experience, where you have all the necessary human and material resources. Laparoscopy is the most effective and most widely accepted for non-palpable testicle diagnostic therapeutic modality, as it provides access to the abdominal cavity and high visibility, with the known advantages in terms of postoperative recovery, also applicable to pediatric patients.
References
-
Sheikh A, Mirza B, Ahmad S, Ijaz L, Kayastha K, et al. (2015) Laparoscopic management of undescended testes 128: Our experience. Afr J Paediatr Surg 9(2): 106-108.
-
Park K, Hwang Choi (2010) An Evolution of orchiopexy: Historical Aspect. Korean J Urol 51(3): 155-160.
-
Lopez PJ, Angel LG, Rodríguez HJ, Reyes CD, Scale AJM, et al. (2009) Laparoscopy in nonpalpable testicle. Rev Chil Paediatr 80(3): 225-230.
-
Antic T, Hyjek EM, Taxy JB (2011) The Vanishing Testis. A histomorphologic and Clinical Assessment. Am J Clin Pathol 136(6): 872-880.
-
Shalaby M (2015) Is there a role for open surgery in the management of the undescended testis?. Afr J Paediatr Surg 9(2): 97-100.
-
Shalaby M, Shoma A, Elanany F, Elganainy E, El-Akkad MA (2011) Management of the looping vas deferens looping During laparoscopic orchiopexy. J Urol 185(6): 2455-2457.
-
Vipul G, Yadav SK, Dean E, Vincent P, Walid F, et al. (2013) Paediatric laparoscopic orchidopexy as a novel laparoscopic mentorship: Training model. Afr J Paediatr Surg 10(2): 117-121.
-
EITayeb A (2009) The unilateral impalpable testis: does the order of the procedure Affect the outcome? Ann Surg Pediatric 5: 115-118.
-
Pirgon O, Bumin Nuri Dündar (2012) Vanishing Testes: A Literature Review. J Clin Endocrinol Pediatr Res 4(3): 116-120.
-
Hrivatakis G, Wolfgang Astfalk, Andreas Schmidt, Andreas Hartwig, Thomas Kugler, et al. (2014) The Timing of Surgery for Undescended Testis A retrospective multicenter analysis. Dtsch Arztebl Int 111: 649-657.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report