Synchronized Bilteral Testicular Plasmocitoma Contribution of a Case and Literature Review
Monroy-Galvez A*, Serrano-Ortega E, Cerda-Guerrero E and Guadarrama Vallejo C
Urology Department UMAE N.14, National Medical Center, Lic Adolfo Ruiz Cortines,
IMSS, Veracruz, México
Ruiz Cortines, IMSS, Veracruz, México, Email: albertomonroy55@hotmail.com Keywords: Testicular; Parenchyma; Seminoma; Plasmacytoma
Introduction
Testicular plasmacytoma accounts for less than 2% of all plasma cell neoplasms; this is usually an autopsy finding, although it may sometimes be a manifestation of multiple myeloma and more rarely is its unique location. Only 3 cases of synchronous bilateral testicular involvement by plasmacytoma have been published in the literature. The prognosis of testicular plasmacytoma depends largely on whether or not it associates with multiple myeloma. In the latter case, the majority of patients presents progression of the disease and dies as a result of the tumor. Treatment includes orchiectomy, radio and / or chemotherapy; however the best treatment has not yet been established.
Clinical Case
A 46-year-old male patient from Orizaba, Veracruz, diagnosed with multiple myeloma type Bence-Jones, stage III-A in 2009, treated with VAD (Vincristine, Adriamycin and Dexamethasone), with adequate evolution. In 2014 it presents progressive and painless increase of both testicles, in predominance of the left side, of two months of evolution reason why it was sent to the consultation of urology. In the physical examination we can see the left testicle with a regular volume increase, with irregular thickening of the spermatic cord that does not allow to distinguish its structures, accompanied by hydrocele. The right testicle also increased in size and consistency, with no other alterations. Testicular tumor markers showed normal values: LDH: 111 IU (240-280) Alpha-fetoprotein: 1.7 ng / ml. Beta-HCG: <1.20 mIU / ml. Testicular ultrasound reported an increase in left testicular size with a longitudinal axis of 55 mm and of 36 mm. of the right testicle. (Figure 1 and 2) Left testicle accompanied by hydrocele. Both testicular parenchyma have a heterogeneous echo graphic structure, with a brindled and irregular appearance. In the Doppler study, a significant increase in vascularization was observed in both testicular parenchymas (Figure 3).
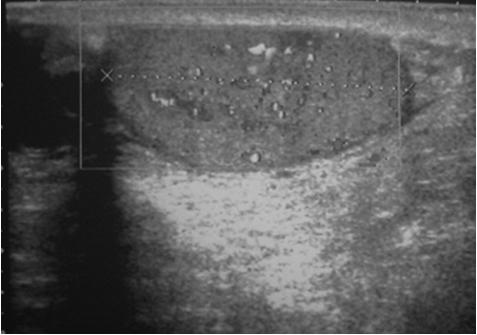

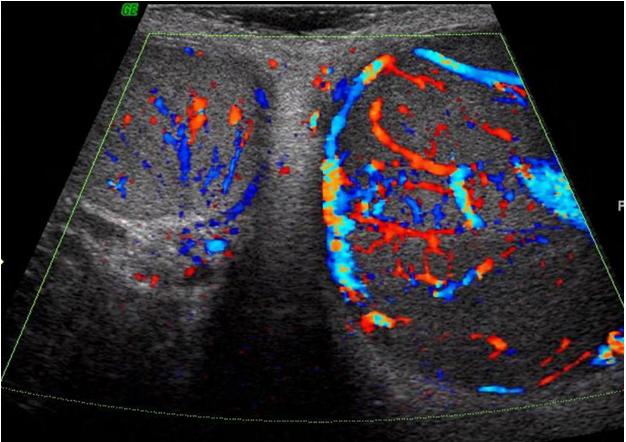
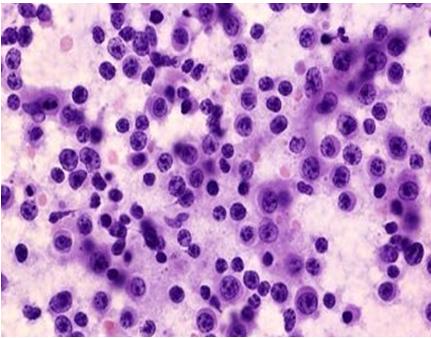
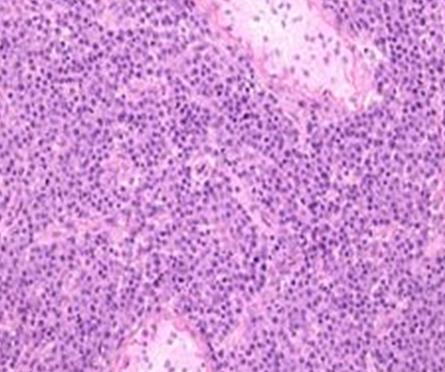
Figure 3: Both testicular parenchyma. It was decided to perform bilateral orchiectomy with a report of pathology: a piece of orchiectomy weighed 55g on the left side and 25g on the right side, with a homogeneous tumor, brownish gray and soft, the tumor contacted with albuginea, without surpassing it, and accompanied by a serohematic hydrocele at the left-side. With bilateral testicular infiltration by neoplastic cells, with testicular parenchyma effacement due to the presence of a diffuse proliferation of plasma cells (eccentric nucleus, amphiphilic cytoplasm, cartilage nucleus) (Figure 4 and 5) Spermatic cord.
Discussion
Multiple myeloma is a disease characterized by aberrant production and excretion of homogeneous monoclonal proteins by a group of neoplastic plasma cells. This cell group originally proliferates in the bone marrow, subsequently invading the adjacent bone with progressive generalized skeletal involvement. Due to favorable conditions in some cases neoplastic plasma cells are present in extra-skeletal locations, then referred to as extramedullary plasmacytoma [1].
Plasmacytoma is a plasma cell tumor that affects the bone marrow or extramedullary sites. Testicular plasmacytoma was first described in 1939 and since then a little more than 60 cases have been described in the literature [2, 3]. Testicular plasmacytoma cases have been described in patients between 26 and 89 years of age, with a mean age of 56, 5 years [4]. Only 3 cases of bilateral bilateral testicular involvement with plasmacytoma have been published in the literature [5]. It presents an incidence range of 0.03% to 0.1% of all primary and secondary tumors affecting the testis. Among patients with multiple myeloma, the incidence of plasmacytoma affecting the testis is 0.6% to 2.7% of the total [6, 7]. In autopsy studies of patients with myeloma, extramedullary involvement of up to 65-70% has been observed [8]. Extramedullary plasmacytomas affecting the testis are extremely rare, with an incidence of 2% in all cases of plasma cell neoplasms [9]. Solitary plasmacytoma is a rare entity and represents only 6% of all plasma cell neoplasms [10, 11]. Testicular plasmacytoma is usually presented as an autopsy finding that lacks clinical expression, although in some cases it may constitute a manifestation of a multiple myeloma and more uniquely be its unique location. There is rarely a clinically evident testicular enlargement, being exceptional that supposes the first manifestation of the disease. There is only testicular involvement in 2.7% of multiple myelomas with extra-medullary manifestations [12]. In half of the cases of testicular myeloma there is a previous history of plasma cell neoplasia [13]. It affects the testicular parenchyma, although occasionally it may also appear in the epididymis. It presents with painless swelling and has occasionally been described with associated hydrocele [12]. Ultrasonographically there is no specific ultrasound pattern to define the type of testicular tumor. The grayscale sonographic pattern in the testicular plasmacytoma has been shown to be homogeneous or heterogeneous, and primarily hypoechoic. When marked hypervascularity occurs in a patient with an improbable picture of orchitis, plasmacytoma should be considered as a differential diagnosis [7]. The most common differential diagnosis is with seminoma, particularly the spermatocytic variant and with lymphomas. However, the relative cellular monomorphism, together with the plasma-cell morphology, absence of intratubular growth and immunohistochemical study (positivity for kappa light chain and negativity for placental alkaline phosphatase) allow the exclusion of seminoma [4, 5, 11]. Lymphoma cells usually have a smaller cytoplasm, lack paranuclear halo, are frequently accompanied by sclerosis, and the immunohistochemical pattern generally shows positivity for CD20 or CD23 antigen and negativity for EMA10 [14]. Histologically, infiltration is demonstrated by the presence of atypical plasma cells. The expression of cytoplasmic monotypic immunoglobulins is objectively assessed by immunohistochemical techniques. The standard treatment of testicular plasmacytoma is radical orchiectomy. Radiation therapy and chemotherapy have not shown benefit. In the case of solitary testicular plasmacytoma, the treatment is radical orchiectomy, and the effectiveness of chemo or radiotherapy treatments is still under discussion. Cases of exclusive treatment with orchiectomy without recurrence have been described during short follow-up periods [15]. The prognosis of testicular plasmacytoma depends largely on whether or not it associates with a myeloma. In the latter case, the majority of patients present a worse prognosis [4]. In a review of 37 cases of multiple myeloma-related testicular plasmacytoma, I showed a postoperative survival ranging from 5 weeks to 18 months, with an average of 12 months [9].
References
-
Álvarez-Múgica M, Jalón Monzón A, Bulnes Vázquez V, Aguilar Andrea C, Fernández Gómez JM, et al. (2007) Secondary Testicular Plasmocytoma. Arch Esp Urol 60(1): 99-102.
-
Ulbright TM, Amin MB, Young RH (1999) Miscellaneous primary tumors of the testis, adnexa, and spermatic cord, hematopoietic tumors and secondary tumors. In: Rosai J (eds.) Atlas of tumor pathology, Tumors of the testis, adnexa, spermatic cord, and scrotum, tirad series. Armed Forces Institute of Pathology, Washington DC, pp: 235-290.
-
Anghel G, Petti N, Remotti D, Rucio C, Blandino F, et al. (2002) Testicular Plasmacytoma: Report of a case and Review of the Literature. Am J Hem 71(2): 98-104.
-
García Escudero A, Segura-Sánchez J, Navarro Bustos G, Poyato Galán JM, Figueredo Manrique A, et al. (2003) Plasmocitoma testicular: descripción de un caso. Rev Esp Patol 36(3): 329-332.
-
Shafqat A, Yum MN, Abanour R, Ganjoo KN (2003) Unusual Locations of Involvement by malignancies. Case1. Testicular plasmacytoma. J Clin Oncol 21(17): 3368-3369.
-
Croft GV, Albertyn LE (1992) Sonographic appearance of plasmacytoma of the testis. Australas Radiol 36(3): 265-267.
-
Bude RO (1999) Testicular plasmacytoma: appearance on gray-scale and power doppler sonography. J Clin Ultras 27(6): 345-346.
-
Pham T, Shetty SD, Stone C, De Peralta-Venturina M, Menon M (2000) Bilateral synchronous testicular plasmacytoma. J Urol 164(3): 781.
-
Oppenheim P, Cohen S, Anders K (1991) Testicular plasmacytoma: a case report with immunohistochemical studies and literature review. Arch Pathol Lab Med 115(6): 629-632.
-
Brambilla G, Pisoni A, Ballarti E, Turri E, Zaroli A, et al. (1993) Plasmacitoma del testicolo. Descrizione di un caso clinico e revisione della letteratura. Minerva Med 84(4): 211-215
-
Castagna M, Gaeta P, Cecchi M, Pagni GL, Pingitore R (1997) Bilateral synchronous testicular involvement in múltiple myeloma. Case report and review of the literature. Tumori 83(4): 768-771.
-
Tomoko S, Takashi K, Torhu A (1995) A case of extramedullary plasmacytoma of the testis diagnosed cystologically by scrotocentesis. J Jpn Soc Clin Cytol 34: 1156-1159.
-
Hou TY, Dai MS, Kao WY (2003) Testicular plasmacytoma with bone dissemination without medullary plasmacytosis. Ann Hematol 82(8): 518- 520.
-
Garrido Abad P, Coloma Del Peso A, Bocardo Fajardo G, Jiménez Gálvez M, Herranz Fernández LM, et al. (2008) Plasmocitoma testicular bilateral secundario. Aportación de un caso y revisión de la literatura. Actas Urol Esp 32(10): 1039-1042.
-
White J, Chan YF (1995) Solitary testicular plasmacytoma. Br J Urol 75(1): 107-108.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report