The Rising Obstacles and Hopes Available in Urethral Replacement
To the wide variation inside the anatomic presentation of hypospadias, no single urethroplasty may be applicable in each case. Further, Because of postoperative complications and a distinct shortage of tissue, a big number of different strategies have been evolved. Complication rates between 5 and 20% are stated in numerous centers, with variations likely depending on inclusion standards.
Introduction
To the wide variation inside the anatomic presentation of hypospadias, no single urethroplasty may be applicable in each case. Further, Because of postoperative complications and a distinct shortage of tissue, a big number of different strategies have been evolved. Complication rates between 5 and 20% are stated in numerous centers, with variations likely depending on inclusion standards. In general, the more extreme the phenotype, the better the risk of postoperative complications. Complications most usually include fistulas and urethra strictures, however additionally dehiscence of the repair, persistent chordee and poor cosmetic final results. Unsuccessful hypospadias repair can unfortunately grow to be a scenario of multiple repairs, justifying the descriptive term ‘hypospadias cripple’. More tissue is frequently had to be got to repair the lacking urethral tube in severe hypospadias instances. The best preference for plenty is a pedicle flap, which can be taken from the mucosal side of the foreskin and moved downside (Only method). The corners of this vascularized flap can then be fixed snugly to the corners and sides of the residual urethra via the usage of thin degradable stitches. The Only approach prevents round anastomose and therefore prevents stenosis on the quantity of the lower side suture lines. It has become pronounced the prevalence of 5 % of urethra-cutaneous connections, 1% of metal narrowing, and half % of diverticulum, whilst others stated negative drawbacks in 42% of the cases, which include anastomotic dehiscence in 7%, urethra- cutaneous connections in 23%, lumen narrowing in nine%, and abnormal dilatations of the urethra in 4% [1]. The Snodgrass technique has additionally been completed for severe hypospadias without extraordinary penile chordee (which sounds moderately opposing) and keeping in mind that the urethral plate is wide and flexible. In their collection of 33 proximal hypospadias cases studied, they expressed 33% of complications, of whom 21% being fistulas (Snodgrass and Lorenzo 2002). On the other hand, an Inlay process might be utilized to complete the urethroplasty as characterized before with detailed a win rate of 85%. An open door is utilizing free grafts to reconstruct the incomplete urethra. Cutaneous tissues have an awful reputation as a urethral substitute, particularly from outside the urogenital region. Utilizing bladder mucosa had a time of acknowledgment both in essential and re-try operations. In any case, outcomes on the long run had been disillusioning with numerous entanglements comprehensive of narrowing of the urethral meatus and diverticulation of the spongiosa, which mandated subsequent surgeries in two-thirds of the conditions. A free join of mouth lining taken from the internal part of the buccal wall or the lower lip is in actuality the most extreme for the most part settled choice. In a 5-year close monitoring of 22 such urethral replacements, it has been accounted for that 32% of drawbacks, especially narrowing, with 13% of the patients being operated again [2]. Others expressed intricacies in 57% of his cases, which incorporates five metal narrowing, seven stenosis, and one dehiscence. Results are higher while the unit is utilized as a partial circumference (Only) rather than as a complete tubular graft, with a lessening danger of narrowing. Bracka specified higher corrective outcomes the use of two-phase forms, fortified by utilizing Cloutier's system in 1962 [3]. In his own accumulation, Bracka detailed urethra-cutaneous holes in 5.7% and narrowing in 7% of the occurrences. Multistage strategies locate their best markers in multi-worked hypospadias and, as indicated by a few, in severe hypospadias while the urethral residual can't be safeguarded.
Current Management of Urethral Strictures and Limitations
Urethral strictures can end result from inflammatory, ischemic, or traumatic conditions. Those diseases result in scar tissue formation; scar tissue contracts and decreases the caliber of the urethral lumen, causing resistance to the antegrade passage of urine. The maximum commonplace reasons of urethral stricture these days are traumatic or iatrogenic. Much less-commonplace reasons encompass inflammatory or infectious, malignant, and congenital. Infectious urethral strictures are secondary generally to gonococcal urethritis, which stays not unusual in certain high-risk populations. Numerous methods are accessible for the treatment of urethral narrowing issue. Based absolutely at the literature, each approach in all actuality cannot be executed proficiently to each circumstance. Urologist who treats sufferers with urethral strictures ought to be knowledgeable about various procedures. Each technique has advantages and disservices. Presently, buccal mucosa free join urethroplasty has gotten great consideration in view of its astonishing early impacts and diminished level of inconvenience in examination with these of pedicle substitutes. To this point, a potential randomized review contrasting free unites and tissue folds have now not been led. In conclusion, most hypospadias conditions and urethral strictures can be managed efficaciously by using contemporary urethroplasty strategies which are associated with critical obstacles. Success rates in extra of 80% are suggested for two stage autologous graft urethroplasties. Thus, most anterior urethral strictures are efficaciously managed by current urethroplasty strategies, utilizing autologous tissue substitution while necessary. Restricted availability and donor site morbidity are risks of these surgical techniques.
The Role of Biomaterials and Regenerative Medicine in Urethral Replacement-Advances and Limitations
Massive research has been done inside the fields of biomedical designing to defeat the confinements related with front line urethral option enterprise. The main role has been to create a unite with qualities like buccal mucosa however which is helpfully accessible 'off the shelf', in boundless segments and without a grimness related with source region. Despite noteworthy advances, the optimum biomedical framework fabric has now not but rather been analyzed for use in clinical atmosphere. Tissue engineering carries the disciplines of cell transplantation and materials designing with the objective of discovering useful substitute to replace or repair damaged human tissue [4]. The basic necessities to tissue engineering any substitution material are a scaffold/matrix and an excellent blood delivery. Handiest small grafts can be sustained by means of this matrix and those require an incredible blood supply to permit tissue in growth. Alternatively, the scaffold may be seeded with cells that are expanded in culture before it is implanted to repair the tissue disorder. The scaffold itself can be made from naturally derived materials which includes alginate or collagen (Silver & Pins, 1992). Cellular matrices are prepared from natural tissues treated to remove cell components to produce a collagen-rich scaffold. Those biodegradable scaffolds offer a transient supportive structure, being absorbed slowly after implantation, developing the least host tissue response, scarring and fibrosis while being replaced by way of the regenerating tissues [5]. A latest study comparing biomechanical characteristics and biocompatibility of these natural scaffolds showed favorable properties in all with ACSM performing best, helping its potential use in urethral tissue engineering in future. Newer scaffolds, which includes silk fibroin, with ever growing biocompatibility and less capability for irritation are currently being, evolved [6]. Artificial polymers which includes polyglycolic (PGA) and polylactic acid (PLA) have also been evaluated as potential scaffolds, demonstrating no considerable cytotoxic outcomes. They own certain benefits over naturally-derived scaffolds [7]. They may be manufactured in huge portions and can be synthesized to fulfill precise properties (mechanical power, shape, length, porosity, degradation rate) essential for their intended use. Various creature models and clinical research have inspected an assortment of built urethral replacements amid the most last 3 decades. Both normal and Synthetic lattices, biodegradable and non-biodegradable, had been examined after a serious assessment of the literature. A mixture of resources of scaffold and cells is obvious on this literature but up to now the right ‘Artificial’ urethra has not yet been produced, even though a few researches have confirmed effective outcomes albeit in small series with very short follow-up. Earliest animal studies the use of Synthetic non-absorbable substances inclusive of Dacron and Polytetrafluoroethylene (PTFE) failed because of erosion, fistulation, failure to epithelialize, and stenosis [8]. Synthetic absorbable materials consisting of PGA mesh confirmed greater promising effects [9]. Unseeded, 'off-the-rack' cylindrical joins have not the slightest bit been used in medicinal trials. In creature models, they have just been effective in supplanting urethral imperfections under half centimeter long because disappointment of epithelialization of longer unites from sound encompassing tissues [10]. Disappointment of change of an urothelial layer at the luminal floor of the join brings about spillage of pee with related irritation and fibrosis prompting to re-stricturing. Unseeded unions utilized as a fix in a partial circumference form have demonstrated higher results in clinical trials [11]. Shockingly, this has not been recreated in longer strictures. 100% failure cites had been accounted for in stenosis longer than 40 mm [12]. A great deal less ideal impacts have been approved in patients who have had going before fizzled urethroplasties or those with a terrible vascularized tissue support, other options to customary substitution materials were used in comparative double group where for the most part looked for [13]. While in transit to treat longer strictures a seeded develop is by all accounts imperative since graft survival would be free of epithelialization. In a current canine creature display a seeded cylindrical unite (acellular porcine bladder submucosa platform impeded with its lining and muscle cellular components has been accurately utilized to supplant a 6 cm long bulbar urethral area with 100% accomplishment at 360 days monitoring [14]. The journey to look for a tissue-designed urethral unite has increased critical force as of late. There are various unmistakable procedures beginning from unseeded frameworks, single cell-seeded platforms and stratified refined epithelium. The part of each unite may also extend among individual clinical circumstances. As a case, a short essential urethral narrowing with a preferable injury bed might be taken care of with an a cellular join, yet the question should be asked for in the matter of regardless of whether this sufferer could be better treated with the guide of a urethral reconstruction with good success rate.
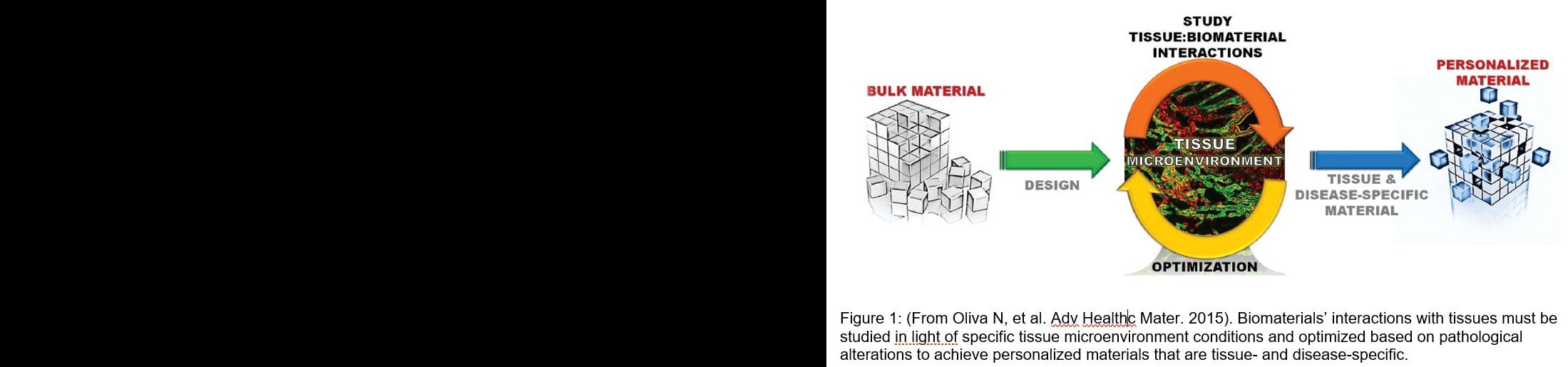
On the other hand, longer urethral stenosis or narrowing are most likely palatable managed by method for cellularized joins; and in this specific situation, the accessibility of the time rather than the simplicity of reaping oral mucosa for strictures of as much as 50 mm long should be addressed. The potential part of tissue designed urethral substitution conceivably exists with regards to extensive narrowing where there is a scarcity of local tissue, e.g., delayed lichen sclerosis stenosis, unavailability of oral mucosa comprehensive of taking after unsuccessful past substitution, where the accessible tissue has been used. Currently available scientific evidence depends on little observational research. Tissue engineering regularly starts with creation of a scaffold from a huge set of feasible assets. Then, cells are brought to the scaffold, in the nearness or nonappearance of growth factors - materials recognized for their excellent regeneration properties. Whilst culture conditions are appropriate, a tissue forms. In a few instances, the cells, scaffold element and growth factors are all blended collectively, allowing the tissue to “self- assemble”. Following transplantation, the proliferating cells and growth factors in the graft stimulate natural repair mechanisms in the faulty tissue. Recent developments in nanomedicine and biomedical engineering format combined with the exact examination of tissue-biomaterial cooperation can open a contemporary part in Personalized Medicine, in which biomaterials are chosen and intended to suit remarkable tissue sorts and disorder conditions. The view of a "one size suits all" biomaterial now not acceptable, as developing confirmation focuses to the significance of redoing material plan to engage (pre)clinical general execution. The mind-boggling microenvironment in vivo at extraordinary tissue destinations displays different cell sorts, tissue science, tissue phenotype, and mechanical burdens which are what is more changed with the guide of nearby disease. This intricate and element environment can likewise change the embedded material's qualities and thusly impact it’s in vivo standard execution. It is vital, in this way, to precisely take a gander at tissue setting and enhance biomaterials considering the implantation situations. This practice could empower fulfilling unsurprising material ordinary execution and improve clinical outcomes (Figure 1).
References
-
Elbakry A (1999) Complications of the preputial island flap-tube urethroplasty. BJU Int 84(1): 89- 94.
-
Dessanti A, Iannuccelli M, Ginesu G, Feo C (2003) Reconstruction of hypospadias and epispadias with buccal mucosa free graft as primary surgery: More than 10 years of experience. J Urol 170(4): 1600-1602.
-
Bracka A (1995) Hypospadias repair: The two- stage alternative. Br J Urol 76(S3): 31-41.
-
Atala A, Koh CJ (2004) Tissue engineering applications of therapeutic cloning. Annu Rev Biomed Eng 6: 27-40.
-
Santucci RA, Barber TD (2005) Resorbable extracellular matrix grafts in urologic reconstruction. Int Braz J Urol 31(3): 192-203.
-
Xie L, Li S, Li Q (2013) Surgical Treatment and Prevention of Recurrence of Urethral Calculi Associated with Hairballs after Urethroplasty. Urol Int 91(3): 256-260.
-
Boland ED, Wnek GE, Simpson DG, Pawlowski KJ, Bowlin GL (2001) Tailoring tissue engineering scaffolds using electrostatic processing techniques: a study of poly (glycolic acid) electrospinning. J Macromol Sci 38A(12): 1231- 1243.
-
Hakky SI (1977) The use of fine double siliconised Dacron in urethral replacement. Br J Urol 49(2): 167-171.
-
Olsen L, Bowald S, Busch C, Carlsten J, Eriksson I (1992) Urethral reconstruction with a new synthetic absorbable device. Scand J Urol Nephrol 26(4): 323-326.
-
Dorin RP, Pohl HG, De Filippo RE, Yoo JJ, Atala A (2008) Tubularized urethral replacement with unseeded matrices: what is the maximum distance for normal tissue regeneration? World J Urol 26(4): 323-326.
-
Fiala R, Vidlar A, Vrtal R, Belej K, Student V (2007) Porcine small intestinal submucosa graft for repair of anterior urethral strictures. Eur Urol 51(6): 1702-1708.
-
Palminteri E, Berdondini E, Fusco F, De Nunzio C, Salonia A (2012) Long-term results of small intestinal submucosa graft in bulbar urethral reconstruction. Urology 79(3): 695-701.
-
Elkassaby A, Kotb M (2016) Management of anterior urethral strictures with buccal mucosa: Our pioneering experience. Afr J Urol 22(1): 24- 32.
-
Orabi H, Abou Shwareb T, Zhang Y, Yoo JJ, Atala A (2013) Cell-Seeded Tubularized Scaffolds for Reconstruction of Long Urethral Defects: A Preclinical Study. Eur Urol 63(3): 531-538.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report