Uretero-Arterial Fistula: A Modern Case of an Orphan Disease
Uretero-arterial fistula (UAF) is an uncommon source of hematuria, but as a harbinger of mortality, diagnosis can potentially be lifesaving. While rare, there is a general consensus that the incidence is rising.
Introduction
Uretero-arterial fistula (UAF) is an uncommon source of hematuria, but as a harbinger of mortality, diagnosis can potentially be lifesaving. While rare, there is a general consensus that the incidence is rising. The condition develops when an aberrant connection is made between a ureter and artery, and the presentation varies from microscopic hematuria to frank hemorrhage. UAF is seldom expected, but having a clinical suspicion is paramount for guiding decision-making. There have been some case reports, but data is scarce regarding etiology and management [1, 2, 3, 4]. Thus, we offer our personal experience to help validate current diagnostic and treatment options. Keywords: Uretero-arterial fistula; Cystoscope; Looposcopy; Pyelogram
The Case
A 66-year-old male was diagnosed with stage IV urothelial cell carcinoma of the bladder (pT2N1M0) in 2008. He underwent neoadjuvant chemotherapy with gemcitabine and cisplatin (GC), followed by a radical cystoprostatectomy with ileal loop urinary diversion and bilateral extended pelvic lymph node dissection in 2009. He developed recurrence of disease at the aortic bifurcation, abdominal wall, and ureteral margin in 2010, 2013, and 2014, respectively. This was treated with additional chemotherapy, as well as 3 reoperations (lymph node dissection, resection of the abdominal wall mass, and conduit revision), and adjuvant radiation. He sought the opinion of several major NCCN designated cancer institutions and was enrolled in a clinical trial after a lymph node biopsy was positive for a Src mutation, which led to targeted chemotherapy with bosunitinib. Post-treatment, he developed widespread abdominal and pulmonary recurrences. He was given another 5 cycles of GC, which this time showed regression of metastasis. In October 2015, the patient was admitted to the hospital for a small bowel obstruction and was found to have renal insufficiency with bilateral hydronephrosis. This was due to stricture of the distal ureters which was initially managed with bilateral nephrostomy tubes before being converted to 8.2F single J ureteral stents. Shortly after this procedure, the stents needed to be exchanged due to stent migration and malposition. Following this, he was managed with stent exchanges every 3 months. During his stent exchange in April 2016, wires were passed up the single J stents emanating from the ileal conduit. The right stent was exchanged, followed by the left. Upon removal of the left stent, there was some resistance noted, which was overcome with gentle, steady pressure. Immediately upon removal, profuse bleeding was seen coming from the urostomy. A finger was placed in the conduit and anesthesia was asked to place another IV line, and obtain a type and cross. Unsure of where the bleeding was coming from, Interventional Radiology (IR) was contacted for an immediate intra operative consult. Several minutes later, when the interventional radiologist arrived, the finger was removed and no more blood was seen coming from the stoma. The conduit was irrigated free of the extensive clots that had accumulated. Looposcopy was then performed with a flexible cystoscope showing a small amount of oozing from around the wire at the left ureteral orifice. The concern at this point was for possible erosion of the stent into the parenchyma of the kidney (as evidenced by the resistance upon removal), and thus after discussion it was decided that there was no need for IR intervention. We continued with our procedure, and a 5F open-ended catheter was advanced over the left ureteral wire and a retrograde pyelogram was performed. This showed multiple filling defects within the renal pelvis consistent with blood clots (Figure 1). The new single J stent was placed and our patient was admitted for observation.
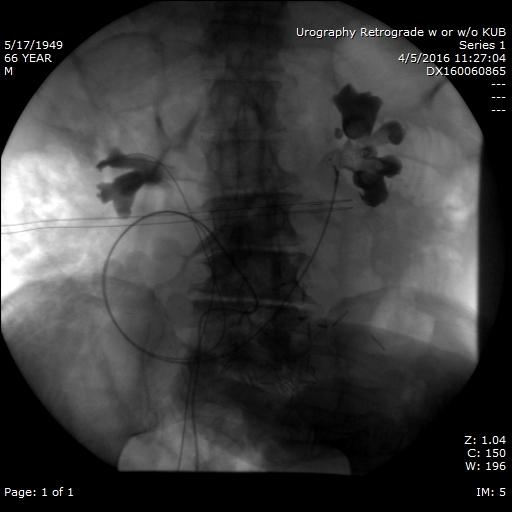
Figure 1: Retrograde pyelogram at the time of stent exchange. Multiple filling defects are seen within the left renal pelvis representing blood clot. As blood entered the ureter via the fistula, it traveled retrograde and collected in the renal pelvis. Additionally, no contrast was seen entering the fistula or artery either because the fistula had either already clotted off, or the pressure within the fistula was greater than that of our injecting pressure.
Hospital Course
Postoperatively, the patient remained asymptomatic with stable vital signs. His hemoglobin did fall from 10.3 to 8.2g/dL, and his is urine was tea-colored, consistent with known blood clots in the renal pelvis. He developed acute renal insufficiency with a rise in creatinine from 1.02 to 2.55mg/dL, concerning for a poorly functioning left stent. Thus, he received a left percutaneous nephrostomy tube. At this point, urine output from the nephrostomy output was tea-colored, while his stoma became clear. His renal function improved to baseline and he was discharged home the following day.
Follow Up
At follow-up 3 weeks later, he was complaining of flank pain and a KUB was performed, showing his stents had migrated distal to the ureteropelvic junction. He was thus scheduled for a stent exchange, this time opting for indwelling 6Fx24cm double J stents. During this exchange, a small amount of bleeding was seen from the left ureteral orifice, which stopped prior to the conclusion of the case, and the patient was discharged home. The following evening, he was re-admitted after having had a large blood clot as well as both ureteral stents expelled from his ileal conduit while at home. On arrival to the hospital, no further bleeding was appreciated, but his hgb was
6.2mg/dL, thus he was admitted, transfused 2 units of pRBCs, and his hgb improved to 8mg/dL. Subsequently, bilateral nephrostomy tubes and antegrade ureteral stents were placed by IR.
Diagnosis and Treatment
Attempting to find the etiology, a tagged RBC scan was performed to rule out renal parenchymal bleeding, which was non-diagnostic. We then pursued work up for a ureteral-arterial fistula similar to that described by Hirsch et al. [5]. IR performed a provocative angiogram, which revealed a left sided uretero-common iliac artery fistula. A covered vascular stent was placed, which showed no further extravasation of contrast into the ureter (Figure 2). At the end of this procedure, he was left with the arterial stent, a left nephrostomy tube, and a right nephroureteral stent. The patient was closely monitored and remained asymptomatic. He was sent home and has been free from any other gross hematuria episodes.
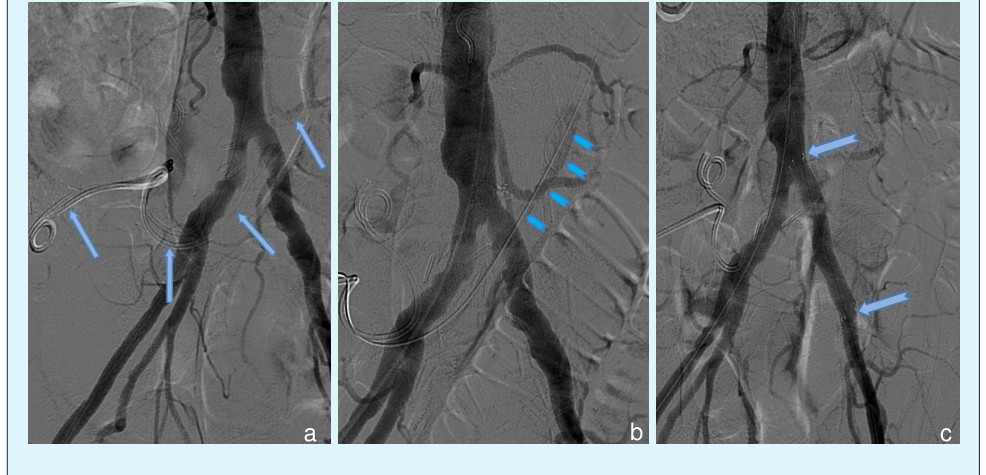
Figure 2: Angiogram series showing the ureteral stents in place with the arrows following the left stent (a.), followed by a provocative angiogram (b.) that shows the aorta with contrast entering the left ureter (ribbon arrows), and after demonstration of the UAF, a covered stent was placed within the left common iliac artery (split-tail arrows) spanning the distance of the fistula (c.).
Discussion
There have been two studies, dating back to 1997, which looked at UAF retrospectively, both examining the incidence and risk factors for developing UAF, treatment options, and the outcomes with proposed algorithms for disease management [5, 6]. There are two types of UAF: primary and secondary. Primary UAF is less common, and comes from intrinsic pathology in the patient (i.e. arterial aneurysms, atherosclerosis, or arterial-venous malformations). Secondary UAF develops with external risk factors such as a history of pelvic surgery, radiation therapy, or indwelling ureteral stents [1, 7, 8]. The patient in our case had 4 of these conditions. A common element among these secondary causes is the creation of a fixed and more rigid surface for the systolic arterial pulsations to press against, theoretically inducing pressure necrosis and fistula development [7] (Figure 3). About 80 cases of UAF have been reported since 2004 [2, 5, 6, 9] and only a handful of case reports since then. Additionally, for historical reference, there were 3 cases of UAF found in pregnancy, each dating back to the late 1930s [10, 11, 12]. All 3 women had complicated UTIs and died from either hemorrhage or sepsis, and the diagnosis of UAF was made at autopsy.
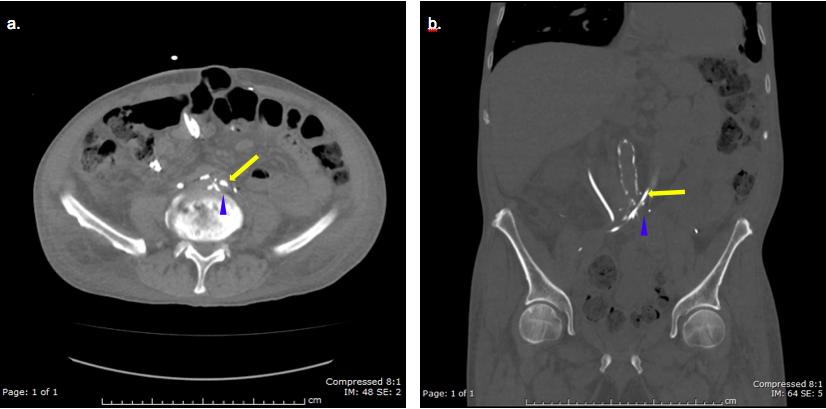
Figure 3: Non-contrast CT of the abdomen and pelvis. a.) Axial view with the abdominal window shows the left ureteral stent passing (arrow) over the left common iliac artery (arrow head). b.) Coronal view in the bone window shows more clearly the stent (arrow) coursing over the iliac artery (arrow head). There is also significant atherosclerosis of the abdominal aorta and iliac arteries. This allows for 2 rigid and relatively fixed environments, which over time sets the stage for fistula formation.
Making the diagnosis can be a major challenge. While hematuria and even bloody efflux seen on cystoscopy should heighten suspicion, this does not make the diagnosis of UAF. Retrograde pyelogram, and CT scan both have low sensitivity for diagnosis, ranging from 45- 50% [7]. Often the fistulous tract can be obscured by a stent on CT scan, plugged by a clot, or the arterial pressure may be enough to overcome the injection pressure of contrast dye on retrograde pyelogram, preventing visualization the fistula. What has become the most sensitive and specific diagnostic test is a provocative angiogram. This involves the manipulation of a ureteral stent just prior to angiogram so that the fistula tract is freshly opened. Tagged RBC scans are not part of the suggested work up because the scan requires active bleeding to make a diagnosis and offers poor anatomic detail. Patients who are bleeding significantly enough to be seen on tagged RBC scan are usually not stable enough for the test. Once the diagnosis is made, prompt treatment is needed, and the options universally require an intervention, either open surgical or endovascular. More specifically, open ligation of the fistula, arterial bypass grafting, and/or nephroureterctomy are the surgical options, while endovascular grafting, or coiling are the minimally invasive techniques. Ureteral stenting is not recommended because at best this will temporize the problem, and potentially exacerbate (i.e. inducing hemorrhage, or enlargement of) the fistula, which is what we saw in our case. There are a multitude of factors to consider when choosing an intervention, such as surgeon abilities, availability of endovascular services, and prior surgical interventions. Due to its minimally invasive approach and ability to perform treatment at the time of diagnosis, endovascular grafting is gaining popularity as the treatment of choice. However, Krambeck et al. views this only as a temporary measure because placing the graft and not addressing the fistulous connection increases the risk of graft infection [7, 6]. Thus, their algorithm would incorporate urinary diversion (i.e. nephrostomy tube) for those patients receiving an endovascular stent. However, only those patients who are poor surgical candidates would receive this stent in the first place, since their model favors primary open surgical repair for those deemed eligible. Our patient ended up having a urinary diversion in concordance with this algorithm.
Closing Thoughts
It can be difficult to anticipate a UAF, and any single physician is unlikely to encounter the disease more than once, if at all, in their career. This is a dangerous combination for providing efficient and successful treatment outcomes. Patients with UAF are often complex both medically and surgically, which adds more layers of difficulty in diagnosis and treatment. Our patient had a significant delay in diagnosis, but was fortunate to have a good outcome. Furthermore, our institution was equipped with the expertise and technology available to eventually provide an accurate diagnosis and curative treatment. This case provides heightened awareness for diagnosing UAF and the current algorithm led to a successful outcome in our patient.
References
-
Kim DH, Mahdy A, Mundra V, Berman M, Ghoniem GM (2009) Ureteroarterial Fistula. Case Reports in Medicine (2009): 1-4.
-
Chehab Monzer, Alexander Copelan, Charles Cash, Howard Korman, Purushottam Dixit (2014) Endovascular Management of Ureteroarterial Fistula: A Rare Potentially Life Threatening Cause of Hematuria. J Radiol Case Rep 8(7): 37-45.
-
Sukha A, N Smyth (2015) Fistula Formation between the External Iliac Artery and Ileal Conduit following a Radical Cystoprostatectomy: A Rare Complication with Prewarning Signs of Haemorrhage. BMJ Case Repo (2015): 1-2.
-
Muradi A, Yamaguchi M, Idoguchi K, Okada T, Nomura Y, et al. (2013) Lessons Learned From Endovascular Management of Ureteroarterial Fistula. Vascular and Endovascular Surgery 48(2): 159-161.
-
Hirsch LM, Amirian MJ, Hubosky SG, Das AK, Abai B, et al. (2015) Urologic and Endovascular Repair of a Uretero-Iliac Artery Fistula. The Canadian Journal of Urology 22(1): 7661-7665.
-
Vandersteen DR, Saxon RR, Fuchs E, Keller FS, Taylor LM, et al. (1997) Diagnosis and Management of Ureteroiliac Artery Fistula. J Urology (1997): 754- 758.
-
Krambeck AE, Dimarco DS, Gettman MT, Segura JW (2005) Ureteroiliac Artery Fistula: Diagnosis and Treatment Algorithm. Urology 66(5): 990-994.
-
Aslam MZ, Kheradmund F, Patel N, Cranston D (2010) Uretero-Iliac Artery Fistula: A Diagnostic and Therapeutic Challenge. Advances in Urology (2010): 1-3.
-
Bergqvist D, Pärsson H, Sherif A (2001) Arterio- ureteral Fistula – a Systematic Review." European Journal of Vascular and Endovascular Surgery 22(3): 191-196.
-
Hamer H (1939) Fatal ureteral hemorrhage due to erosion into the iliac artery. Trans Amer Ass Geritourinary Surgery 32: 177-183.
-
Taylor W, Reinhardt H (1939) Mycotic aneurysm of common iliac artery with rupture into right ureter. J Urol 42: 21-26.
-
Davidson O, Smith R (1938) Uretero-arterial fistula. J Urol 42: 257-262.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report