Acute Renal Failure in an HIV Patient: The Importance of Antiretroviral Treatment and Concomitant Medications
<p>Antiretroviral treatment has significant side effects, including wasting syndrome, lipodystrophy and kidney damage. The authors present a 49-years female patient who developed acute renal failure after the intake of NSAIDs at the background of combined antiretroviral regimen (lopinavir, ritonavir, tenofovir, emtricitabine).</p>
Letter to Editor
Dear Sir,
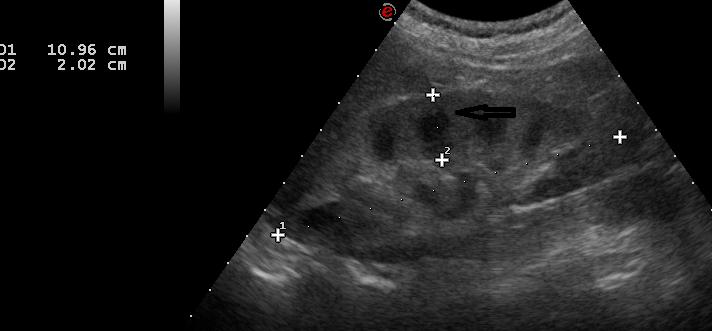
A 49-years-old female patient was admitted to the Clinic of Nephrology at the University Hospital Alexandrovska – Sofia, in December 2017 for diagnostic evaluation of newly-found renal failure – serum creatinine 260 mcmol/l, and anemia – hemoglobin of 100 g/l. The patient reported nausea, vomiting, weight loss of 12 kg for the past 3 months with preserved appetite and redistribution of the body fat, fatigue, muscle, joint and bone pains, and muscle wasting. In 2013 she was found HIV-positive and has been on antiretroviral treatment since then with excellent viral response. Her renal function was normal until September 2017. In the beginning of December she was admitted to Neurology unit for muscle pain and muscle wasting and did not report the presence of HIV infection and the intake of antiretroviral treatment to the attending physician. In the Neurology unit she received non-steroid anti inflammatory drugs (NSAIDs), Dexamethasone, Mannitol, and Ciprinol for urinary tract infection, and was referred to our Clinic for diagnostic evaluation of renal Letter to Editor failure and anemia of unknown origin. At the admission to our clinic the patients reported past history of appendectomy, viral hepatitis and urinary tract infections. At the admission the patient was n treatment with: lopinavir 133.3 mg + ritonavir 33.3 mg 2 tablets bid and tenofovir 245 mg + emtricitabine 200 mg 1 tablet a day. The physical examination revealed lipodystrophy, pale skin and linings, decreased muscle strength in the extremities, unstable gait, aphthous lesions in the mouth cavity, blood pressure 130/80 mm Hg. The rest of the physical examination was unremarkable. The clinical-laboratory investigations at the admission revealed anemia (hemoglobin 99-86 g/l, hematocrit 30- 27%, RBC 2.9-2.6 T/l), WBC 11.9 G/l (after corticosteroid treatment with Dexamethazone), differential count: neutrophils 78%, lymphocytes 13%, eosinophils 1%, basophils 0%, platelet count 196-181, MCV 106 fl, MCH 34 pg, urea 14.2 mmol/l, creatinine 244 mcmol/l, potassium 3.18 mmol/l, sodium 148 mmol/l, calcium2.06 mmol/l, phosphates 0.61 mmol/l, total protein 62 g/l, albumin 39 g/l, uric acid 152 mcmol/l, normal liver enzymes, cholesterol and triglycerides, normal coagulation tests, alkaline-base balance: pH 7.25, рСО2 2.52 kPa, рО2 22.1 kPa, standard bicarbonate 10.6 mmol/l, base excess (-18) mmol/l, O2 saturation 98%, total СО2 7.9 mmol/l. Urine: pH 5, specific gravity 1025, protein, blood, leukocytes positive, bilirybin negative, urobilinogen normal, sediment: 5-6 RBC, mass WBC and casts. Proteinuria 0.67 g/l. Urine microbiological investigation (urine culture) – no bacterial growth. The ECG examination and the chest X-ray were unremarkable. The abdominal ultrasound scan revealed cholelithiasis and diffuse renal parenchymal disease (figure 1).
safe antiretroviral agent but is known to cause a wide variety of tubular changes, ranging from acute tubular- cell death to interstitial nephritis with severe but reversible tubular dysfunction - Fanconi-syndrome-like condition with glucosuria, phosphateuria, aminoaciduria, urinary potassium and bicarbonate loss and severe metabolic acidosis [1, 2, 3]. Ritonavir is also known to cause renal damage [1, 2, 3] and to increase the propensity of tenofovir to cause renal damage due to increase in intracellular tenofovir levels within the proximal tubular cells [3]. NSAIDs also have negative impact on renal function and can cause tubule-interstitial nephritis and tubular dysfunction, and can deepen the nephrotoxic impact of antriretroviral agents. Furthermore, renal failure in HIV-positive individuals may be due to thrombotic thrombocytopenic purpura, other nephrotoxic medications (including, antibiotics, NSAIDs, etc.), immune-mediated and HIV-associated nephropathy [2, 3]. In our patient we observed the classical muscle wasting syndrome, fatigue, muscle and bone pains and lipodystrophy induced by antiretroviral treatment [4, 5]. These changes were accompanied by acute tubular dysfunction with severe metabolic acidosis, hypokaliemia and hypophosphatemia, and acute renal failure that improved after cessation of antiretroviral and NSAIDs treatment. Therefore, in every patient with acute renal injury with severe metabolic acidosis, hypokaliemia and especially with hypophosphatemia, antiretroviral treatment should be suspected as a causative factor and the patient should be pro-actively asked for the intake of such medications. The development of renal abnormalities at the background of anti-HIV treatment should lead to prompt re-evaluation of the therapeutic strategy.
References
-
Rho M, Perazella MA (2007) Nephrotoxicity associated with antiretroviral therapy in HIV-infected patients. Curr Drug Sag 2(2):147-154.
-
Roling J, Schmid H, Fischereder M, Draenert R, Goebel FD (2006) HIV-associated renal diseases and highly active antiretroviral therapy-induced nephropathy. Clin Inf Dis 42(10): 1488-1495.
-
Kalyesubula R, Perazella MA (2011) Nephrotoxicity of HAART. AIDS Res Treat 2011: 11.
-
Carr A, Cooper DA (2000) Adverse effects of antiretroviral therapy. Lancet 356(9239): 1423-1430.
-
Reust CE (2011) Common adverse effects of antiretroviral therapy for HIV disease. Am Fam Physician 83(12): 1443-1445.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report