Retroperitoneal Lymphangioma with Chyluria
<p>A 37 years old lady presented with blood in urine and weight loss for 3 months. Urine report confirmed chylomicrons and contrast enhanced CT scan revealed a retroperitoneal mass extending from mediastinum to pelvis. MRI findings suggested a diagnosis of lymphangioma. She underwent bilateral retrograde pyelography with betadine instillation. Her chyluria subsided after this treatment. This case is rare in view of association of lymphangioma with chyluria which responded to minimal invasive endourological approach.</p>
Waseem sheikh5
scsahay@rediffmail.com.
responded to minimal invasive endourological approach.
Keywords: Lymphangioma; Chyluria; Retroperitoneal
Introduction
Chyluria is prevalent in those patients coming from endemic zone of filariasis. Tuberculosis and malignancy are other non parasitic causes of chyluria. Retroperitoneal lymphangioma has occasionally been reported as causing chyluria [1]. Chyluria associated with retroperitoneal lymphangioma is very rare. We are presenting a rare such case which responded to endourological treatment.
Case Report
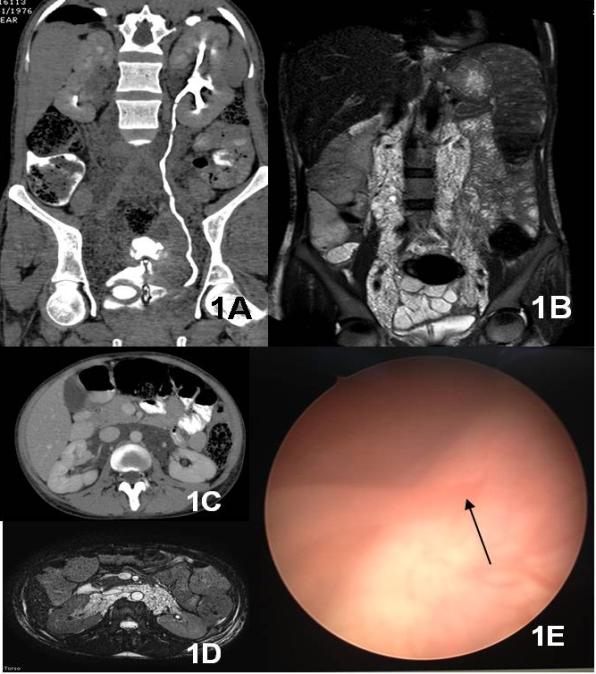
and bilateral pedal edema. Urine colour was red with passage of clots. Serum biochemistry revealed normal kidney function test, anemia (Hb 3.8 gm/ dl), leucocytosis (Total wbc count 13400) and hypoproteinemia (total protein 4.31 gm/dl, albumin 2.19 gm/dl). Urine was turbid and milky. Urine microscopy revealed 20-25 RBC/ high power field and 5-7 pus cells. Urine culture was sterile and AFB staining did not reveal any mycobacteria. Urine was positive for chylomicrons (27 gm/dl) and 24 hr urinary protein excretion was 11.2 gm. Contrast enhanced CT scan revealed bilateral kidneys to be normal in size with normal nephrogram. Both ureters were normal. Low attenuating heterogeneous non enhancing hypodense infiltrative mass (value ranges from -5 to 15HU) seen in retro- peritoneum encasing vessels and extending inferiorly along bilateral iliac vessels, superiorly into mediastinum and also in bilateral perinephric space, renal hilum and mesenteric root. MRI abdomen revealed extensive cystic / fluid signal intensity lesion creeping in retroperitoneum extending from the level of celiac axis till pelvis encasing the aorta and its branches and bilateral iliac arteries showing hyperintense signal on T2W and FAT SAT images. This finding most likely represented lymphangioma (Figure 1A-D). Patient was given 4 units packed RBC transfusion, IV albumin injections and IV Ceftriaxone 1 gm twice daily. She was planned for cystoscopy after stabilizing the biochemical parameters. Cystoscopy revealed dirty, milky urine with clots (Figure 1E). Right ureteric orifice was normal whereas left uretric orifice revealed reddish white, thick urine efflux. Left sided retrograde pyelography was done which showed peripelvic and periureteric leakage of contrast and visualisation of lymphatics. Under fluoroscopic guidance a 6Fr ureteric catheter was passed into the left ureter and positioned in the pelvis. 10 ml of diluted solution of povidone iodine (2 ml of 5% povidone iodine + 8 ml of distilled water) was instilled into the renal pelvis and 6 Fr DJ stent was placed. Patient was observed for 48 hrs in the hospital. Her urine became clear and she was discharged. Patient was not having any hematuria till 1 year follow up.
Discussion
Chyluria is usually associated with TB, Filariasis and malignancy. Chyluria can lead to weight loss and weakness due to loss of absorbed nutrients as in our case. Endemic cases usually do not require surgical intervention. Conservative management include dietary manipulations with omission of long chain triglycerides (TG), drug therapy with diethyl Carbamazepine and bed rest. Non endemic cases usually require surgical intervention. Various types of sclerosing agents have been proposed for renal pelvic instillation (1% Silver nitrate, povidone iodine, 50% glucose, normal saline, 10-25% sodium iodide and 15% potassium iodide). Instillation of povidone iodine induces inflammation and edema followed by fibrosis in the lymphatic channels leading to permanent blockage and cure of chyluria. It has shown promising results in some cases [2]. Those patients not responding to conservative measures and having severe nutrient loss may require surgical treatment. There has been case report showing chyluria associated with retroperitoneal lymphangioma but that was managed by bilateral nephro ureterolysis [1]. This patient was unique in the sense that she responded very well to endourological treatment.
References
-
Kekre NS, Arun N, Date A (1998) Retroperitoneal cystic lymphangioma causing intractable chyluria. BJU 81: 327-328.
-
Bhat S, Kishore TA, Govindan H, Dineshan KM, Cardoza F (2005) The Efficacy and Safety of Povidone Iodine in the Management of Chyluria. The Internet Journal of Urology 2(2): 4.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report