Interventional Radiology Techniques in the Genitourinary Tract
<p>The increasing use of interventional radiology techniques for diagnosis and treatment in different fields of medicine has shown its great benefits since it involves techniques that avoid carrying out extensive procedures in unstable patients or with multiple comorbidities, reduce surgical times, incidence of complications and hospital stay. In the field of nephrology and urology, interventional radiology represents a fundamental support in diagnostic and therapeutic with procedures such as kidney biopsy, nephrostomy placement, double J catheters and cystostomies, ablation and embolization techniques. In this mini review, we present the most frequently performed interventional procedures of the genitourinary tract, with their main indications, contraindications and some illustrative examples.</p>
Introduction
Interventional radiology, also known as minimally invasive therapy, is a sub specialization of radiology that consists in performing diagnostic and therapeutic procedures with minimally invasive techniques guided by diagnostic images as fluoroscopy, ultrasound, scanography or magnetic resonance imaging. The specialty was born in the United States in the 60s with doctors Charles Dotter and Bill Cook, and today it represents a fundamental part for the diagnosis and treatment in multiple fields of medicine. These techniques not only avoid carrying out extensive procedures in unstable patients or with multiple comorbidities, but also reduce surgical times, incidence of complications, hospital stay and costs, and promote the interaction of different specialists to provide a multidisciplinary and more complete management to patients. In the field of nephrology and urology, interventional radiology plays a fundamental role in terms of diagnostic and therapeutic support. Procedures such as renal biopsy, placement of nephrostomies, double J catheters and cystostomies are very common in daily practice. In addition, there are ablation techniques for renal tumors or embolization for acute management of bleeding or definitive management of masses that are increasingly used for its high benefits with lower rates of complications.
In this mini review, we present the most frequently performed interventional procedures of the genitourinary tract, with their main indications, contraindications and some illustrative examples.
Mini Review
Percutaneous renal biopsy consists of obtaining tissue for pathological or cytological analysis. It can be non- localized when evaluating a diffuse parenchymal disease, or localized when there is an isolated lesion from which the sample is obtained. Indications include unexplained acute or progressive renal failure, nephrotic syndrome or proteinuria, persistent hematuria, systemic diseases with renal involvement (such as lupus or scleroderma) and renal transplant dysfunction. Practically there is no absolute contraindication for its performance, and the relative ones include coagulopathy and arterial hypertension, which once controlled do not represent any risk for the procedure [1, 2]. Although a transjugular approach can be performed, the most frequent is the percutaneous approach with the patient in prone position (native kidney) or supine (transplanted kidney), using automatic or semiautomatic needles of 16-18G, always with a path away from the renal hilum. Non-localized biopsies are taken from the renal cortex, while localized biopsies should have a pathway that contains healthy parenchyma between the capsule and the lesion to reduce the risk of hemorrhage (Figure 1). At least 2 samples of 1 cm in length should be obtained that include a minimum of 5 glomeruli if a glomerular lesion is being evaluated, 6-10 glomeruli for tubulointerstitial injury and 7 glomeruli in transplanted kidney. The most frequent complications include the formation of intra- or perirenal hematomas (Figure 2), hematuria that is usually self-limited, arteriovenous fistula formation or pseudoaneurysm that usually resolves spontaneously and injury to other organs such as the colon or lung.

(a)

(b) Figure 1: a) Longitudinal section of ultrasound showing localized renal biopsy of a mass in the upper pole of the left kidney in a male patient of 72 years, which resulted in a plasmacytoma. b) Longitudinal section of ultrasound showing non-localized renal biopsy in a 29-year-old patient with a history of Lupus and proteinuria.
![Figure 3: Control pyelography after placement of left nephrostomy, where adequate position and functioning are confirmed. The placement of double J catheters follows the same steps for the placement of the nephrostomy but the guide and catheter are advanced to their final position: proximal within the renal pelvis and distally within the bladder (Figure 4). Indications include renal lithiasis, ureteral fistula, ureteral stenosis, urinoma or risk of displacement of a nephrostomy. The only contraindication, which is relative, is coagulopathy. Among the most frequent complications are clogging or embedding of the catheter, its distal migration or, less frequently, ureteral rupture [1,6].](/fulltextimages/1655/fig_3.jpeg)
Figure 2: Axial ultrasound section showing perirenal hematoma as a biopsy complication in a 16-year-old female patient with lupus nephropathy. Percutaneous nephrostomy is the placement of external drainage in the renal collecting system. Its main indication is the presence of urinary leaks, decompression of renal or perirenal collections or to facilitate percutaneous access for other urological procedures (stent placement, nephrolithotomy, extraction of foreign bodies, administration of medication). The only contraindication, which is relative, is coagulopathy. As for the renal biopsy, the position of the patient must be prone (native kidney) or supine (transplanted kidney), and the approach must be made by Brodel's avascular plane, which is about
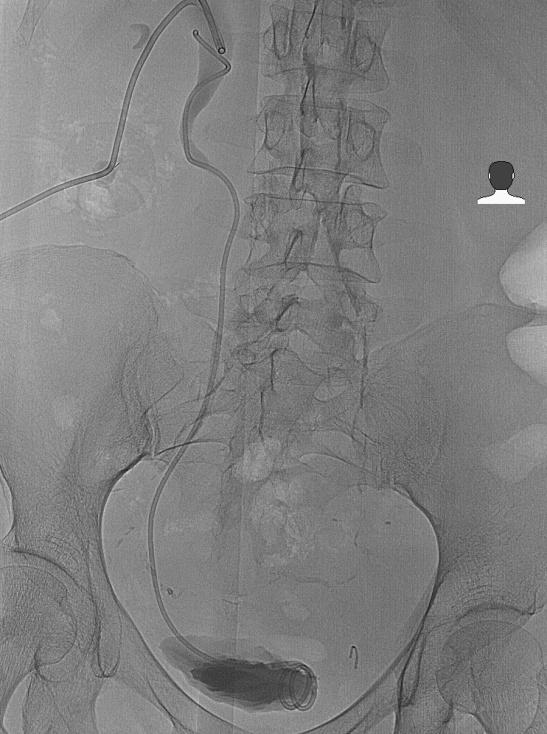
20-30º from the plane sagittal and represents obstructive hydronephrosis or pyonephrosis, but it can also be used for the management of fistulas or the junction point of the anterior and posterior circulation. Once the desired calyx has been identified (ideally in the lower pole of the kidney), the puncture is performed under local anesthesia and with Seldinger technique the catheter (8-10 F) is placed within the renal collecting system, ideally in the pelvis, position which is confirmed by pyelography (Figure 3). Among the complications that may occur are bleeding, infection and injury to adjacent organs, a risk that increases depending on the caliber of the catheter used [1, 3, 4, 5].

Figure 3: Control pyelography after placement of left nephrostomy, where adequate position and functioning are confirmed. The placement of double J catheters follows the same steps for the placement of the nephrostomy but the guide and catheter are advanced to their final position: proximal within the renal pelvis and distally within the bladder (Figure 4). Indications include renal lithiasis, ureteral fistula, ureteral stenosis, urinoma or risk of displacement of a nephrostomy. The only contraindication, which is relative, is coagulopathy. Among the most frequent complications are clogging or embedding of the catheter, its distal migration or, less frequently, ureteral rupture [1, 6].

(a)
(b) Figure 4.Placement of leftnephrostomyand ureteral stent. a) The same steps are carried out as for the placement of a nephrostomy and the catheter is advanced to its final position. b) Final position of the ureteral stent with proximal end in the renal pelvis and distal end in the bladder.
Cystostomy is the placement of a percutaneous drainage catheter into the bladder above the pubic symphysis. Its indications include bladder outlet obstruction in patients with prostatic disease, urinary incontinence, neurogenic bladder, bladder fistula or urethral trauma, among others. The only contraindication is coagulopathy, which once corrected does not represent a greater risk. The patient should be in a supine position, with a full bladder (this can be done through a bladder catheter with normal saline) and the ideal approach is median or paramedian immediately above the pubic symphysis. The puncture can be performed directly with the catheter set on a trocar (trocar technique), or with an exchange system using the Seldinger technique. Once the procedure is finished, the position of the catheter must be confirmed with the injection of contrast medium. The most frequent complications are the development of bladder stones, urinary leakage, or migration of the catheter [1, 7]. Embolization or exclusion of renal arteries consists of the occlusion of renal blood vessels, both major and minor caliber. The most frequent indications include: (1) severe renal trauma (category II) or associated with the formation of pseudo aneurysms and fistulas, (2) treatment of renal angiomyolipomas when acute bleeding occurs or as prophylaxis when the tumor size is greater than 4 cm or there are intralesional aneurysms greater than 5mm (Figure 5), (3) exclusion of renal artery aneurysms when they are greater than 2 cm, when they are associated with poorly controlled hypertension or when they show growth, (4) complete renal occlusion in dysfunctional kidneys when patients are not candidates for surgery and as pre-surgical or palliative management in patients with renal cell carcinoma. The most widely used access is the femoral artery, through which selective or supraselective catheterization of the renal artery or its branches is performed to administer different embolizing agents in the desired location. Among the most common embolizing agents are particles, coils, ethanol and Onyx. Hematuria is frequent and self-limiting after the procedure and up to 90% of patients develop postembolization syndrome, which represents the inflammatory response to necrotic tissue and manifests with pain, nausea, vomiting and fever; it requires only symptomatic management. Other more feared and less frequent complications include the rupture of aneurysms during the procedure, arterial injury, erroneous embolization, formation of bruises, abscesses and reactive pleural effusion [1, 8].
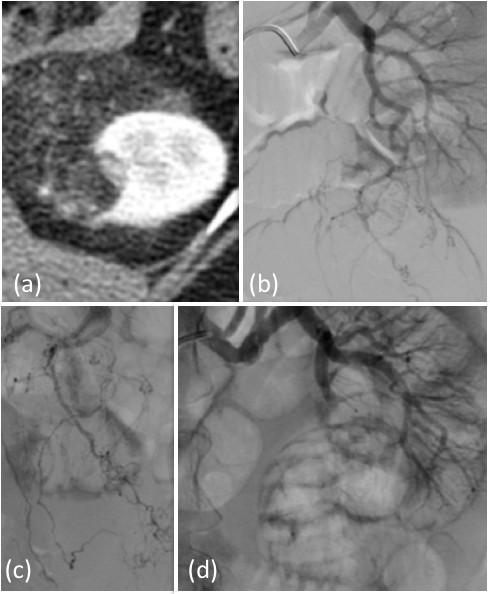
Figure 5: (a) Axial section of abdominal CT in which left renal angiomyolipoma is demonstrated. (b) Angiography image by selective digital subtraction of the left renal artery. The branches supplying the lesion are detected (c), and embolization is performed with PVA microparticles (d), with subsequent evidence of an adequate supraselective embolization of the lesion. Tumor ablation consists in the direct local percutaneous destruction of the malignant tissue through the application of energy (radiofrequency, freezing, microwaves) or chemical substances. The most commonly used modalities are radiofrequency ablation where heat is used and microwave ablation where cytotoxicity is also produced by heat. It is used as alternative management to surgery in patients with renal cell carcinoma (ideally lesions <4 cm) who are not surgical candidates for other comorbidities or in whom it is desired to preserve functioning renal parenchyma due to other causes such as a single kidney, kidney failure, von Hipple-Lindau syndrome, among others. It also represents a management option in patients with renal angiomyolipomas greater than 4 cm or with aneurysms greater than 5 mm. The procedure is contraindicated in patients with non-correctable coagulopathy and when the lesions to be treated are greater than 4 cm or are very close to vascular structures or to the collecting system, due to the risk of associated injury.
Once the ablation needle is located in the center of the lesion (percutaneously), hydrodissection is performed and heat is administered. In 90% of cases of lesions <4 cm complete necrosis is achieved; however, the incidence of recurrence has been reported up to 13.4%. Among the most frequent complications are hemorrhage, pleural effusion and skin burn. Other less frequent complications include vascular lesion or the collecting system with posterior stenosis [1, 9].
References
-
Kandarpa K, Machan L, Durham J (2016) Handbook of Interventional Ra diologic Procedures. Philadelphia: Lippincott Williams & Wilkins.
-
Agarwal SK, Sethi S, Dinda K (2013) Basic of kidney biopsy: A nephrologist´s perspective. Indian J Nephrol 23(4): 243-252.
-
Hart C, Ryu J (2002) Complications of percutaneous nephrostomy tube placement to treat nephrolitiasis. Hospital physician 43-46.
-
Ramchandani P, Cardella JF, Grassi CJ, Roberts AC, Sacks D, et al. (2003) Quality improvement guidelines for percutaneous nephrostomy. J Vasc Interv Radiol 14(9Pt 2): S277-S281.
-
Mandeep D, Parvati R (2011) Percutaneous Nephrostomy: Technical Aspects and Indications. Semin Intervent Radiol 28(4): 424-437.
-
Ahallal Y, Khallouk A, Jamal M, Hassan M (2010) Risk factor analysis and management of ureteral double J stent complications. Rev U ro l 12 (2-3): e147-e151.
-
Cronin C, Prakash P, Gervais D, Hahn P (2011) Imaging-Guided Suprapubic Bladder Tube Insertion: Experience in the Care of 549 Patients. AJR Am J Roentgenol 196(1): 182-188.
-
Sauk S, Suckerman D (2011) Renal artery embolization. Semin Intervent Radiol 28(4): 396- 406.
-
Mauri G, Nicosia L, Varano GM, Bonomo G, Della Vigna P, et al. (2017) Tips and tricks for a safe and effective imablInsights age-guided percutaneous renal tumour ablation. Insights Imaging 8(3): 357-363.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report