Cystolitholapaxy for a Large Bladder Calculi Using Semi-Rigid Ureteroscope through the Mitrofanoff Stoma
Bladder calculi are a common long-term complication of enterocystoplasty. Increasingly, mini-invasive techniques are taking the place of open cystolithotomy in the management of this patient category. Options include extra-coropreal lithotripsy, endoscopic management, percutaneous or combined technique using both endoscopic and laparoscopic approaches. Reports of Mitrofanoff cystolitholapaxy are rare and are not free from complications, the challenge is to obtain a free stone patient without compromising or the continence mechanism or inducing a mucosal lesion that could lead to the stenosis of the conduit. We report the case of a large neobladder calculi managed endoscopically using semi-rigid ureteroscope, which allowed a complete stone cleansing without damage to the Mitrofanoff conduit.
Introduction
Bladder calculi are a common complication of enterocystoplasty [1, 2]. Its treatment poses challenges especially in patients with an impassable or surgically ablated urethra. Endourological approach became cornerstone in the management of this situation but access can potentially traumatize a reconstructed tract; Achieving complete stone cleansing without damage to the conduit or the reconstructed bladder is real challenge in this patient category.
Case Report
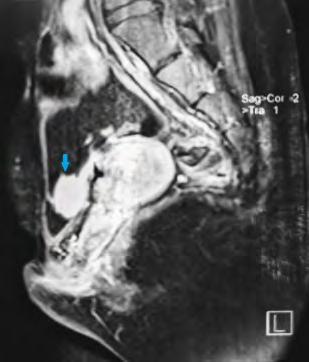
A 21-year-old woman with history of bladder extrophy, for which she had undergone an enterocystoplasty with bladder enlargement and mitrofanoff type bypass; She is under intermittent catheterization since the age of 6, and a vaginal reconstruction with labioplasty is planned for her; the patient presented with a one-year history of recurrent urinary tract infections, difficult self-catherization and a pelvic heaviness. The operative details of all her surgeries were not available to us. A pelvic MRI was performed, as part of surveillance, revealing a large neo-bladder calculi measuring 27x15 mm, ultrasound has shown no renal lithiasis or hydronephrosis and the creatinine clearance was normal (49 µmol/l), the calculi was radio-opaque on X-ray abdomen (Figure 1).

Physical examination of her abdominopelvic region revealed multiple scars, a catheterizable stoma, and an ablated urethra (Figure 2).

Technique and Results
Under general anesthesia, we proceeded to a first progressive dilation of the orifice of the mitrofanoff, which was punctiform, with a hegar dilator until 16 FR, then an introduction of a 9.5 CH semi-rigid ureter scope under visual control, neo-bladder exploration has shown no suspect lesion of the mucosa, the use of a 265 µm HOLMIUM Laser fiber down ureter scope permitted fragmentation of the stone using dusting mode then fragmentation which were then removed with the zero tip basket. The procedure took 95 minutes and rendered the patient completely stone free. She was discharged the next day (Figure 3).
Discussion
Bladder stones are one of the most common long-term complications seen in patients with enterocystoplasty [2]. Its incidence is up to 50% [3, 4] and its etiology is multifactorial [5] due essentialy to urinary stasis, bacteriuria, and mucous production [6]. The best treatment for vesical lithiasis is prevention by improving the standard of living, dietary measures and regular follow up [7]. Traditionally these stones are managed using either a transurethral, shockwave lithotripsy [8] or percutaneous approach [9, 10] .
Open cystolithotomy is traditionally used for large and multiple bladder stones but exposes the patient to an increased morbidity [11], complications of a prolonged hospital stay and surgical difficulties especially when repeat procedures are required for recurrent urolithiasis. However To avoid open surgery and in an already scarred abdomen, several techniques have been described using endoscopic, percutaneous [10, 11, 12] or combined approach [13].
To our knowledge, there has been no reported case of lithotricy on neobladder using exclusively semi-rigid ureteroscope through the MITROFANOF channel, the use of the ureteroscope offers the advantage of minimizing the risk of damaging channel continence mechanics by its low caliber, but could pose two technical difficulties: - The drainage of the irrigation fluid, in our case a discharge by vesical catheter 14 FR once in the middle of the gesture was sufficient, also the large volume of the neobladder allowed to continue the lithotricy while keeping a good visibility. - The risk of mucosal lesion when multiplying the entries for recovery of fragments, some authors have chosen the use of an access sheath as solution [14]. In our patient the use of dusting mode during lithotricy, minimized the number of entrances and exits and allowed the obtaining of sand and minimal fragments, but which slightly lengthened the duration of the surgery.
The use of a nephroscope [14] or a flexible cystoscope [15] has been described with the installation of an access sheath to maintain a continuous flow of irrigation but to the detriment of a larger caliber that may compromise the channel’s continence mechanism [16].
Conclusion
The endoscpic treatment of neobladder stones by rigid ureteroscope allowed a complete cleansing of lithiasis in our patient while avoiding the complications of percutaneous approach as well as those of open surgery.
Declaration of Patient Consent
We certify that we have obtained all appropriate patient consent forms. In the form the patient has have given her consent for her images and other clinical information to be reported.
We have explained to the patient that her name and initial will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
References
-
Welk B, Herschorn S, Law C, Nam R (2012) Population based assessment of enterocystoplasty complications in adults. The Journal of urology 188(2): 464-469.
-
Kisku S, Sen S, Karl S, Mathai J, Thomas RJ, et al. (2015) Bladder calculi in the augmented bladder: a follow- up study of 160 children and adolescents. Journal of pediatric urology 11(2): 66e 61-66.
-
Schlomer BJ, Copp HL (2014) Cumulative incidence of outcomes and urologic procedures after augmentation cystoplasty. Journal of pediatric urology 10(6): 1043- 1050.
-
Woodhouse CR, North AC, Gearhart JP (2006) Standing the test of time: long-term outcome of reconstruction of the exstrophy bladder. World journal of urology 24(3): 244-249.
-
Woodhouse CR, Robertson WG (2004) Urolithiasis in enterocystoplasties. World journal of urology 22(3): 215-221.
-
McDougal WS (1992) Metabolic complications of urinary intestinal diversion. The Journal of urology 147(5): 1199-1208.
-
Papatsoris AG, Varkarakis I, Dellis A, Deliveliotis C (2006) Bladder lithiasis: from open surgery to lithotripsy. Urological research 34(3): 163-167.
-
Kilciler M, Sümer F, Bedir S, Ozgök Y, Erduran D (2002) Extracorporeal shock wave lithotripsy treatment in paraplegic patients with bladder stones. International journal of urology 9(11): 632-634.
-
Paez E, Reay E, Murthy LN, Pickard RS, Thomas DJ (2007) Percutaneous treatment of calculi in reconstructed bladder. Journal of endourology 21(3): 334-336.
-
Hubsher CP, Costa J (2011) Percutaneous intervention of large bladder calculi in neuropathic voiding dysfunction. International braz j urol 37(5): 636-641.
-
Kronner KM, Casale AJ, Cain MP, Zerin MJ, Keating MA, et al. (1998) Bladder calculi in the pediatric augmented bladder. The Journal of urology 160(3 Pt 2): 1096-1098.
-
Miller DC, Park JM (2003) Percutaneous cystolithotomy using a laparoscopic entrapment sac. Urology 62(2): 333-336.
-
Lam PN, Te CC, Wong C, Kropp BP (2007) Percutaneous cystolithotomy of large urinary-diversion calculi using a combination of laparoscopic and endourologic techniques. Journal of endourology 21(2): 155-157.
-
Floyd MS, Sakalis V, Davies MC (2016) Mitrofanoff cystolitholopaxy and bladder biopsy using a mini-PCNL kit. Journal of Clinical Urology 10(1): 36-38.
-
Floyd MS, Stubington SR (2015) Mitrofanoff cystolitholapaxy: an innovative method of stone clearance in a hostile abdomen with an inaccessible urethra. Urology journal 12(2): 2115-2118.
-
Thomas JS, Smeulders N, Yankovic F, Undre S, Mushtaq I, et al. (2018) Paediatric cystolitholapaxy through the Mitrofanoff/Monti channel. Journal of pediatric urology 14(5): 433 e431-433 e434.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report