Comparative Study on the Use of Umbilical Vein Transplant Vs Buccal Mucosa Graft in Male Urethral Stricture
Urethral stricture in men is a common disease affecting males from one day to >80 year. The disease till date is poorly managed. Different methods have been proposed to plan the management of such patients. A systematic literature review and expert opinion were the basis of this article.
Introduction
Urethral strictures can be caused by varieties of disorders from congenital meatal stenosis to urethral valves urethral injuries, inflammatory conditions, iatrogenic situations in catheterization or therapeutic endoluminal surgery [1]. The surgical treatment has an overwhelming history and represents one of the oldest urological credentials to mankind [2].
Urethral stricture is one of the most difficult urological problems to definitively treat. The condition has been documented in the ancient literature from the Pharaohs, the Hindu scriptures and the Greek relics [1, 2]. Different techniques have been employed for the treatment of urethral strictures, depending on the stricture length, location, and depth of scar [3, 4] which include simple dilatation, urethrotomy, uroLume stent placement [5], urethroplasty and perineal urethrostomy [6].
Optical internal urethrotomy (OIU) is one of the most commonly used procedures for urethral stricture [7, 8, 9]. Data from the National Health Service in the UK during 2006 showed that OIU or urethral dilatation was used in 93% of cases and urethroplasty in 7% of cases [10]. Optical internal urethrotomy has the advantage of short learning curve, simplicity, speed, and short convalescence of patients. In 1957, Ravasini [11] described internal urethrotomy under direct vision and used electrocautery to incise the stricture, but it was not until 1971 that Sachse [12] introduced the sharp-bladed cold-knife urethrotome under direct vision, reporting 80% success rate with the procedure in 1974.
Further technological advances have been utilized. Lasers have been used for the treatment of urethral strictures since 1977 [13] the types of lasers [5] that have been used for urethrotomy include carbon dioxide, Nd: YAG, the KTP, Argon, and the Ho: YAG and excimer lasers. No superiority of one type of laser has been demonstrated [14] Holmium: YAG [5] is a new introduction in the range of laser modalities available; it provides both direct contact cutting and vaporization with minimal retropulsion.
Substantial clinical observations indicate that the umbilical vein is an excellent source of stem cell when used with its covering Wharton’s jelly. The umbilical vein is an inert tissue capable of obtaining nutrients by diffusion for the first 6 weeks of implantation and is a very good and economical source of urethral implantation (33, Klippel 1977). Klippel demonstrated the use of umbilical vein xenografts from different species in 1977. Al-Naib [9] in his experimental study used the umbilical vein in homologous autologous grafts with excellent results [9].
Aim of the Study
The aim of this study is to compare the Use of Umbilical vein with Buccal mucosa as a urethral graft with assessment of the outcomes of patients irrespective of the length and location of the stricture.
Patients Data
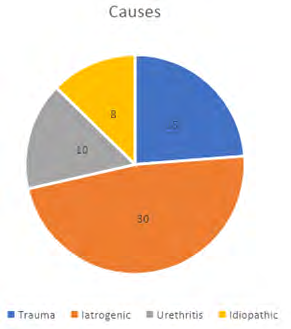
Between August 2001 and 2018, this retrospective randomized study was conducted in Medical city teaching hospital Baghdad and King Hamad university Hospital Bahrain. A total of 63 patients aged between 26 and 69 years (mean age ± standard deviation: 45.1 ±7.1 years) were included in the study. There was no significant difference between the mean ages of the treatment groups, which were 54.8 ±-9.5 years for OIU (n = 29) and 55.3 ±8.9 years for laser internal urethrotomy (n = 34) (p = 0.895). Of the 63 patients, 59 (93.7%) were married. Urethral stricture was iatrogenic in 42 (66.7%) patients, secondary to trauma in 12 (19%), secondary to urethritis in 6 (9.5%), and idiopathic in 3 (4.8%) patients.
There were no significant differences between the mean age, marital status and preoperative Qmax values between the two groups (p >0.05 for all comparisons). The demographic features and aetiology of the strictures are present in Table 1. Patients were randomized to receive umbilical vein graft (n=33) or buccal mucosal graft (n=30) (Figure 1).
| Min-Max | Median | Mean | |
|---|---|---|---|
| Operation Time | 1 h-2:30 h | 180 min | 1.44 h |
| Complication | 5 (6.7%) | ||
| Preoperative | 5.7-6.8 | 6.2 | 6.3 |
| After 3M | 18-20 | 18.45 | 17.2 |
| After 6M | 17.1-19.3 | 18.8 | 18.1 |
| After 12M | 18-19.1 | 18.4 | 18.2 |
Table 1: The demographic features and etiology of the strictures are present.
Data
All patients underwent a complete physical, radiological and blood tests including ABO and Rh testing. Radiological investigations were tailored to patient condition but included a urethrogram to assess the stricture state. Patients with infected urine will be treated with appropriate antibiotics.
Technique of preparing umbilical vein: In an appropriate patient requiring a urethroplasty, after ensuring sterile urine. An ABO and Rh compatible umbilical vein is collected by the labour room team/ Obstetrics team. 1. During Normal Vaginal delivery or an elective caesarean section, the umbilical cord is maintained in a sterile manner.
2. The umbilical cord is delivered to the urology theatre sterile in 0.9% buffered Normal Saline.
3. The cord can be stored in liquid nitrogen in temp. of -196 Celsius for up to 12 months.
In the urology theatre, the umbilical vein is dissected on the back table of the urology theatre. Care is taken to leave 1-2mm from the Wharton jelly margin. 10 Fr. Catheter is used to splint the umbilical vein when fully dissected. The umbilical vein is then bathed in a solution of Gentamicin 160 mg and Cisplatin solution for 1 hour. This aims to eliminate all donor antigenic leukocytes. This is based on the hypothesis that the umbilical vein is an inert structure and has no vasa vasorum and therefore easy to eliminate the antigenic cells from its mucosa. Twenty centimetres of the vein with its Wharton’s jelly delivered to the operation field.
Intraoperatively the desired length of the vein is calculated to bridge the length of the stricture. Care is taken to ensure over coverage of 2mm proximal and distal end when anastomosed to the healthy urethra, as the urethral- umbilical vein anastomotic site tend to shrink longitudinally [1] The vein is opened and anastomosed proximally and distally to the healthy urethra using interrupted absorbable synthetic suture.
All patients received 40 mg hydrocortisone for 3 days intravenously and 10 days of 20 mg methylprednisolone orally to induce immunosuppression. All patients received nitrofurantoin for 6 weeks postoperatively with an indwelling catheter kept in place. After catheter removal uroflowmetry was performed.
Neopterin in urine was measured in 6 weeks and 3 months to detect early rejection. Neopterin is a sensitive marker of increased activity of cellular immunity in humans and therefore early rejection can be diagnosed. The neopterin in urine detects the increased lymphocytic population before the full picture of rejection is clinically evident [11, 12, 13, 14].
In conditions when the umbilical vein needed to be stored. The vein will be washed with buffered saline solution and immersed in a mixture of gentamicin and cisplatin for one hour and stored in liquid nitrogen at a temperature of –196 degree Celsius.
Results
In 1985 after extensive animal study, implantation under Local anaesthesia of the umbilical vein in the thigh of Professor K.F. Klippel in Celle Germany 1985, which showed no evidence of rejection after 6w of implantation. (Figure 2) demonstrated the histopathology results after removing the vein with its Wharton’s jelly.
Results of the two groups
Umbilical Vein Group
No rejection was demonstrated in the UV group. No significant difference in both groups in Qmax (p >0.05) after
3 and 6 months. After the 12 months period urethroscopy was performed for 15 patients with urinary symptoms, Qmax <12 ml/sec. 10 patients with BMU and 5 with UVU.
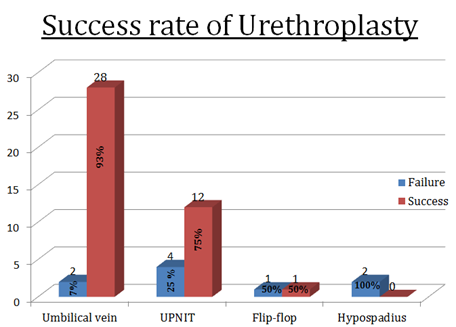
The Umbilical vein transplant patients demonstrated a 90%% success rate of resolution of urethral obstruction, while the Buccal mucosa patients did slightly less with a success rate of only 80% (P = 0.002; Fisher’s exact test). Buccal mucosa group With 33 patients underwent buccal mucosa grafting and anastomosis 13 patients developed failure of achieving an adequate flow rate. 5 patients developed urethro-cutaneous fistula which was repaired at 6 weeks. 4 developed Recurrent strictures after 9 months with severe obstruction and flow of 4-6 ml/sec, redo operation was performed. The site of the stricture was the graft-urethral anastomotic sites. Three fistulae were treated conservatively (Figure 3).

The postoperative hospital stay was equal for Umbilical vein group and buccal mucosa group. UV and BM groups average operation time was 2:45 and 2:00 hours respectively.
Discussion
The aim of this study is to improve and refine the available surgical procedures for management of recurrent strictures. We aimed to improve the outcomes and better delineate patients who will benefit from various interventions.
One of the oldest procedures in Urology is Urethral dilation [1]. Urethral dilatation use has been trending down since the appearance of visual internal urethrotomy [3]. Researchers converging strategy on CISC (Clean Intermittent Self catheterization) [4]. With urethral dilation, high recurrence rate is expected, with possibility of further fibrosis. The postulated method is that dilation causes rupture of the urethral mucosa in the whole circumference of the urethra which consequently leads to extravasation of the urine to submucous layers and causing more inflammatory response leading to stricture and fibrosis [4, 5].
Steenkamp, et al. [1] pointed out no statistical difference in outcome between VIU and UD. However, there were severe and frequent recurrences induced by UD (urethral dilation), haemorrhage and severe infection [2, 5, 6].
More commonly, optical urethrotomy or Visual Internal Urethrotomy (VIU) is performed. [7]. This is since the learning curve of VIU is very short compared to intrinsic surgical procedures that have a long learning curve with specialized centres and expertise being needed [1, 6, 7]. The VIU is reserved for short strictures (≤1.5 cm) [1]. Steenkamp, et al. [1] shown, that everyone cm longer stricture brings extra risk factor (RR:1.22) for recurrence of stricture. Even though repetitive frequent self-dilation or hydraulic self- dilation or office dilation by urologists have been utilized. Evidence of these adjunct procedures (self-dilation or hydraulic-self dilation) might benefit slightly from repeated recurrences, but data failed to specify patient sub- groups that will benefit from such practices and, at the same time pointed out that it is associated with poor quality of life [1, 2].
The use of corticosteroids post urethrotomy injection or installation has been evaluated by 4 studies [1, 12, 13, 14, 15]. All these studies are limited to strictures less than 2 cm and based on poor quality studies, therefore no clear conclusions about true valves of corticosteroids can be contemplated [1]. Low dose of Mitomycin C (MMC) (0.1mg in 2 ml., 5% solution) injection in the freshly operated urethrotomy. The MMC dose is effective in its activity as an antifibrotic and anticollege formation property [16]. Serious side effects from extravasation of MMC in the incised area leading to severe immune reaction with fibrosis and subepithelial reaction with subsequent urethral strictures [17]. Although the concentration is low this procedure did not find its way in routine practice, but recent studies confirmed the benefit of adding MMC injection over VIU alone [1, 2, 4, 18].
The use of metallic stents did not gain wide acceptance in general practice. Metallic stents are good for short term use; their use showed an overwhelming complication rate with severe obliteration and encrustation of the stent to the degree of total blockages and retention. [1, 19].
Laser evaporation is used in the form of holmium laser due to its minimal destruction of the urethral [20] mucosa and fast re-epithelialization, but it is currently recommended for short urethral stricture [2]. Its recurrent rate for short strictures within a year is less than VIU [2].
Surgical Techniques
Many procedures for management of urethral stricture disease are described in the literature. None of the described surgeries achieved ease of use, generalizability, and short learning curve with high success rate. Many procedures under different surgeons’ names are listed in literature Das S [2]. This is because none are ideal but with variable success rates.
- End-to-end anastomosis in fact, it is excision and end to end anastomosis (EPA), this procedure has the highest success rate [2]. If a bulbar urethral length is 10 cm, a stricture of 2 cm or less can be safely connected. Further length can be reached by proximal and distal mobilization of the healthy urethra. However, if a gap is still present a graft is required to bridge the stricture [4]. Bulbo-prostatic anastomosis can be created in patients with prostate cancer post radiation therapy with severe fibrosis [1, 2].
- Staged urethroplasty as adopted by Sir Blandy is an option aiding posterior or even proximal bulbar strictures [1, 4].
- End to end urethroplasty must be avoided and contraindicated due to the high possibility of shortening and chordae as recommended by The International Consultation of Urologic Diseases (ICUD) [5].
- Free graft urethroplasty is a logical answer to all the above procedures, it represents the easiest and versatile technique from the meatus to the posterior urethra [21].
- Buccal mucosa or preputial graft one has similar outcomes [22]. Wesley verla, et al. stated that buccal mucosa is not free of complications and the learning curve is also long and tedious. The complications include donor site pain, difficulty eating, taste loss and difficulty in opening the mouth. Persistent pain and discomfort which leads to prolonged hospital stay and consequently cost [22, 23]. Buccal mucosal grafting is an essential part of the urological inventory in urethral stricture disease management.
- Free urethral graft basically is placed ventrally along the opened urethral stricture area, but posterior onlay or both can also be used (72). It is assumed that posterior onlay is more successful due to better vascularity of the corpora, than ventral onlay where the graft will depend on its vascularity from subcutaneous tissue only [1].
- Pedicled flaps are an excellent option from meatus to posterior urethral stricture. Still complications like sacculation, intraurethral hair growth depending on the type of graft used. However, it should not be considered as first choice option [1, 23].
- Multistage urethroplasty is an outstanding procedure, recently this lengthy procedure is mostly reserved for recurrent urethral stricture. The drawbacks are the prolonged duration of catheterization and possibility of graft failure [24].
- Permanent perineostomy of urethra. Some old patient and recurrent failure cases, prefer this option as they can void freely and without pain, Sir Blandy U shaped incision is the procedure of choice with very good results [1, 25].
- Stricture after radical prostatectomy with or without radiation, due to the development of fibrosis and diminished vascularity at the bladder-urethral anastomosis site, end to end anastomosis is the treatment of choice nowadays [1].
This is since most of the strictures are short and near the bladder neck [26].
Conclusion
In conclusion the umbilical vein is an excellent option for urethral stricture. Umbilical vein carries many advantages including; no vasa-vasorum resistant to urine, no extravasation, inert with no antigenic structure, economical and widely available. The umbilical vein can nourish itself in the first 6 weeks by diffusion only reducing the risk of ischemic graft contractures [2].
The umbilical vein fulfilled the requirement of an excellent urethral transplant in recurrent and long urethral strictures. Further studies with randomized, blinded controlled trials can shed more information and the possibility to consider it as a first line option in open urethral surgeries for strictures.
References
-
Peterson AC, Webster GD (2004) Management of urethral stricture disease: Developing options for surgical intervention. BJU Int 94(7): 971-976.
-
Das S (2007) Urology in ancient India. Indian J Urol 23(1): 2-5.
-
Tavakkoli Tabassi K, Yarmohamadi A, Mohammadi S (2011) Triamcinolone injection following internal urethrotomy for treatment of urethral stricture. Urol J 8(2): 132-136.
-
Singh O, Gupta SS, Arvind NK (2011) Anterior urethral strictures: A brief review of the current surgical treatment. Urol Int 86(1): 1-10.
-
Wilson TS Lemack GE, Dmochowski RR UroLume stents: lessons learned. J Urol 167(6): 2477-2180.
-
DeLong J, McCammon K, Capiel L, Rovegno A, Tonkin JB, et al. (2017) Augmented perineal urethrostomy using a dorsal buccal mucosal graft, bi-institutional study. World J Urol 35(8): 1285-1290.
-
Ghosh B, Dorairajan LN, Kumar S, Manikandan R, Muruganandham K, et al. (2013) Randomized clinical trial comparing effectiveness of intra corpus spongiosum block versus topical anesthesia for performing visual internal urethrotomy for urethral stricture disease. Urology 81(1): 204-207.
-
Kumar S, Prasad S, Parmar K, Ganesamoni R, Batra YK (2012) A randomized controlled trial comparing combined spongiosum block and intraurethral lignocaine with intraurethral lignocaine alone in optical internal urethrotomy for urethral stricture. J Endourol 26(8): 1049-1052.
-
Dubey D (2011) The current role of direct vision internal urethrotomy and self-catheterization for anterior urethral strictures. Indian J Urol 27(3): 392-396.
-
Heyns CF, van der Merwe J, Basson J, van der Merwe A (2012) Treatment of male urethral strictures-possible reasons for the use of repeated dilatation or internal urethrotomy rather than urethroplasty. S Afr J Surg 50(3): 82-87.
-
Smith P, Dunn M, Dounis A (1978) Sachse optical urethrotome in management of urethral stricture in the male: Preliminary communication. J R Soc Med 71(9): 596-599.
-
Saavedra-Briones DV, Merayo-Chalico CE, Sanchez- Turati G, Cantellano-Orozco M, Shuck-Bello C, et al. (2009) Urethral stricture recurrence following internal urethrotomy. Rev Mex Urol 69(4): 153-158.
-
Jabłonowski Z, Kedzierski R, Miekoś E, Sosnowski M (2010) Comparison of neodymium-doped yttrium aluminum garnet laser treatment with cold knife endoscopic incision of urethral strictures in male patients. Photomed Laser Surg 28(2): 239-244.
-
Herrmann TR, Liatsikos EN, Nagele U, Traxer O, Merseburger AS, EAU Guidelines Panel on Lasers, Technologies (2012) EAU Guidelines on Laser Technologies. Eur Urol 61(4): 783-795.
-
Atak M, Tokgoz H, Akduman B, Erol B, Donmez I, et al. (2011) Low-power holmium: YAG laser urethrotomy for urethral stricture disease: Comparison of outcomes with the cold-knife technique. Kaohsiung J Med Sci 27(11): 503-507.
-
Dutkiewicz SA, Wroblewski M (2012) Comparison of treatment results between holmium laser endourethrotomy and optical internal urethrotomy for urethral stricture. Int Urol Nephrol 44(3): 717-724.
-
Kamal BA (2002) The use of the diode laser for treating urethral strictures. BJU Int 87(9): 831-833.
-
Hussain M, Lal M, Askari SH, Hashmi A, Rizvi SA (2010) Holmium laser urethrotomy for treatment of traumatic stricture urethra: A review of 78 patients. J Pak Med Assoc 60(10): 829-832.
-
Jin T, Li H, Jiang LH, Wang L, Wang KJ (2010) Safety and efficacy of laser and cold knife urethrotomy for urethral stricture. Chin Med J (Engl) 123(12): 1589-1595.
-
Santucci R, Eisenberg L (2010) Urethrotomy Has a much lower success rate than previously reported. J Urol 183(5): 1859-1862.
-
Iselin CE, Webster GD (1998) Dorsal onlay urethroplasty for urethral stricture repair. World J Urol 16(3): 181-185.
-
Pansadoro V, Emiliozzi P, Gaffi M, Scarpone P (1999) Buccal mucosa urethroplasty for the treatment of bulbar urethral strictures. J Urol 161(5): 1501-1503.
-
Pansadoro V, Emiliozzi P, Gaffi M, Scarpone P, DePaula F, et al. (2003) Buccal mucosa urethroplasty in the treatment of bulbar urethral strictures. Urology 61(5): 1008-1010.
-
Barbagli G, Lazzeri M (2006) Urethral reconstruction. Curr Opin Urol 16(6): 391-395.
-
Myers JB, McAninch JW (2011) Perineal urethrostomy. BJU Int 107(5): 856-865.
-
Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA (2012) Philadelphia: Elsevier Saunders. 10th (Edn.), Campbell-Walsh Urology, pp: 967-973.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report